The Association of Postmenopausal Osteoporosis with Serum Inflammatory Biomarkers
Received Date: February 18, 2023 Accepted Date: March 18, 2023 Published Date: March 21, 2023
doi: 10.17303/ejmrc.2023.5.102
Citation: Minoo Ranjbar, Sanaz Malekian, Nasrin Abolhasanpour, Azizeh Farshbaf-Khalili, The Association of Postmenopausal Osteoporosis with Serum Inflammatory Biomarkers. Eur J Med Res Clin Trials 5: 1-13
Abstract
Introduction: During menopause, when estrogen levels fall, inflammatory cytokines such are activated and predispose women to osteoporosis
Objectives: This study aimed to compare inflammatory markers between 50-65-year-old postmenopausal women with osteoporosis and normal bone mineral density (BMD).
Materials and Methods: This was a cross-sectional study conducted in health centers of Tabriz, northwest Iran. Of 850 randomly-selected eligible postmenopausal women, 100 women with normal BMD and 101 peers with osteoporosis (diagnosed based on dual-energy X-ray absorptiometry after ruling out other secondary causes) were included in the study. Data collection tools included questionnaires for gathering demographic, anthropometric, and physical activity data. Interleukin-6, TNF-α, and high sensitivity C-reactive protein (hs-CRP) were measured by biochemical methods. The data were analyzed by SPSS-21 software using descriptive and analytical statistics, including the independent t-test, Chi-square test, Fisher’s exact test, Mann-Whitney, and binary logistic regression.
Results: There were significant differences between the two groups in terms of age, menopausal age, body mass index, and education level (p< 0.005). Also, serum levels of TNF-α (p=0.026) and hs-CRP (p< 0.001) were significantly different between the two groups. However, the results of logistic regression analysis adjusted for the confounders showed that the elevation of only hs-CRP could significantly increase the risk of osteoporosis (OR (95% CI)= 42.41 (12.66-142.3), p< 0.001).
Conclusions: An elevated serum level of hs-CRP was a sensitive marker of increased risk of osteoporosis. Due to the fact that hs-CRP provides an exact and cost-effective test, it can be used for timely screen and prevent osteoporosis in postmenopausal women
Keywords: Menopause; Osteoporosis; Bone Density; Inflammatory Mediators; Biomarkers
Introduction
Osteoporosis is a skeletal disease characterized by low bone mass and weakened and damaged tissue structure [1]. Osteoporosis is also one of the most common metabolic bone diseases, and it is characteristically associated with decreased bone strength, predisposing patients to fracture [2]. About 10% of the world’s population and 30% of postmenopausal women suffer from osteoporosis. This rate is about 32% in Iran, presenting a prevalence close to the global average. It has been estimated that about 10 million Iranians suffer from this disease, and 34 million people in the country show low bone density and are at a high risk of osteoporosis [3].
Unlike many other chronic diseases that have multiple signs and symptoms, osteoporosis remains silent until a fracture occurs [4]. The clinical significance of osteoporosis lies in the risk of bone fractures. According to the International Osteoporosis Association, osteoporotic fractures will comprise more than 50% of all bone fractures occurring in East and Southeast Asia by 2050 [5]. Menopause followed by decreased levels of sex steroid hormones is the main cause of osteoporosis in women [6].
Also, estrogen levels decline during menopause, followed by the activation of inflammatory cytokines such as IL-6 and TNF-α, which lay the groundwork for osteoporosis [7]. Cytokines are important regulators of bone metabolism. Interleukin-6 seems to be a potent osteoporotic cytokine with important roles in increasing bone resorption and activation of osteoclasts. This cytokine, which is produced by monocytes, is one of the most important mediators associated with metabolic bone diseases, including osteoporosis. Tumor necrosis factor-α, a cytokine naturally involved in inflammatory and immune responses, is mainly produced by innate immune cells such as macrophages. This mediator can promote osteoporosis by inducing the expansion and activation of osteoclasts [8]. C-reactive protein is also an acute phase protein that increases in response to tissue damage, inflammation, and infections. This protein is synthesized in the liver in response to the factors released by adipocytes. During the first 6 to 8 hours of infection, the hs-CRP level rapidly rises, inducing the release of free radicals and augmenting the activity of phagocytes, paving the way for osteoporosis [9]. Inflammatory mediators shrink bone mass by increasing the rate of apoptosis in osteocytes; however, further studies are recommended to disclose the molecular and cellular mechanisms that link inflammatory factors to bone metabolism [10].
Despite the increase of inflammatory mediators after menopause, a few studies have been conducted in Iran aiming to investigate inflammatory factors in postmenopausal women with osteoporosis. So, this study was performed to compare inflammatory factors between post-menopausal women with osteoporosis and women with normal bone density in Tabriz, northwest Iran. This study can enrich our knowledge about the relationship between inflammation and osteoporosis and help prevent and control osteoporosis by modifying the lifestyle.
Materials and Methods
Study design and participantsThis was a descriptive cross-sectional case-control study. The study population included all postmenopausal women who had an electronic file in the health centers of Tabriz. Among 850 eligible postmenopausal women who were randomly selected, 100 women with normal bone density and 101 women with osteoporosis (diagnosed based on dual-energy X-ray absorptiometry after ruling out other secondary causes of osteoporosis) entered the study.
Inclusion criteria: Postmenopausal women aged 50 to 65 years living in Tabriz, having no menstrual cycle for at least 12 consecutive months, no history of pathological fractures in the last 10 years, the ability to communicate verbally to answer questions, receiving no hormone therapy during the recent last year, and reaching menopause after the age of 40 years were regarded as for inclusion criteria.
Exclusion criteria were the diagnosis of bone diseases other than osteoporosis diagnosed by an endocrinologist, suffering from hereditary diseases (hemophilia, thalassemia, and hemochromatosis), endocrine disorders (Cushing’s syndrome, hyperthyroidism, renal failure and diseases, type 1 diabetes, and primary hyperparathyroidism) confirmed by an endocrinologist, hepato-gastrointestinal diseases (chronic liver diseases such as primary biliary cirrhosis, celiac disease, Crohn’s disease, total or partial gastrectomy), consuming drugs that affect bone metabolism (such as intravenous bisphosphonate) during the last five years, taking oral bisphosphonate during the last six months, taking oral bisphosphonate collectively for more than three years or more than one month during the recent six to 12 months prior to the start of the study, the use of parathyroid hormone analogues or Strontium during the last 12 months, consuming hormonal drugs or corticosteroids during the study, excessive use of thyroxine, cytotoxic drugs, immunosuppressive drugs (such as cyclosporines), prolonged use of some anticonvulsants (e.g. phenytoin), hypocalcemia, D25 (OH) level of < 20 ng/ml (i.e., secondary osteoporosis), and finally, body mass index < 18.5 [11]. An endocrinologist, a member of the research team, examined all the participants for the eligibility criteria and differentiating between primary and secondary osteoporosis. Osteoporosis was detected as a low bone density in the lumbar vertebrae or femoral neck when the T-score was ≤ -2.5; a T-score between -1 and -2.5 was designated as osteopenia, and a T-score ≥ -1 was marked as normal.
Sample SizeThe sample size in this study was determined using G-Power software and the formula designed for comparing the mean difference in a variable (IL-6 was used as the target variable in this study considering the higher sample size estimated using this variable). Based on the standard deviation of IL-6 level in women with osteoporosis (SD = 9.3) and considering α = 0.05 and d = 0.15 around the mean (m = 12.1), the sample size was determined as n = 100 per group [12].
The study protocol was approved by the research deputy of Tabriz University of Medical Sciences and received an ethics approval code from the Ethics Committee of Tabriz University of Medical Sciences (IR. TBZMED.REC.1397.733). We also obtained the necessary permits from health centers in Tabriz before starting to recruit participants. The city of Tabriz has 87 health centers that include the details and contact information of all postmenopausal women. We initially prepared a list of 50-65- year-old postmenopausal women registered in all of these 87 health centers using the integrated health system. Out of 108778 people, 850 women (about twice the required sample size) were selected by simple random sampling. The postmenopausal women selected were then telephoned and briefly explained the objectives and protocols of the study. If they agreed to participate in the study, we requested them to refer to the health center at a specific time. Overall, 730 eligible women were interviewed via phone and asked to refer to health centers on specific dates. Then the objectives of the study were fully explained during face-to-face meetings, and the inclusion/exclusion criteria were reviewed using a checklist. In this step, 194 people who did not fulfill the inclusion criteria were excluded from the study. Blood samples (10 mL) were obtained from the remaining 536 individuals to analyze CBC/diff and the serum levels of calcium, phosphorus, ALP, TSH, creatinine, FBS, and vitamin D to differentiate primary osteoporosis from secondary osteoporosis. Blood samples were analyzed in the laboratory of the Nutrition Research Center of Tabriz University of Medical Sciences by an expert. The final diagnosis of osteoporosis and differentiation of primary and secondary osteoporosis were made by an endocrinologist (a member of the research team). According to the results of these tests, 74 people were diagnosed with secondary osteoporosis and excluded from the study. Seventeen individuals who were unwilling to continue participation in the study were excluded.
Finally, the demographic and midwifery questionnaires were completed for 445 individuals who were then referred to the Sina Hospital of Tabriz for determining the bone density of the lumbar vertebrae and femoral neck via Dual-energy X-ray absorptiometry (DEXA). All measurements were performed by the same expert. For measuring bone density, the criteria of T score (the number of standard deviations between the patient’s bone mass and the average bone mass in young adults) and Z score (the number of standard deviations between the patient’s bone mass and the average bone mass for the same age and weight) were determined, and bone mineral density (BMD) was measured as g/cm2 . According to the instruction of the World Health Organization (WHO), the T scores of ≥-1, between -1 and -2.5, and ≤-2.5 are regarded as normal, osteopenia, and osteoporosis (i.e., a BMD lower than 2.5 SD of that of a 30- year-old man or woman), respectively [13]. According to the reports of densitometry analysis, 142 individuals had normal BMD; 109 women were osteoporotic, and 194 individuals were diagnosed with osteopenia. Out of the mentioned individuals, 100 women with normal BMD and 101 women with osteoporosis were assigned via simple random sampling. These individuals were subjected to blood sampling (5 mL) in the fasting condition to measure the inflammatory factors of TNF-α, hs-CRP, and IL-6. Blood samples were collected in tubes containing serum separator gels and centrifuged for 10 minutes at 3500. The sera were stored at -80°C. The measurements were performed using biochemical assays by the researchers in the Nutrition Research Center under the supervision of a laboratory specialist.
Measurement of Study VariablesThe demographic questionnaire included queries about the age, menopausal age, occupation, education level, marital status, the adequacy of monthly income for living expenses, vacancy status, smoking, hookah use, alcohol consumption, physical activity, sunlight exposure, using supplementation, family history of bone fractures due to osteoporosis, body mass index, and finally, history of hypertension & dyslipidemia.
The level of physical activity was assessed using a short version of the International Physical Activity Questionnaires (IPAQ), whose validity and reliability have been confirmed in Iran [14]. This tool was completed by interviewing the participant, and the level of physical activity was calculated as either light, moderate, or intense.
First, dietary intake was evaluated using a three-- day food registration questionnaire (two nonconsecutive weekdays and one weekend day). In terms of total energy, fiber, macronutrients, vitamins and minerals were analyzed using Nutritionist IV software (First Databank, San Bruno, CA) modified based on Iranian foods.
The serum levels of TNF-α and IL-6 were determined using commercial kits purchased from Carmania Pars Gene Co. (Iran) following the manufacturer’s instructions. The working and standard solutions were prepared using the reagents provided by the distributor in packages at indicated conditions and temperatures and in recommended dilutions. The optical absorption of the samples was read at 450 nm using an ELISA reader (Bio Tek Instruments Inc., the USA), and the ODs were employed to determine the cytokine’s serum concentration. Also, the serum level of hsCRP was measured using a commercial kit provided by Pars Azmoun Co. (Iran) using an autoanalyzer. The kit worked based on a reinforced turbidimetric method (i.e., photometry two-point measurement) and the formation of a complex between hs-CRP and antiserum.
In this study, the content validity method was used to verify the scientific validity of the tools. To determine the reliability of the tests, the first 10 samples were assayed twice (under two different names) by each test, and the reliability of the test results was calculated [15].
Statistical AnalysisThe data obtained from the questionnaires and densitometry analysis were first entered into SPSS software (version 24). The Kolmogorov-Smirnov test was used to evaluate the normality of quantitative variables, showing the non-normal distribution of inflammatory biomarkers in the study groups. The socio-demographic and midwifery characteristics were presented by descriptive statistics, including frequency, percentage, mean, and standard deviation. The above-mentioned characteristics were compared between the study groups using the Chi-square test and Fisher’s exact test (for qualitative data), as well as the t-test (for quantitative data). The main variables of the study were compared between the two study groups (osteoporotic women and those with normal BMD) using the independent ttest (for normally distributed data) or Mann-Whitney test (for non-normally distributed data). Also, a logistic regression model was used to adjust for the effects of confounding variables, and the odds of osteoporosis were calculated for each of the study variables. The goodness of fit of the model was checked by the Hosmer and Lemeshow test. The results of the analyses were interpreted at a P value of less than 0.05 as the statistical significance level.
Results
In this study, 100 women with normal BMD and 101 women with osteoporosis were compared in terms of serum inflammatory biomarkers. Figure 1 shows the flow chart of participant selection, and Table 1 describes the participants’ demographic data and it compares the daily food intake in two groups. The results showed that there were significant differences between the two groups in terms of age (p< 0.001), menopausal age (p= 0.034), BMI (P< 0.001), and education level (P=0.002). The mean age was higher but the mean menopausal age, BMI, and education level were lower in osteoporotic women than in their counterparts with normal BMD. No significant difference was observed between the two groups in terms of other demographic features. The means of BMD, T-score, and Z-score in lumbar vertebrae and femoral neck were significantly lower in the osteoporosis group than in the normal BMD group.
Table 2 shows that the median (IQR) serum IL-6 level was 19.26 (6.26) pg/mL in the group with normal BMD and 19.42 (7.75) pg/mL in the osteoporosis group. According to the Mann-Whitney test, this difference between the two groups was not statistically significant (P=0.289).
The median (IQR) of serum TNF-α was 20.76 (16.84) pg/mL in the osteoporosis group, which was significantly lower than that of the control group (25.45 (13.03) pg/mL P=0.026). The medians (IQRs) of hs-CRP were 0.95 (0.67) and 0.31 (0.67) mg/L in the osteoporosis and control groups, respectively, showing a significantly higher level in the former (p< 0.001)
Table 3 shows the results of the binary logistic regression model to predict the odds of developing osteoporosis in postmenopausal women based on inflammatory biomarkers and after adjusting for the age, menopausal age, BMI, and education level. According to the results, the odds of developing osteoporosis were not related to serum levels of IL-6 (p=0.628) and TNF-α (p=0.391). However, the risk of osteoporosis increased significantly by the elevation of serum hs-CRP (OR (95% CI) = 42.41 (12.66-142.3), p< 0.001).
Discussion
The results of the present study showed that in comparison with women who had a normal BMD, osteoporotic women had a higher mean age but a lower mean menopausal age, BMD, and education level. Although there was a significant difference between the two groups in terms of the serum levels of TNF-α and hs-CRP, after adjustment for the effects of confounding variables, the risk of osteoporosis significantly increased only in correlation with rising hs-CRP levels. In this regard, each unit increase in the serum hs-CRP level intensified the risk of osteoporosis by more than 40 times.
In parallel with the fall of estrogen levels (as an antioxidant agent boosting total antioxidant capacity, i.e., TAC), inflammatory cytokines such as IL-6 and TNF-α are activated during menopause, paving the path for osteoporosis development (7). A novel molecular system belonging to the TNF family, comprising RANKL and osteoprotegerin (OPG), has been identified to regulate bone degradation (16). Along with RANKL, OPG glycoprotein regulates bone metabolism via modulating osteoclasts. On the other hand, RANKL enhances bone resorption by binding to the nuclear receptor activator of nuclear factor kappa B (NF-kB). The binding of OPG to RANKL suppresses the activity of the latter, thereby inhibiting bone resorption and reducing osteoclastogenesis (17). The nuclear factor kappa B mediates a key signaling pathway involved in the early stages of RANKL-induced osteoclast differentiation and is known as an evolutionary family of transcription factors promoting protection against environmental insults (18). One of the consequences of menopause is an increase in the activity of bone-eating cells due to a decrease in estrogen. This process continues for 10 to 15 years so that at end of this time, there will be 50% and 30% reductions in the mass of spongy and dense bones, respectively, correlating with a boost in the incidence of bone fractures in this period (i.e., 60 to 75 years old) (19). In the absence of estrogen, osteoclasts become more active, leading to more bone loss and causing bones to become thinner. Therefore, the rate of bone loss in postmenopausal women increases 2-3% annually due to decreased estrogen levels (20).
In agreement with our findings, Benjamas et al., in a cross-sectional study conducted on 102 men with COPD, showed that BMI and hs-CRP were significantly associated with osteoporosis (P = 0.001). In the recent study, patients with osteoporosis had lower BMIs and higher hs-CRP levels compared with peers with normal bone mass (21). Sudjaroen et al., in a cross-sectional study on 105 adult men and women over the age of 60 years, reported that the serum level of hs-CRP was higher in osteoporotic individuals compared with those with normal BMD (22), which was consistent with our study
Pasco et al., in a 2006 study in Australia, evaluated the association of hs-CRP with the risk of bone fractures in older women. The baseline level of hs-CRP was assessed by the Roche (latex) method; BMD was measured by the DEXA technique, and the data were analyzed by Lunar Dpx–L software (version 1.31). The results of the recent study showed that although there was no significant relationship between hs-CRP and BMD, elevated serum levels of hs-CRP were associated with an increased risk of fracture (23). The recent study differed from our study in terms of the methods of measuring inflammatory biomarkers, the sample size, as well as inclusion criteria, and the follow-up period.
Safari et al., in a 2019 case-control study in Shiraz (Iran), investigated the association of serum levels of circulating amyloid A, hs-CRP, and vitamin D with osteoporosis in postmenopausal women. Forty-four postmenopausal women with osteoporosis (the case group) and 44 postmenopausal women without osteoporosis (the control group) were compared, revealing no significant difference in hsCRP serum levels between the two groups (24). The results of the recent study contradicted our observation, which can be due to differences in the sample size, the age spectrums of participants, and the fact that we excluded secondary causes of osteoporosis in our study.
Kimble et al. revealed that IL-6 and TNF-α were regulated by estrogen, and therefore, contributed to the reduction of bone density secondary to estrogen deficiency (25). This notion opposes our findings in the present study, which can be attributed to differences in study designs (the recent experimental research had been conducted on mice). Besides, we should notice that after adjustment for the impacts of confounding variables, the link between TNF-α and osteoporosis disappeared.
Lizha et al. in a study in 2018 showed that TNF-α could contribute to postmenopausal osteoporosis via enhancing RANKL-induced osteoclastogenesis. They showed that TNF-α levels were considerably higher in osteoporotic postmenopausal women compared with counterparts with out osteoporosis (26). This report was inconsistent with our observation. In explanation, we should reiterate that the secondary causes of osteoporosis were excluded in our study, which was not the case in Lizha et al.'s study. Moreover, the sample size of our study was smaller than theirs.
Zheng et al. showed that direct stimulation boosted the blood levels of IL-1β, IL-6, TNF-α, IFN-γ, GM-CSF, and LIF, among which the production of IL-6 and TNF-α was significantly higher in women with osteoporosis than in healthy controls subjects (27). The reason for the inconsistency between our findings and that of Zheng et al. can be different sample sizes and inclusion criteria.
In a study in Saudi Arabia in 2017, Al-Daghri et al. aimed to investigate the link between pro-inflammatory mediators and bone turnover markers in postmenopausal women with or without osteoporosis. The results of the recent research showed that IL-6 and TNF-α serum levels were significantly higher in osteoporotic women compared to control subjects (28). The inconsistency between our observations and that of the recent study can be justified by the different age spectra of participants in the two studies (50-65-yearold vs. over 50-year-old). In addition, the two studies employed different methods to measure inflammatory biomarkers.
In this study, the random sampling method was used to avoid selection bias. The participants were selected among postmenopausal women referring to health centers located in areas with different socioeconomic situations distributed across the city of Tabriz to allow generalization of results to a larger population of postmenopausal women. Due to the lack of a relationship between secondary osteoporosis and lifestyle, women with this type of disease were identified and excluded from the study. The age range was chosen at 50-65 years due to the importance of this age range for the loss of bone density following the sharp reduction of estrogen. Therefore, the results may not be generalizable to postmenopausal women over the age of 65 years. Also, the results cannot be generalized to the entire population (including men). Serum estrogen levels were not measured in this study.
Conclusion
In this study, higher serum levels of hs-CRP and TNF-α were associated with an increased risk of osteoporosis. However, after controlling for confounding variables, only hs-CRP increased the odds. Considering that osteoporosis is one of the important problems in the country's health system, which will take on wider dimensions due to the change in the demographic pattern in the future and on the other hand, the high prevalence and debilitating side effects have made osteoporosis one of the most important health issues, the investigation of inflammatory biomarkers and its increasing trend, and on the other hand, the cheapness and cost-effectiveness of hs-CRP measurement. It can be used for prevention and timely screening of this disease in postmenopausal women.
- Ahmadian F, Mozaffari-Khosravi H, Azaraein MH, Faraji R, Zavar-Reza J (2017) The effect of consumption of garlic tablet on proteins oxidation biomarkers in postmenopausal osteoporotic women: A randomized clinical trial. Electronic physician 9: 5670.
- Weitzmann MN, Pacifici R (2006) Estrogen deficiency and bone loss: an inflammatory tale. Eur. J. Clin. Invest 116: 1186-94.
- Hemmati F, Sarokhani D, Sayehmiri K, Motadayen M (2018) Prevalence of osteoporosis in postmenopausal women in Iran: a systematic review and meta-analysis. IJOGI 21: 90-102.
- Riou B, Rothmann C, Lecoules N, Bouvat E, Bosson JL, Ravaud P et al (2007) Incidence and risk factors for venous thromboembolism in patients with nonsurgical isolated lower limb injuries. AJEM 25: 502-8.
- Sugimoto T, Sato M, Dehle FC, Brnabic AJ, Weston A, Burge R (2016) Lifestyle-related metabolic disorders, osteoporosis, and fracture risk in Asia: A systematic review. Value Health Reg Issues 9: 49-56.
- Pansini F, Mollica G, Bergamini CM (2005) Management of the menopausal disturbances and oxidative stress. Curr. Pharm. Des 11: 2063-73.
- Biglia N, Cagnacci A, Gambacciani M, Lello S, Maffei S, Nappi R (2017) Vasomotor symptoms in menopause: a biomarker of cardiovascular disease risk and other chronic diseases? Climacteric 20: 306-12.
- McMahon MS, Ueki Y (2008) Does anti-TNF-alpha have a role in the treatment of osteoporosis? Bull Hosp Jt Dis 66: 280.
- Ganesan K, Teklehaimanot S, Tran T-H, Asuncion M, Norris K (2005) Relationship of C-reactive protein and bone mineral density in community-dwelling elderly females. J. Natl. Med. Assoc 97: 329.
- Domazetovic V, Marcucci G, Iantomasi T, Brandi ML, Vincenzini MT (2017) Oxidative stress in bone remodeling: role of antioxidants. Clin Cases Miner Bone Metab 14: 209.
- Kawaguchi H, Pilbeam CC, Vargas SJ, Morse EE, Lorenzo JA, Raisz L (1995) Ovariectomy enhances and estrogen replacement inhibits the activity of bone marrow factors that stimulate prostaglandin production in cultured mouse calvariae. J. Clin. Investig 96: 539-48.
- Parhami F (2003) Possible role of oxidized lipids in osteoporosis: could hyperlipidemia be a risk factor? Prostaglandins Leukot. Essent. Fat. Acids 68: 373-8.
- Yalin S, Bagis S, Polat G, Dogruer N, Aksit SC, Hatungil R et al (2005) Is there a role of free oxygen radicals in primary male osteoporosis? Clin. Exp. Rheumatol 23: 689.
- Committee IR (2005) Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ)-short and long forms.
- Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE et al (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35: 1381-95.
- Rao L, Rao A (2013) Oxidative stress and antioxidants in the risk of osteoporosis—role of the antioxidants lycopene and polyphenols. Topics in osteoporosis 5: 117-44.
- Léotoing L, Wauquier F, Guicheux J, Miot-Noirault E, Wittrant Y, Coxam V (2013) The polyphenol fisetin protects bone by repressing NF-κB and MKP-1-dependent signaling pathways in osteoclasts. PloS one 8: e68388.
- Kamyabi Z, Aflatonian M, Bahrampour A (1997) Determination of the mean age of menopause and it's distribution terms of known variables in Kerman. JKMU 5: 178-85.
- Rachner TD, Khosla S, Hofbauer LC (2011) Osteoporosis: now and the future. The Lancet 377: 1276-87.
- Lindsay R, Aitken J, Anderson L, Hart D, MacDonald E, Clarke A (1976) Long-term prevention of postmenopausal osteoporosis by oestrogen: evidence for an increased bone mass after delayed onset of oestrogen treatment. The Lancet 307: 1038-41.
- Rittayamai N, Chuaychoo B, Sriwijitkamol A (2012) Prevalence of osteoporosis and osteopenia in Thai COPD patients. J. Med. Assoc. Thail 95: 1021.
- Sudjaroen Y (2018) Association of bone-related biochemical markers and risk of prehypertension in osteoporotic elders AJP 12(01).
- Pasco JA, Kotowicz MA, Henry MJ, Nicholson GC, Spilsbury HJ, Box JD et al (2006) High-sensitivity C-reactive protein and fracture risk in elderly women. Jama 296: 1349-55.
- Safari A, Borhani-Haghighi A, Dianatpour M, Heydari ST, Foroughinia F, Omrani GR (2019) Circulating Serum Amyloid A, hs-CRP and Vitamin D Levels in Postmenopausal Osteoporosis. GMJ 8: e1548.
- Kimble RB, Bain S, Pacifici R (1997) The functional block of TNF but not of IL‐6 prevents bone loss in ovariectomized mice. JBMR 12: 935-41.
- Zha L, He L, Liang Y, Qin H, Yu B, Chang L et al (2018) TNF-α contributes to postmenopausal osteoporosis by synergistically promoting RANKL-induced osteoclast formation. Biomed. Pharmacother 102: 369-74.
- Zheng S, Vrindts Y, Lopez M, De Groote D, Zangerlé P-F, Collette J et al (1997) Increase in cytokine production (IL-1β, IL-6, TNF-α but not IFN-γ, GM-CSF or LIF) by stimulated whole blood cells in postmenopausal osteoporosis. Maturitas 26: 63-71.
- Al-Daghri NM, Aziz I, Yakout S, Aljohani NJ, AlSaleh Y, Amer OE et al (2017) Inflammation as a contributing factor among postmenopausal Saudi women with osteoporosis. Medicine 96.
FIGURE 1
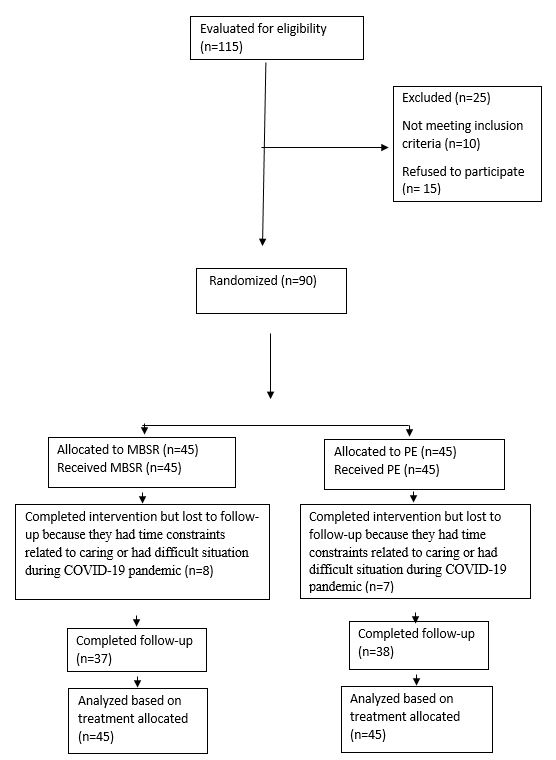
Figure 1: The process of selecting study participants
Tables at a glance
Figures at a glance