Effect of Psycho-Education and Mindfulness-Based Stress Reduction on Psychological Stress in Carers of Relatives with Dementia in Iran: a Randomized Controlled Trial
Received Date: December 11, 2022 Accepted Date: January 11, 2023 Published Date: July 14, 2023
doi: 10.17303/ejmrc.2023.5.101
Citation: Victoria Omranifard, Azam Mansourzadeh, Mohsen Janghorbani (2023) Effect of Psycho-Education and Mindfulness Based Stress Reduction on Psychological Stress in Carers of Relatives with Dementia in Iran: a Randomized Controlled Trial. Eur J Med Res Clin Trials 5: 1-13
Abstract
Background and Objectives: The intention of this randomized controlled trial was to compare the relative usefulness of psycho-education (PE) and mindfulness-based stress reduction (MBSR) training programs on carers of relatives with dementia (RWD).
Materials and Methods: An eight-week, randomized, controlled trial was accomplished from March to December 2020.Ninety carers of RWD were randomly allocated to PE or MBSR-training program. Carers were rated at baseline and at the 8-week after training with the Beck Depression Inventory, Hamilton Anxiety Inventory, Coping Response Inventory, and the Short Form of Health Survey.
Results: A significant decrease in state anxiety symptoms and gains in problem-focused coping appeared in both groups. In the 45 carers trained by MBSR, the mean (SD) of the anxiety score declined from 37.0 (1.9) to 35.6 (1.7) (P<0.001). Of the 45 carers trained by PE, the mean (SD) of the anxiety score declined from 36.7 (1.2) to 34.5 (2.9) (P < 0.001). The mean (SD) of problem-focused coping score increased from 15.5 (5.0) to 16.7 (4.8) (P<0.001) and from 14.7 (5.8) to 15.5 (5.7) (P <0.05) in the PE and MBSR groups. Carers’ adherence was fine and no unpleasant effects were seen.
Conclusions: Both MBSR and PE significantly reduce state anxiety symptoms and gains in problem-focused coping. MBSR demonstrated no superiority over the PE-training program.
Trial Registration: irct.ir: IRCT20161010030255N4 registration date 18/12/2020
Keywords: Mindfulness; dementia; caregiver; clinical trials; psychoeducation.
HighlightsCaring for people with dementia is a source of stress, anxiety, and depression, which strongly affects the health and quality of life of carers. Both MBSR and PE significantly reduce state anxiety symptoms and gains in problem-focused coping.Both MBSR and PE training previously reduce stress and anxiety, and MBSR demonstrated no superiority over the PE training program.
Introduction
Dementia is an important cause of older adults'morbidity and mortality and its rate is increasing worldwide,due to rapid population aging, affecting more than 50million people in 2020 [3,4]. At present 60% of people with dementia live in low and middle income nations, but by 2050, this will increase to 71% [3,4] The growing rate of dementia throughout the world and Iran is prominent and requires new plans to cover new demands [28] Iran is facing a fast growth rate of the mature residents, due to the fast decline in the fertility rate and rise in life expectancy [26] The speedy population aging in Iran can be linked with unpleasant health issues, consisting of an increase in age-related disorders such as dementia. The age- adjusted prevalence of dementia in Iran based on the WHO standard population was 8.1% (9.6% in women and 6.9% in men) in people over 60years old. The prevalence of dementia raised with population grow older, as the rate was 3.7% in the age-group 60-64years; while it reached 13.0% in the age-group ≥ 80 years [31,4] The total diagnostic rate of dementia in Iran is 21.2% [31] This low diagnostic rate is due to the general population’slack of knowledge about dementia and it is also due to incorrect belief declaring that aging is normally related to memory loss and thus the older adults with memory weakening do not need to seek health services [31] Another possible cause of low diagnostic rate is the dearth of clinical awareness of dementia among clinicians [31] This under-reporting rate could affect the support services to the RWD. [2]
As families play a crucial role in the care of the older persons, the responsibility of caring for people with dementia is subsequently put on family carers in most cases,and the length of home caring can be as long as approximately 7 years [7,3]. High levels of psychological and physical distress are the most prevalent and disabling symptomsin carers of relatives with dementia (RWD) [9,3] It is linked with considerable depression, emotional problems, and impaired quality of life, and adversely affecting daily activity for many family carers. Stress controlling can enhance care, coping skills, and treatment outcomes of RWD and reduced anxiety, increase self-efficacy, confidence, and better ability to perform; therefore, the management of depressive symptoms in carers of RWD is an important goal [37] Rumination and emotion regulation may decrease perceived stress and increase coping skills in RWD.
Universal, cost-effective dementia care that supports the quality of life is deemed a public health main concern [36,3] Many types of psychological and social interventions have been established to decrease the carers’ stress and depressive symptoms and improve their general well-being with an overall small to moderate effect size [29, 34, 30, 8,13, 20, 38, 33]. Several reviews have failed to find a steadily effective method for decreasing the distress and burden suffered by carers of RWD [6,14,22] suggest that further studies should ascertain how best to intervene to benefit carers of RWD well-being and other key consequences. The psychological intervention used most frequently is the eight-week mindfulness-based stress reduction (MBSR) [30] Some studies with inactive or active controls show that stress is reduced by MBSR training in carers of RWD [14,27, 35]
Psycho-educational (PE) interventions are an important and effective tool for psychological health management.These programs provide carers of RWD with information,coping strategies, and support, thus broadening carers' knowledge and understanding of RWD. It improves the coping skills and decreases the burden of care for carers of RWD. Few studies show that anxiety and stress is reduced by PE training in carers of RWD [11, 12, 20, 27]
This randomized controlled trial, compared the effects of PE and MBSR training to explore which was more useful in the management of caring-related state anxiety symptoms, depression, coping, and quality of life. We hypothesized that the MBSR training program would be superior to the PE program in reducing depression, state anxiety,and gain coping and quality of life 8-week after intervention.
Research Design and Methods
An eight-week randomized, single-blinded trial was used to compare the effects of PE and MBSR-training program for managing state anxiety symptoms, depression,coping, and quality of life in carers of RWD. Participants were told that they would be randomized to one of two eight-week mind/body courses, both of which benefited other aspects of health and well-being. The research procedure was accepted by the Institutional Review Board of the Isfahan University of Medical Sciences, Iran and all contributors provided written informed consent. All procedures were carried out in accordance with the pertinent guidelines and regulations. The trial protocol was registered with the Iranian clinical trial registry (IRCT20161010030255N4, and registration date 18/12/2020).
Participants
The participants were carers of relatives with any type of dementia living at home. Family carers of consecutive patients with a definite diagnosis of any type of dementia who sought treatment at our psychiatric clinics at Isfahan University of Medical Sciences, Iran, between March and December 2020 were evaluated. We did not consider care workers who were paid to provide care to people with dementia. Inclusion criteria included men and women principal carers of RWD,18 to 60 years, living with them, can read and write, having continuing care-giving accountability for first-degree RWD and having no self-reported doctors’diagnosis of psychiatric ill health and impaired cognitive status and will participate in one of two eight-week courses. Exclusion criteria included significant chronic illnesses that affect their contribution, were under treatment for serious mental disorders or with uncontrolled mood disorders,untreated depression, alcohol or drug abuse, history of suicidal ideation, or an episode of severe depression within the three months before enrollment and had prior experience of contributing in a mindfulness intervention, cognitive therapy, or structured psychosocial intervention.
Randomization design
Participants were randomized by applying a list of computer-generated numbers, and the group allocations were masked in an impenetrable sealed envelope until just before entry into the study. 115 family carers of consecutive patients with dementia were qualified for the study. Twenty- five family carers were excluded because they refused entry.The 90 participants were allocated randomly and similar to one of the two training groups. The 90 participants(15 men, 75 women) randomized to the intervention groups included in the analyses. The first training group obtained MBSR and the second group received PE-training for eight weeks. At enrollment, all family carers had a pre-training evaluation that contained demographic data, complete medical history, physical and psychiatric examination. The patient allotment is displayed in Figure 1.
Evaluation
All contributors were blinded to our study hypothesis.The trial was single-blinded in that the carers of RWD were not aware of which training they were receiving, did not know the contents of either course before randomization,and did not know the content of the course that they were not allocated to. The primary efficacy measure was the decrease in depression, state anxiety symptoms, and gains in coping and quality of life. Participants were rated at baseline and at eight-week after intervention using self-administered tests. The scale was described to the carers. One physician (VO) who knows which family carers had received which intervention was in charge of all clinical assessments of all carers.
Mindfulness-based stress reduction intervention
Mindfulness was defined as "moment-to-moment awareness, cultivated by paying attention specifically, in this moment, as non-reactively, non-judgmentally, and open--heartedly as possible" [19] The MBSR intervention comprised eight weekly one and half-hour sessions developed by Kabat-Zinn, 2013. The main talents trained in MBSR included body scan, sitting meditation, yoga postures, and mindfulness in each day activities (mindful eating, walking,listening, etc.). The classes consist of 12 to 15 persons. To warrant the consistency of program administration, the identical course procedure and teaching materials were handled in the different classes. The MBSR program also comprised day-long intensive mindfulness training and discussion session. Course work projects, intended to strengthen techniques and general approaches, involved 45 min/day of MBSR, six days/week. A clinical psychologist (AM) experienced in MBSR taught the weekly course and handled weekly telephone support calls during the intervention and encouraged participants to practice daily and ensured there were no logistical problems influencing subjects’ persisted contribution. The MBSR program was somewhat altered for this study population from the established MBSR program [19] particularly in its time schedule and in minor changes to mindfulness exercises to adjust physical limitations common among older individuals and difficult situations during COVID-19 pandemic. Additionally, separating carers from the RWD for more than two hours may be too large a burden.
Psycho-education intervention
The PE course had the same group format as MBSR and consisted of eight weekly one and half-hour sessions.The emphasis of the course was mind/body medicine and comprised eight lectures. Course programs involved the effect of stress on physical and psychological health and management, the effect of stress on sleep, dementia in the older adults, and management, skillful communication, and practical home-nursing advice, and advice on mental health and a healthy lifestyle. A clinical psychologist (AM) taught the weekly course and performed weekly telephone support calls during the intervention and stimulated the PE group to practice daily or apply what they were learning in their intervention and make sure there were no logistical problems affecting subjects’ continued participation.
Measures
All questionnaires used in our study have been validated in Persian. Following the completion of baseline evaluations, participants were invited to self-administer questionnaire to eight-week after the intervention. The frequency and duration of home practice of MBSR (including mindfulness in daily activities) was recorded on a weekly practice note that was collected each week during the course. Clinically related depressive symptoms were assessed by the Persian version of the Beck Depression Inventory (BDI) [10] The BDI is a recognized self-report device for screening depression and contains 21 items, each consisting of four self-descriptive statements, which the subject rates on a 4-point measure of severity. The interpretation was based on a 0-63 total score. The tool showed good reliability with Cronbach's alpha of 0.85 and robust construct validity based on moderate-to-strong positive correlations with other measures of mental health issues [10]
Validated Persian versions of the Hamilton State Trait Anxiety Inventory [32, 1] are a self-report measure with two 20-item scales that measure self-reported state, or current, anxiety (State-A) and trait, or chronic, anxiety (Trait-A). Persons are requested to rate items on a 4-point scale as to how well they illustrate the subjects current or typical mood, from not at all to very much so. Scores range from 20 to 80 on each scale, with higher scores demonstrating greater anxiety. In this study, the state-trait anxiety was considered. Its internal validity ranged from 0.84 to 0.90. The reliability of the scale ranged from 0.85 to 0.89, with test-retest analysis [1]
The Short Form 36 (SF-36) [24] includes 36-item was also used to measure the health-related quality of life. It covers eight emotional and physical domains: physical function, role limitations due to physical health problems, pain,general health perceptions, vitality, social functioning, role limitations due to emotional problems, and general mental health. These eight subscales can be evaluated from physical and mental perspectives. The scores of each area vary from zero to 100, which shows that higher scores reveal higher levels of functioning or well-being. Internal reliability analysis disclosed that the Persian version of SF-36 had minimum standard reliability of 0.77 to 0.90 [24]
Cope with a recent problem or stressful situation was measured by the validated Persian version of the Coping Response Inventory for adults (CRI-A) [25, 2]. The CRI-A is a recognized self-report instrument for screening coping and contains 32 items that measure the problem- (11 items) vs. emotion- (8 items) focused on, each including 4 self-descriptive statements, which the subject rates on a 4--point scale of seriousness. The interpretation is based on a 0-57 total score (0-32 for problem-focused and 0-24 for emotion-focused coping), with higher scores indicating greater problem or emotional coping. Internal reliability analysis showed that the Persian version of CRI-A had a minimum standard reliability of 0.53 to 0.92 [2]
Statistical analysis
The sample size was computed when the study was planned and was based on the comparison of two means. Assuming a standard deviation (SD) for treatment differences in BDI score of 6.5, as observed in other studies testing psychological treatments [12] we computed that 60 participants per the treatment group and assuming a 20% attrition rate would be needed to provide the study with approximately 80 percent power to identify (with a two-sided alpha of 0.05) a mean difference in BDI scores of at least 3.0 between family carers who obtained MBSR vs. those who obtained PE. The groups received MBSR and PE were compared with Student t-test for independent samples and a mixed ANOVA to compare the effects of PE and MBSR over time. Baseline and eight-week after intervention periods were compared with paired Student t-tests. Percentages were compared with the chi-squared or Fisher’s exact tests. The findings are stated as the mean (SD) unless expressed otherwise, and P < 0.05 was taken into account statistically significant. All the statistical tests were two-sided. All analyses were performed with SPSS version 25 software for Windows (SPSS Inc., Chicago, IL).
Results
Fifteen of the 90 participants (8 in the MBSR group and 7 in the PE group) accomplished the training program but dropped out before completing the eight-week after intervention follow-up because they had time constraints related to caring or had a difficult situation during the COVID-19 pandemic. All 90 carers with RWD completed the 8-week intervention; and among them, 75 completed the 8-week follow-up assessment. The drop out of this study was 16.7%, and the MBSR group had a drop-out rate similar to that of the PE group (17.8% vs. 15.5% P = 0.57). The drop-outs and completers had similar age (49.2 year vs.51.1year, P = 0.36), anxiety score (36.5 vs. 36.9, P = 0.30), emotional-focused coping score (17.7 vs. 17.8, P = 0.74),problem-focused coping score (14.9 vs. 15.2, P = 0.84) and quality of life score (72.1 vs. 71.2, P = 0.66) at baseline. The two training groups were well matched at baseline concerning age, gender, depression, state anxiety symptoms, quality of life, and coping score (Table 1). Depression and anxiety scores were elevated at baseline for both groups, indicating mild-to-moderate levels of depression and higher levels of anxiety. Adherence was assessed by class attendance and family carers’ adherence to both training groups was good and no adverse effects were observed. Mean (SD) of participant attendance rates at classes was similar in both groups (MBSR group 0.84 (0.07); PE group 0.87 (0.04)). Carers had a mean (SD) age of 50.8 (7.1) year (range 35 to 60 year) (50.1 (7.6) year in the MBSR group and 51.5 (6.6) year in the PE group) at registration. Women accounted for 75 (83.3%), while men accounted for 15 (16.7%) of the 90 carers of RWD.
Changes in depression, state anxiety symptoms,quality of life, and coping eight-week after receiving MBSR or PE-training are shown in Table 2. At eight-weeks after intervention,in both the MBSR and PE groups, state anxiety,emotional and problem-focused coping scores significantlyimproved. The average state anxiety score decreased from baseline by 2.2 (95% CI; 1.50, 3.08) in the PE group, compared with a decrease of 1.4 (95% CI; 1.14, 1.94) in the MBSR group. The mean emotional-focused coping score decreased from baseline by 0.8 (95% CI; 0.4, 1.3) in the PEgroup, compared with a decrease of 0.4 (95% CI; 0.04, 0.73) in the MBSR group. The average problem-focused coping score increased from baseline by -1.2 (95% CI; -2.11, -0.66) in the PE group, compared with an increase of -0.8 (95% CI;-0.95, -0.10) in the MBSR group. The average quality of life score slightly decreased from baseline by -0.3 (95% CI;-0.33, -0.06) in the MBSR group, but not in the PE group.The average depression score decreased from baseline by 0.5 (95% CI; 0.17, 0.96) in the PE group, but not in the MBSR group.
The overall analysis of repeated measures ANOVA showed significance decrease in anxiety score in both training groups at the end of the trial between the PE and MBSR groups (F= 81.9, df = 2, P<0.001). Also, overall repeated measures ANOVA disclosed a significant increase in problem-focused coping score (F=21.98, df = 2, P<0.001) and a significant decrease in emotional-focused coping score in both training groups (F= 22.07, df = 2, P<0.001)(Table 3). There were no significant interaction effect (group) on the anxiety score or problem-focused coping score relationship (P > 0.05)
Discussion
This study compared the relative efficacy of MBSR versus PE on carers of RWD. This study shows that although both MBSR and PE training for 8 weeks decreased the burden of carers state anxiety symptoms and increased problem-focused coping eight-week after the intervention period, MBSR showed no superiority over PE. MBSR revealed no clear evidence of any effect on depression,whereas PE slightly decreased carers depression. Instead, PE showed no clear evidence of any effect on quality of life, whereas MBSR slightly increased carers quality of life.
Concerning carer's anxiety, our result showed a significant association between MBSR and PE-training program and anxiety, which was consistent with a significant finding from Dharmawardene et al. meta-analysis [11], but inconsistent with another meta-analysis [22] that no significant effect was found for the alleviation of carers’ anxiety.These inconsistencies may be due in part to the debate linked with the methodological differences in the included trials between these two reviews. Other studies also show a positive effect of MBSR on mental health [15, 27, 35] Our findings confirm that the intervention effect becomes clear eight weeks after the intervention. The current results agree with Hou et al. [15] who compared MBSR with an inactive control (self-help control group) and demonstrated improvement in state anxiety symptoms among participants in the MBSR group, although this difference was not statistically significant at 3-month after intervention training.
Depressive symptoms are the most common behavioral symptoms in carers of RWD and many types of psychological and social interventions, including MBSR, showed a reduction of the carers’ stress and depressive symptoms with a total trivial to modest effect size [8, 13, 20, 29, 30, 33, 38]. Surprisingly, in present trial MBSR did not show a significant effect on the depression level, although we could see a trend of decreased mean depression after PE intervention. There were several possible elucidations. The decreased sample size resulting from drop-out reduced the power to test for a significant difference between the two groups and therefore there had been a type I error. Also, the tools used in our study might not have been sensitive enough to measure the changes in depressive score. In a systematic review and meta-analysis of seven RCTs with 410 carers of RWD, [22] investigated the usefulness of MBSR in decreasing the stress of carers of RWD.Their results showed that MBSR may reduce carers' depressive symptoms, stress, and enhance the quality of life of carers,at least in the short-term, but due to low-quality evidence,they could not be sure of any effect on clinically important depressive symptoms. Because of the low-quality of the evidence, they could not be certain of any effect on carers’coping style, nor could they ascertain whether carers were almost likely to drop out of the intervention. They suggested that MBSR can meet some significant needs of the carers, but more high-quality studies must confirm its usefulness. In another Cochran's review of four RCTs and quasi-experimental studies with 168 participants, [20] studied the efficacy of MBSR in decreasing the stress of carers of RWD. The analysis showed that MBSR seems to be effective at reducing stress. Despite differences in types of interventions, assessed outcomes, data comparison, and analysis between this review and Liu et al. [22] both reviews found that evidence of MBSR for carers is still preliminary,and that based on the available evidence, no clear conclusion could be reached. Hou et al. (15) in an RTC with inactive control (self-help control group) suggested a significant decrease in depressive symptoms after intervention and at 3-month after intervention.
The results of this study showed that both MBSR and PE training might improve coping capabilities in every-day life and even under more extraordinary situations of severe stress, such as caring. The results from this study, are coherent with other reviews studying carers of individuals with advanced illnesses (encompassed but not limited to dementia) [17, 11, 16]
Our study shows eight-week after intervention,MBSR had a significant positive effect on the quality of life score of carers of RWD, a result that was not seen in the PE group. There were no important differences between the MBSR and PE groups in expressions of quality of life. Similarly,Hou et al. [15] found no statistically significant effects on the quality of life.
The mechanisms whereby MBSR or PE exerts positive effects on the coping state of carers of RWD are not entirely clear. It is possible that MBSR and PE training may affect several dimensions of psychological stress among carers. Under continuing stress for several years, carers of RWD could have problems altering their automatic and usual ways of reacting to continuous caring. MBSR and PE--training offer an occasion for carers to be aware of their useless reactions or thought patterns. More studies are necessary to ascertain how MBSR or PE may impact psychosocial pathways that may also contribute to the positive effects on the coping state of carers of RWD.
This trial has some limitations, including single-blind scheme, brief follow-up, and small sample size. Although the importance of the double blind, controlled trial is extensively documented, this design is not always suitable or suggested. Treating physicians dealing with carers and their RWD can easily become un-blinded. The duration of this trial was relatively short to evaluate the effect of MBSR and PE. Whether the special effects of this short-term MBSR and PE intervention will continue in the longer term are unclear. It is likely that an 8-week after intervention follow-up be short to realize the real influence of the intervention.Evaluating the usefulness in the long-term period is,therefore, reasonable. Although the number of participants studied was small, the effect was robust. While we enrolled carers of RWD from the tertiary care center and less than 60 years old, generalizability to other populations and older carers is undetermined. Finally, the cognitive status, behavioral symptoms, health conditions, caregiving duration, hours providing care per week, of the individuals with dementia who were being cared for by the carers were not measured.These are stressors for carers, which might have affected the results. There was only one trainer for both interventions in this study delivers all the MBSR and PE-training sessions and thus, disparities in the application of the interventions will be minimized. It is reasonable to assume that the trainer may have conflated some aspects of the interventions.
In conclusion, this study indicated that adherence to both MBSR and PE-training program is good and well--tolerated by carers of RWD and the data furnish more support for the argument that both MBSR and PE are suitable instruments in the managing of state anxiety symptoms, depression, coping, and quality of life of carers of RWD. PE training program could be an alternative for those dementia carers who have not good experience with MBSR outcomes.Our conclusions underline the need for a larger sample size and longer follow-up period to approve these preliminary results and better comprehend the mechanisms by which MBSR and PE modify anxiety and increase coping in carers of RWD.
Declarations
Ethics approval and consent to participate: The research procedure was accepted by the Institutional Review Board of the Isfahan University of Medical Sciences,Iran and all contributors provided written informed consent.
Consent for publication: Not applicable
Availability of data and materials: We would like to inform you that the datasets analyzed in the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that there are no conflicts of interest associated with this manuscript
Funding
This study was partially supported by the Isfahan University of Medical Sciences, Iran.
Acknowledgments
We state our thankfulness to all the family carers who agreed to participate
- Abdoli N, Farnia V, Salemi S, Davarinejad O, Ahmadi- Jouybari T et al. (2020). Reliability and validity of the Persian version of the State-Trait Anxiety Inventory Among High School Students. East Asian Arch Psychiatry 30: 44-7.
- Aguilar-vafaie ME, Abiari M (2007) Coping Response Inventory: Assessing coping among Iranian college students and introductory development of an adapted Iranian Coping Response Inventory (CRI). Mental Health, Religion & Culture 10: 489-513.
- Alzheimer's disease facts and figures (2022).Alzheimer's Dement 18: 700-89.
- Breijyeh Z, Karaman R (2020) "Comprehensive Review o HYPERLINK Disease: Causes and Treatment".
- Molecules (Review) 25: 5789.
- Bourgeois MS, Schulz R, Burgio L (1996) Interventions for caregivers of patients with Alzheimer’s disease: A review and analysis of content, process, and outcomes. International Journal of Aging and Human Development 35-92.
- Brodaty H, Donkin M (2009) Family caregivers of people with dementia. Dialogues Clin Neurosci 11: 217-28.
- Caspar S, Davis ED, Douziech A, Scott DR (2017) Nonpharmacological management of behavioral and psychological symptoms of dementia: what works, in what circumstances,and why? Innovation in Aging 1: 1-10.
- Cooper C, Balamurali TBS, Selwood A, Livingston G (2007) A systematic review of intervention studies about anxiety in caregivers of people with dementia. International Journal of Geriatric Psychiatry 223: 181-8.
- Dadfar M, Kalibatseva Z (2016) Psychometric Properties of the Persian version of the Short Beck Depression Inventory with Iranian Psychiatric Outpatients. Hindawi Publishing Corporation Scientifica, Article ID 8196463.
- Dharmawardene M, Givens J, Wachholtz A,Makowski S, Tjia J (2016) A systematic review and meta-analysis of meditative interventions for informal caregivers and health professionals. BMJ Support Palliat Care., 6: 160-9.
- Gallagher-Thompson D, Coon DW (2007) Evidence-based psychological treatments for distress in family caregivers of older adults. Psychol Aging 22: 37-51.
- Gilhooly KJ, Gilhooly ML, Sullivan MP, McIntyre A,Wilson L et al. (2016) A meta-review of stress, coping and interventions in dementia and dementia caregiving. BMC Geriatr16: 106.
- Gottlieb BH, Wolfe J (2002) Coping with family caregiving to persons with dementia: A critical review. Aging and Mental Health, 6: 325-42.
- Hou RJ, Wong SY, Yip BH, Hung AT, Lo HH et al.(2014) The effects of mindfulness-based stress reduction program on the mental health of family caregivers: A randomized controlled trial. Psychotherapy and Psychosomatics 83: 45-53.
- Hurley RV, Patterson TG, Cooley SJ (2014) Meditation- based interventions for family caregivers of people with dementia: a review of the empirical literature. Aging Mental Health 18: 281-8.
- Jaffray L, Bridgman H, Stephens M, Skinner T (2016) Evaluating the effects of mindfulness-based interventions for informal palliative caregivers: A systematic literature review. Palliat Med 30: 117-31.
- Kabat-Zinn J (2011) Some reflections on the origins of MBSR, skillful means, and the trouble with maps. Contemporary Buddhism 12: 281-306.
- Kabat-Zinn J (2013) Full Catastrophe living: using the wisdom of your body and mind to face stress, pain and illness.New York, Delacorte press.
- Kishita N, Hammond L, Dietrich CM, Mioshi E (2018) Which interventions work for dementia family carers?An updated systematic review of randomized controlled trials of carer interventions. Int Psychogeriatr 30: 1679-96.
- Kor PP, Chien WT, Liu JY, Lai CK (2018) Mindfulness-based intervention for stress reduction of family caregivers of people with dementia: a systematic review and meta-analysis. Mindfulness 9: 7-22
- Liu Z, Chen QL, Sun YY (2017) Mindfulness training for psychological stress in family caregivers of persons with dementia: a systematic review and meta-analysis of randomized controlled trials. Clin Interv Aging 12: 1521-9.
- Montazeri A, Goshtasbi A, Vahdaninia M (2005) Translation, reliability and validity of Persian as the SF36.Quality of Life Research 14: 875-82.
- Moos RH (1993) Coping Response Inventory Professional Manual Adult Form. FL: PAR
- Norouzian M (2012) The elderly population in Iran:an ever-growing concern in the health system. Iran J Psychiatry Behav Sci 6: 1-6
- Oken BS, Fonareva I, Haas M, Wahbeh H, Lane JB et al (2010) Pilot controlled trial of mindfulness meditation and education for dementia caregivers. Journal of Alternative and Complementary Medicine 16: 10-1038
- Sabayan B, Bonneux L (2011) Dementia in Iran:How soon it becomes late! Archives of Iranian Medicine, 14:290-1.
- Schulz R, Martire LM, Klinger JN (2005) Evidence-based caregiver interventions in geriatric psychiatry.Psychiatr Clin North Am 284: 1007-38.
- Shapiro S, Brown KW, Biegel GM (2007) Teaching self-care to caregivers: effects of mindfulness-based stress reduction on the mental health of therapists in training. Training and Education in Professional Psychology 12: 105-15.
- Sharifi F, Fakhrzadeh H, Varmaghani M, Arzaghi SM, Alizadeh Khoei M et al. (2016) Prevalence of Dementia and Associated Factors among Older Adults in Iran: National Elderly Health Survey (NEHS). Arch Iran Med 19: 838-44.
- Spielberger CD, Gorusch RL, Lushehe R, Vagg PR,Jacobs GA (1983) Manual for the State-Trait Anxiety Inventory.Mountain View (CA): Consulting Psychologist Press
- Vandepitte S, Van Den Noortgate N, Putman K, VerhaegheS, Faes K et al. (2016) Effectiveness of supporting informal caregivers of people with dementia: a systematic review of randomized and non-randomized controlled trials. J Alzheimers Dis 52: 929-65.
- Van Houtven CH, Voils CI, Weinberger M (2011) An organizing framework for informal caregiver interventions:detailing caregiving activities and caregiver and care recipient outcomes to optimize evaluation efforts. BMC Geriatr 11: 77.
- Whitebird RR, Kreitzer M, Crain AL, Lewis BA, Hanson LR et al. (2013) Mindfulness-based stress reduction for family caregivers: a randomized controlled trial. The Gerontologist 53: 676-86.
- World Health Organization. (2012) Dementia: A Public Health Priority. World Health Organization.
- World Health Organization (2015) Supporting informal caregivers of people living with dementia.
- Ying J, Wang Y, Zhang M, Wang S, Shi Y et al.(2018) Effect of multicomponent interventions on competence of family caregivers of people with dementia: a systematic review. J Clin Nurs 27: 1744-58.
FIGURE 1
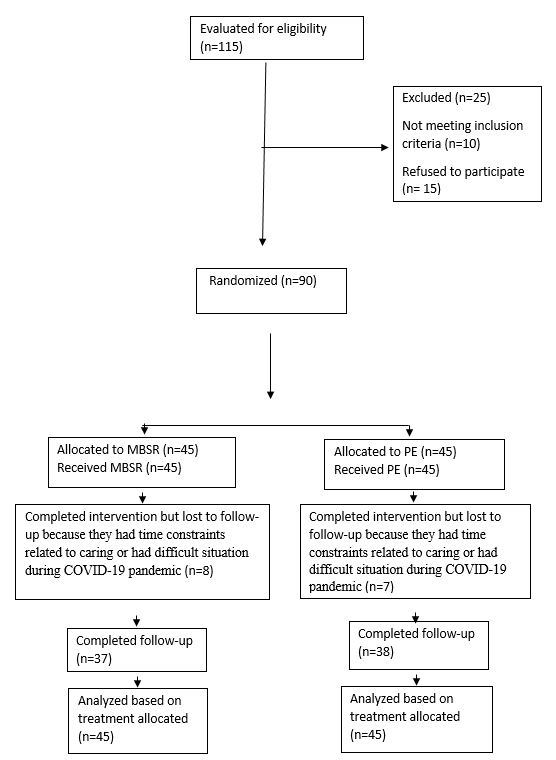
Figure 1: Scheme of the study.
Tables at a glance
Figures at a glance