"Safety and Efficacy of Vitamin D Supplementation in Patients With Allergic Rhinitis: Randomized Double Blind Placebo Control Study in Mexican Population”
Received Date: March 11, 2023 Accepted Date: April 11, 2023 Published Date: April 14, 2023
doi: 10.17303/aicb.2023.1.103
Citation: Elisa Ortega Jordá Rodríguez, Daniela Rivero Yeverino, Aída Inés López García, Chrystopherson Gengyny Caballero López, Juan Jesús Ríos López, Dr. José Sergio Papaqui Tapia. Ann Immunol Cell Biol 1: 1-8
Abstract
The severity of allergic rhinitis has been related to low levels of vitamin D and its supplementation could have a positive impact on the severity of symptoms. In this randomized double blind placebo control study, we aimed to evaluate the safety of supplementation with cholecalciferol versus placebo in patients with allergic rhinitis and vitamin D insufficiency or deficiency, and its impact on symptom's severity and serum 25 (OH)D levels. The experimental group received 5,000 IU of cholecalciferol daily for 60 days and the control group received placebo. Follow- up was performed with Total Nasal Symptom Score (TNSS) and serum vitamin D levels. The mean serum Vitamin D level went from 18.10 ng/ml to 44.94 ng/ml, with no difference in the placebo group. The mean TNSS in the active group went from 7.16 to 2.58 (p<0.029). There were no toxicity levels or adverse events. Supplementation of cholecalciferol is safe, and it can be considered an adjuvant in the management of patients with AR and vitamin D deficiency and insufficiency, improving their quality of life.
Keywords: Allergic Rhinitis; Deficiency; Insufficiency; Supplementation; Vitamin D
Introduction
Allergic rhinitis is an inflammatory disease of the nasal mucosa mainly mediated by immunoglobulin E, caused by exposure to allergens and characterized by the presence of one or more of the following symptoms: nasal itching, rhinorrhea, nasal obstruction, and sneezing. With a great impact on both health and quality of life deterioration, as well as on productivity, involving high costs. [1] Its worldwide prevalence has increased over the last 30 years, currently reported at 15-25%. [2]
Vitamin D3 or cholecalciferol is the main dietary source of vitamin D and it is present mostly in foods of animal origin, nevertheless, around 80% of vitamin D3 is produced endogenously in the skin from 7- dehydrocholesterol by the action of UV light. Cholecalciferol and ergocalciferol (vitamin D2), undergo 25-hydroxylation in liver to 25(OH)D (calcidiol), the major circulating form. Then it is converted in kidneys through 1-alpha-hydroxylation to its most active form, 1,25(OH)2D (calcitriol). In the innate immune system, 1,25-OH-D increases chemotaxis, autophagy, phagolysosome fusion, defensin and cathelicidin production by macrophages, monocytes and keratinocytes. In the adaptive immune system, it causes inhibition of the production of proinflammatory cytokines. In monocytes and macrophages, it decreases the expression of major histocompatibility complex class II (MHC II) molecules, CD80/86, decreasing antigen presentation. In dendritic cells, it inhibits the production of IL-12 and IL-23 and stimulates the production of IL-10. It modulates the response of T lymphocytes, decreasing their proliferation, inducing apoptosis of autoreactive lymphocytes, and increasing regulatory T lymphocytes, FoxP3 and cytotoxic T lymphocyte antigen (CTLA 4). (Figure 1) [3-6]
The prevalence of vitamin D deficiency in children and adults has increased exponentially in recent years, making it a global epidemic, related to overweight, sedentary lifestyles, decreased intake, gastrointestinal diseases, deficient absorption, renal and hepatic pathologies. Guidelines published by the Endocrine Society on vitamin D defined vitamin D deficiency as 1,25-OH-D <20 ng/mL, insufficiency as 21-29 ng/mL, and suffi-ciency as at least 30 ng/mL for maximum skeletal muscle health. [7] In Europe, it is estimated that more than 40% of the population has deficiency, 13% being severe. In the U.S. population aged 1 to 21 years, 61% had insufficiency and 9% deficiency. In Mexico, the prevalence of deficiency and insufficiency in children is 16% and 23% respectively, while in the adult population, deficiency was 9.8% and insufficiency 20%. [8]
There is currently no international consensus on the supplementation of this vitamin. The dose of 25 mcg (1000 IU) increases the serum level of 1,25-OH-D by an average of 15 to 25 nmol/L. [9] According to the Endocrine Society, the daily dose of 10,000 IU of vitamin D should not be exceeded; even with this dose, no adverse reactions occurred in healthy adults. [10] Cholecalciferol supplementation has been shown in several studies to have a positive impact on the clinical outcome of the patient. A study in Australia showed that low vitamin D levels at age 6 years were predictive of increased risk of asthma and sensitization to aeroallergens at age 14 years. [11] It has been reported that low levels of vitamin D correlated with severity of allergic rhinitis, and after supplementation there was a decrease in the TNSS score, an improvement attributed to the immunomodulatory effects of vitamin D. [12] Our group has previously reported that vitamin D supplementation, in patients with allergic rhinitis, with 6000 IU weekly for adults and 5000 IU weekly for children improves symptomatology. However, it does not demonstrate an increase in serum 25-OH-D concentrations. [13]
The aim of this study was to evaluate the efficacy of supplementation with 5000 units of cholecalciferol in patients with allergic rhinitis and insufficiency or deficiency of Vitamin D, to describe the relationship between the severity of allergic rhinitis symptoms and vitamin D levels after it's supplementation. In addition, the safety of this intervention was evaluated by assesing possible adverse effects related to vitamin D and by monitoring its serum levels.
Materials and Methods
Randomized, double-blind, placebo-controlled, experimental study involving pa-tients aged 10 to 40 years who attended the Allergy and Clinical Immunology service of the University Hospital of Puebla, Mexico, during the period from October 2020 to July 2021, with a diagnosis of allergic rhinitis, confirmed by skin tests or specific serum IgE. Patients with pathologies that alter the metabolism, absorption or excretion of cholecal-ciferol, patients pregnant or breastfeeding, and patients under treatment with cortico-steroids, antiepileptic drugs and vitamin D supplements in the previous 3 months were excluded from the study.
Patients were randomly divided into two groups in a double-blind design. Randomization sequence was created using Excel for Microsoft 365, participants were randomly assigned to 1 of 2 treatment groups (active or placebo). The placebo group received pharmacological treatment (fluticasone furoate 27.5 mcg once a day for two months), subcutaneous immunotherapy and placebo. On the other hand, patients in the active group received the same dose of fluticasone furoate, subcutaneous immunotherapy and cholecalciferol 5000 IU or 714 IU/day for 8 weeks
Severity of allergic rhinitis symptoms was assessed at study entry, 30 days, and 60 days later using the TNSS. 25(OH)D levels were quantified at baseline and at the end of the study by particle chemiluminescent immunoassay with ARCHITECT i1000SR equipment.
During follow-up, the presence of symptoms and signs of adverse effects of vitamin D supplementation was questioned at one month of follow-up and at the end of supplementation
Statistical analysis
Data were collected and organized in Microsoft Excel. Descriptive summary statistics were used by determining averages, percentages, and frequencies. A comparison of two averages was considered with a bilateral hypothesis, 95% confidence level, and an expected loss ratio of 20%. Statistical analysis of the data was performed with the IBM® SPSS® Statistics 28 program by means of a comparison of means using Student's t-test considering a significance value < 0.05.
All procedures during the present study were performed in accordance with the ethical norms, the Regulations of the General Law of Health, on Health Research and the Declaration of Helsinki. All participants expressed their authorization through informed consent and assent.
Results
Thirty-six patients with allergic rhinitis and vitamin D deficiency and insufficiency were included. The experimental group, which received vitamin D3, included 19 patients (52.78%),10 males and 9 females aged 10-40 years (SD 12.2). The control group included 17 patients (47.25%), 8 men and 9 women between 13 and 40 years of age (SD 9.6). When comparing both groups with respect to gender and age, no statistically significant differences were found between them (p> 0.05).
Serum 25(OH)D levels
The mean value of serum 25(OH)D levels at baseline in the placebo group was 20.32 ng/ml and in the active group 18.10 ng/ml. At 8 weeks of follow-up, the placebo group presented a mean vitamin D level of 21.38 ng/ml even with deficiency and in the active group it was 44.94 ng/ml reaching sufficiency. A statistically significant difference was shown between the initial value and at 8 weeks after treatment, with a mean increase of 26.83. (p=<0.05). (Figure 2) Within the active group, patients between 10 and 20 years old presented a mean serum 25(OH)D elevation of 34.6 ng/ml, while in the 20 to 40 years old age group the mean was 19.7ng/ml.
Severity of symptoms
The mean nasal symptom score (TNSS) at baseline was 6.47 in the placebo group and 7.16 in the active group. Consequently, no significant differences were observed between the two groups with respect to this variable (p= 0.277). The improvement in mean TNSS at the end of the study was lower in the placebo group (6.47 to 3.94) than the active group (7.16 to 2.58) and this difference between groups was statistically significant p<0.029
Safety of supplementation with cholecalciferol
None of the participants presented toxicity levels (> 150 ng/ml) or adverse events related to cholecalciferol supplementation, therein the risk of total adverse events was not increased in vitamin D supplemented arm compared with placebo.
Discussion
In recent years, multiple investigations have been performed analyzing the relationship between serum vitamin D value and the incidence and severity of allergic diseases.
There are multiple clinical trials evaluating the effects of cholecalciferol supple-mentation and correction of cholecalciferol levels with doses ranging from 800 IU to 7000 IU daily, showing efficacy and safety at low doses (800-1000 IU). [14-22]. However, the safety and incidence of adverse effects associated with it are rarely analyzed.
In the present study, the efficacy and safety of vitamin D supplementation in children older than 10 years old and adults with 5,000 units daily for 60 days was analyzed, none of the participants presented adverse events associated with the supplementation, in addition, at the end of the study, there was highly significant improvement in the total nasal symptom score in the active group compared to the placebo group, all participants within the active group, significantly decreased their symptoms and reached sufficiency levels with the mentioned dose without presenting toxicity levels (> 150 ng/ml). These results agree with the proposal of Khan et al., that a daily dose of 4000 to 5000 IU of vitamin D2 or vitamin D3 per day is required to reach levels of 40 to 60 ng/ml 23, and similarly with the safety studies of Bischoff-Ferrari et al. where there were no adverse reactions associated with intakes of up to 50,000 IU per day. [24-26]. Another study previously conducted at the University Hospital of Puebla, proved the clinical efficacy of supplementation with 5000 IU weekly for children and 6000 IU for adults for 8 weeks, however no significant sufficiency levels were achieved in the experimental group [13].
Bakhshaee et al. demonstrated that supplementation with 50,000 IU cholecalciferol every week for 2 months in patients with AR and vitamin D deficiency resulted in a significant difference between the initial and final nasal symptom severity score measured by TNSS (P = 0.007). [27]. Other placebo-controlled studies have used lower doses of cholecalciferol, 1000 IU daily, in shorter periods of time, 21 and 30 days, obtaining the same reduction in the total score of nasal symptoms (P < 0.05). [28, 29]. Patients aged 10 to 20 years’ old who received vitamin D supplementation showed an elevation of serum levels 1.75 times higher than patients aged 20 to 40 years old, which is consistent with that described in studies of fixed-dose supplementation in children and adults, where the elevation of serum levels is more significant in children and the elderly. [3, 30].
Conclusion
This study supports the evidence about the association between vitamin D deficiency and allergic rhinitis. Results shown here, remark the importance of assessing vitamin D levels in allergic rhinitis patients, to provide vitamin D supplementation along with standard treatment in deficient subjects. Funding: This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Hospital Universitario de Puebla. Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest: The authors declare no conflict of interest.
- Passali D, Cingi C, Staffa P et al. (2018) The International Study of the Allergic Rhinitis Survey: outcomes from 4 geographical regions. Asia Pacific Allergy 8: 1-15.
- Brozek JL, Bousquet J, Agache I et al. (2016) Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines. J Allergy Clin Immunol 140: 950-57.
- Hanel A, Carlberg C (2020) Vitamin D and evolution: Pharmacologic implications. Biochem Pharmacol. 2020;173(1):113-25.
- Sassi F, Tamone C, D'Amelio P (2018) Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients. 10: 1656-60.
- Martens PJ, Gysemans C, Verstuyf A et al. (2020) Vitamin D’s Effect on Immune Function. Nutrients 12: 1248-62.
- Charoenngam N, Holick MF (2020) Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 12: 20-97.
- Holick MF, Binkley NC, Bischoff-Ferrari HA et al. (2011) Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 96: 1911-30.
- Khayyatzadeh SS, Bagherniya M, Abdollahi Z et al. (2019) What is the best solution to manage vitamin D deficiency? IUBMB Life 71: 1190-97.
- Flores M, Sánchez-Romero LM, Macías-Lozada A et al. (2011) Concentraciones séricas de vitamina D en niños, adolescentes y adultos mexicanos. Resultados de la ENSANUT 2006. Instituto Nacional de Salúd Pública. 1: 1-27
- Amrein K, Scherkl M, Hoffmann M et al. (2020) Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr 85: 1-16.
- Agostoni C, Bresson JL, Fairweather-Tait S et al. (2012) Scientific Opinion on the Tolerable Upper Intake Level of vitamin D. EFSA Journal 10: 1-45.
- Hollams EM (2012) Vitamin D and atopy and asthma phenotypes in children. Curr Opin Allergy Clin Immunol. 12: 228-34.
- Balakrishnan M, Charanjeet K, Harsh V et al. (2015) Placebo controlled trial of Vitamin D supplementation in Allergic Rhinitis. European Respiratory Journal 46: 1-8.
- Payan-Díaz JH, Rivero-Yeverino D, López-García AI et al. (2020) Efecto terapéutico de la suplementación de vitamina D en pacientes con rinitis alérgica: ensayo clínico aleatorizado frente a placebo. Tesis para obtener el Diploma de especialista en Alergia e Inmunología Clínica, Benemérita Universidad Autónoma de Puebla.
- Gil Á, Plaza-Diaz J, Mesa MD (2018) Vitamin D: Classic and Novel Actions. Ann Nutr Metab 72: 87-95.
- Hawrylowicz CM, Santos AF (2020) Vitamin D: can the sun stop the atopic epidemic? Curr Opin Allergy Clin Immunol 20: 181-7.
- Özdemir Ö, Karavaizoğlu Ç (2018) Role and Importance of Vitamin D in Asthma and Other Allergic Diseases. JAREM 8: 1-8.
- Rosser FJ, Han YY, Forno E et al. (2021) Effect of vitamin D supplementation on total and allergen specific IgE in children with asthma and low vitamin D levels. J Allergy Clin Immunol S0091- 6749: 00902-7.
- Urquiza C, Fernández de Córdova JC, Velasco A et al. (2020) Prevalence of Vitamin D deficiency and associated factors in Mexican patients with allergic rhinitis and asthma. Rev. med. Hosp. Gen. Mex 83: 113-9.
- Chang SW, Lee HC (2019) Vitamin D and health - The missing vitamin in humans. Pediatr Neonatol 60: 237-44.
- Plesa M, Gaudet M, Mogas A et al. (2021) Vitamin D3 Attenuates Viral-Induced Inflammation and Fibrotic Responses in Bronchial Smooth Muscle Cells. Front. Immunol 12: 1-12.
- Amorim CLG, Oliveira JM, Rodrigues A et al. (2020) Vitamin D: association with eosinophil counts and IgE levels in children with asthma. J Bras Pneumol 47: 1-4.
- Gaude G, Kummarganti S, Hattiholi (2020) Clinical Effects of Vitamin D on the Control of Bronchial Asthma- Is It Relevant? J Clin of Diagn Res 14: 1-4.
- Khan QJ, Fabian CJ (2010) How I treat vitamin d deficiency. J Oncol Pract 6: 97-101.
- Rizzoli R (2021) Vitamin D supplementation: upper limit for safety revisited? Aging Clin Exp Res 33: 19-24.
- Heaney RP, Davies KM, Chen TC et al. (2003) Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am J Clin Nutr 77: 204-10.
- Bischoff-Ferrari HA, Shao A, Dawson-Hughes B et al. (2010) Benefit-risk assessment of vitamin D supplementation. Osteoporos Int 21: 1121-32.
- Bakhshaee M, Sharifian M, Esmatinia F et al. (2019) Therapeutic effect of vitamin D supplementation on allergic rhinitis. Eur Arch Otorhinolaryngol 276: 2797-801.
- Modh D, Shah P, Thakkar B et al. (2014) Role of vitamin D supplementation in allergic rhinitis. Indian J Allergy 28: 35-9.
- Menon B, Kaur C, Vardhan H et al. (2016) Placebo controlled trial of Vitamin D supplementation in Allergic Rhinitis. Research 3: 1501-15.
- Holick MF (2017) The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord 18: 153-65.
FIGURE 1
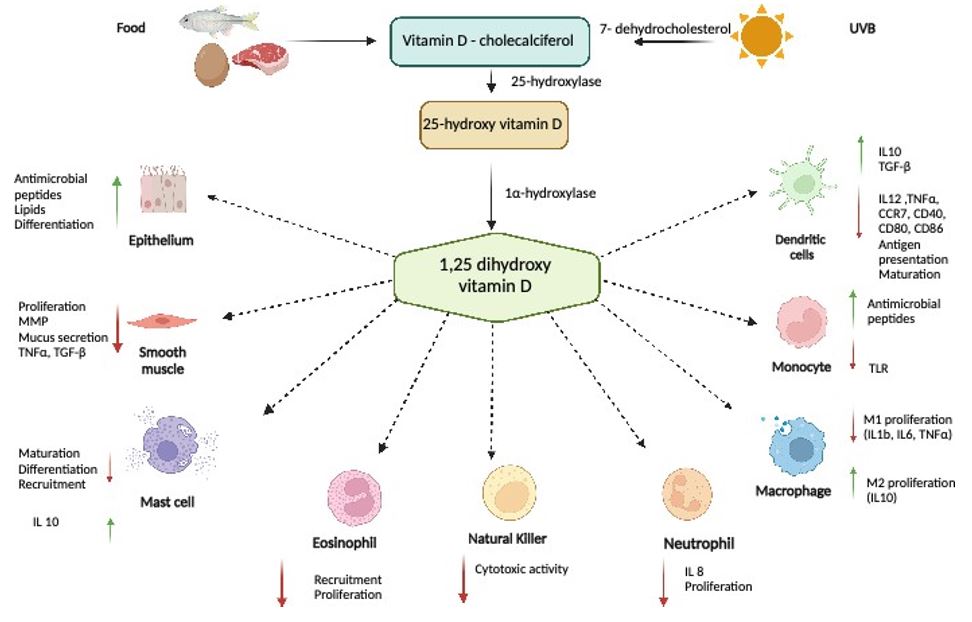
Figure 1: Vitamin D is a fat-soluble vitamin. Few foods naturally contain vitamin D, so dermal synthesis after UVB radiation remains the major route to obtain vitamin D. 7-dehydrocholesterol in skin epidermal cells is converted after UVB radiation into pre-vitamin D. Both vitamin D3 and undergo further enzymatic conversion to its active forms. First, it undergoes 25-hydroxylation in liver to 25(OH)D (calcidiol), then it is converted in kidneys through 1-alpha-hydroxylation to its most active form, 1,25(OH)2D (calcitriol)
FIGURE 2
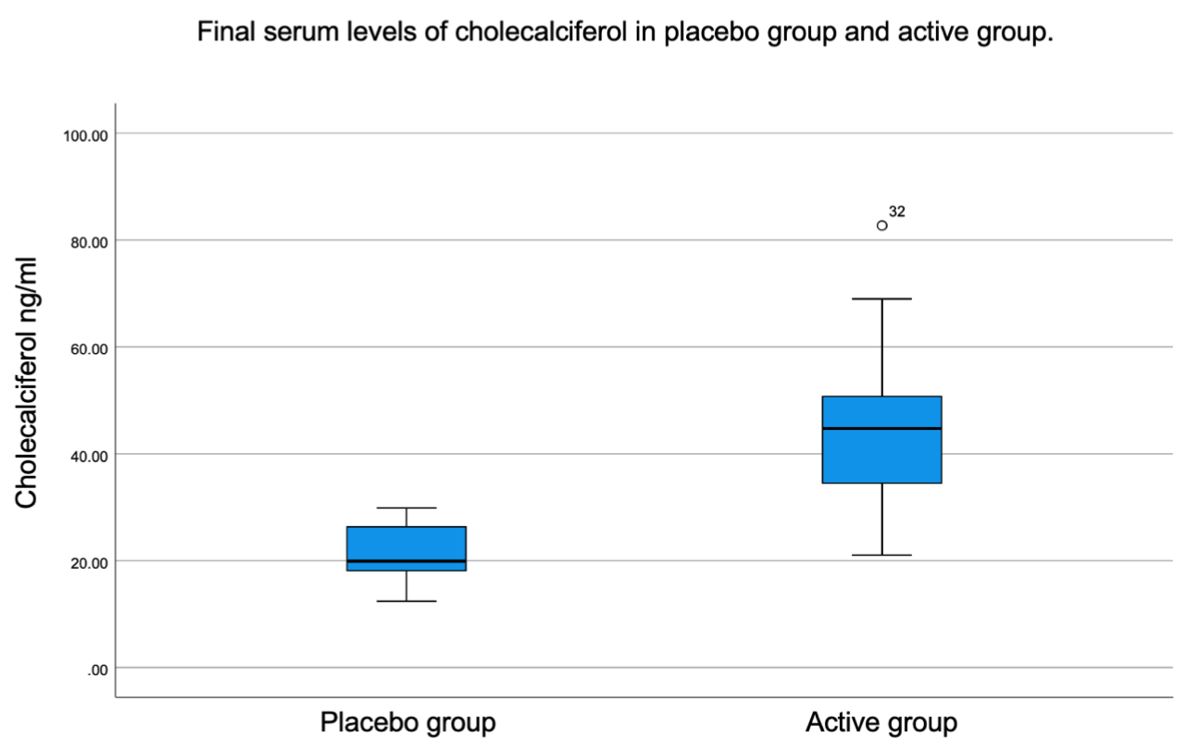
Figure 2: Final serum levels of cholecalciferol in placebo group and active group
FIGURE 3
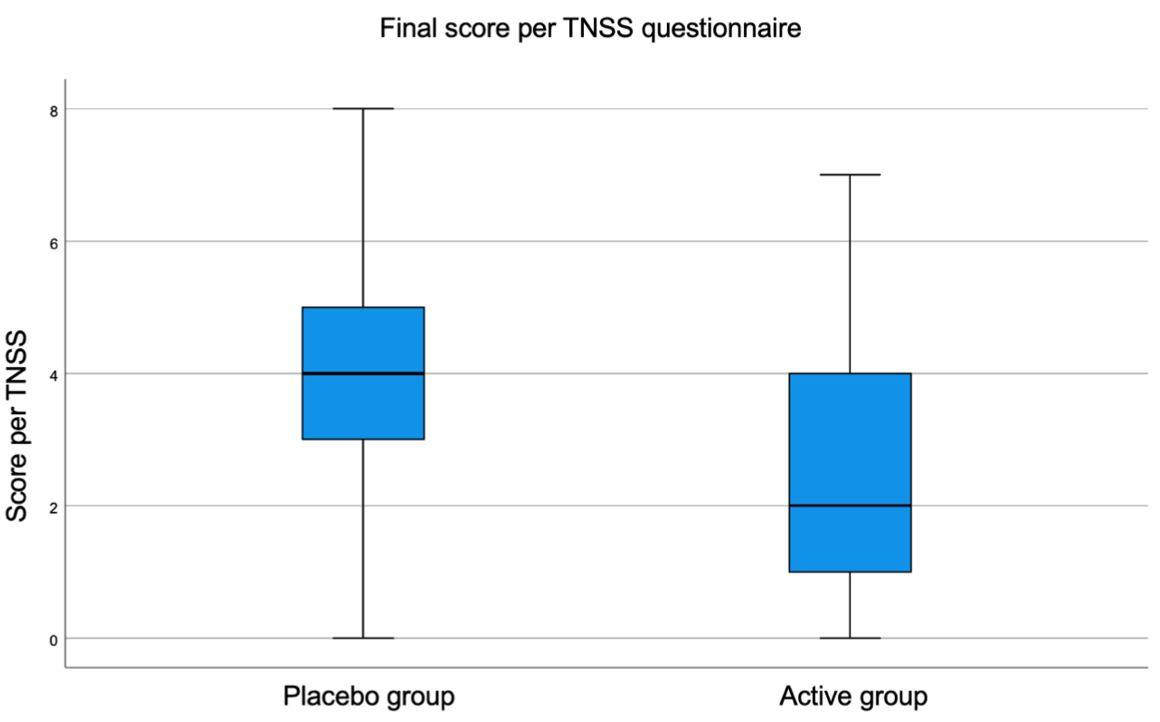
Figure 3: Final TNSS
Tables at a glance
Figures at a glance