Intravitreal Injection of Etamsylate Improves Visual Acuity in Patients with Dry Age-Related Macular Degeneration. Results from the International, Multicentric,Blind, Randomized, and Sham-Controlled Jericho-D Study
Received Date: August 12, 2023 Accepted Date: September 12, 2023 Published Date: September 15, 2023
doi: DOI: 10.17303/ejmrc.2023.5.103
Citation: Pedro Cuevas, Javier Angulo, Luis Outeirino, Laura Monje, Joao Figueira et al. (2023) Intravitreal Injection of Etamsylate Improves Visual Acuity in Patients with Dry Age-Related Macular Degeneration. Results from the International, Multicentric, Blind, Randomized, and Sham-Controlled Jericho-D Study. Eur J Med Res Clin Trials 5: 1-11
Abstract
Background
Dry age-related macular degeneration (AMD) is a disease that progressively worsens over time. As of 2022, there are no medications available to reverse or stop worsening of dry AMD. With the anticipated increase in dry AMD cases related to an aging population, there is an increasing and important unmet need for new dry AMD therapies.
Methods
Fifty one patients with dry AMD were included in the international, multicentric, randomized, blind, controlled Jericho-D study. Primary endpoint of the study was, for each subject, the difference in best-corrected visual acuity (BCVA) between the baseline values and those determined after 90 days of a single intravitreal injection of etamsylate or sham treatment. BCVA was determined by using the Early Treatment Diabetic Retinopathy Study (ETDRS) chart. A crossover design was used.
Findings
BCVA significantly improved in patients with dry AMD 90 days after intravitreal injection of etamsylate. The difference in number of letters read in the ETDRS optotype between the baseline values and after 90 days of treatment was in terms of least square mean (SD): 8.66 (3.49), p = 0.0169. In contrast, no significant improvement was observed in sham-treated patients: 3.70 (3.41), p=0.2838. No adverse events related to the treatment were detected.
Interpretation
Etamsylate improves visual acuity in patients suffering dry AMD, representing a therapeutic potential in a disease without available treatment.
Keywords: Dry Age-Related Macular Degeneration; Etamsylate; Intravitreal Injection; Fibroblast Growth Factor; Inflammation
Introduction
Age-related macular degeneration (AMD) is characterized by changes in the central region of the retina, known as the macula, and mostly affects individuals over 50 years of age. The disease causes various degrees of visual impairment and can lead to blindness. In fact, AMD is the most frequent cause of visual loss in industrialized countries and is associated with the majority of blind registrations [1]. A systematic review and meta-analysis conducted on all population-based studies of AMD published before May, 2013 showed a worldwide prevalence for AMD of 8.69% (mapped to an age range of 45-85 years), and the projected number of people with the disease was around 196 million in 2020, increasing to 288 million in 2040 [2]. In this sense, it is estimated that 19.8 million people aged 40 years and older were living with any stage of AMD in the United States [3]. AMD is diagnosed as being dry or wet, depending on the absence or presence of abnormal growth of new blood vessels (angiogenesis) in the macular region. Non-exudative (dry) AMD comprises more than 90% of patients diagnosed with AMD. Clinical funduscopic examination showing yellow spots called drusen in the areas proximal to the fovea or macula is a diagnostic feature of dry AMD. Histopathologic features of dry AMD include atrophy and loss of retinal photoreceptors and retinal pigment epithelium (RPE), deposition of drusen between the RPE and Bruch membrane along the chorioretinal interphase, and accumulation of lipofuscin. Drusen can be detected early in this type of AMD without visual loss. As dry AMD progresses to retinal atrophy and central retinal degeneration, loss of central vision is often observed. Generally, dry AMD has a much slower (over decades) progressive visual loss relative to wet AMD (over months). Central blind spots (scotomas) usually occur late in the disease and can sometimes become severe. Symptoms are usually bilateral. While there is no proven effective treatment for dry AMD, wet AMD is mostly pharmacologically treated with agents inhibiting vascular endothelial growth factor (VEGF) and hence neoangiogenesis. Therefore, the search for pharmacological therapies to treat dry AMD is of utmost clinical importance.
The fibroblast growth factor (FGF) is a powerful pro-inflammatory and proangiogenic protein that plays an important role in the pathophysiology of both forms of AMD [4-8]. In normal conditions, FGF is strictly regulated by its attachment to the extracellular matrix. After physical or chemical injury, an important amount of FGF is released from the extracellular matrix and participates in the pathological processes occurring during inflammation and angiogenesis. 2.5-dihydroxybenzene sulfonate is a synthetic FGF inhibitor blocking the coupling of free FGF to its receptor without any effect on sequestered physiological FGF [9,10], maintainingphysiological activity of this factor [11]. Etamsylate is the diethylammonium salt of 2.5-dihydroxybenzene sulfonate that has been on the market since more than 50 years for treating haemorrhages. Dicynone® (etamsylate 250 mg/2 ml), by Sanofi-Aventis laboratories (Paris, France) is commercialised in liquid form in France and Switzerland. Previous case reports and uncontrolled clinical studies have suggested the efficacy of intravitreal administration of etamsylate for the treatment of both forms of AMD [12-15].
The main aim of the present multicentre, randomised, blind, sham-controlled, 2x2 cross-over phase III clinical trial was to evaluate the efficacy and the safety of an intravitreal injection of etamsylate to improve visual acuity in patients with dry AMD.
Methods
Patients
Jericho-D is an international, multicentre, randomised, blind, sham-controlled, 2x2 cross over phase III clinical trial conducted from 2018 to 2021 (EudraCT 2017‐ 003899‐31). We included adult (aged ≥18 years), male and female outpatients with diagnosis of dry AMD from seven centres in Spain, Portugal and Italy. Inclusion criteria were: to have best corrected visual acuity (BCVA) between 20/25 and 20/320, measured by ETDRS optotype (Early Treatment Diabetic Retinopathy Study), to use highly effective contraconceptive methods in the case of women with childbearing potential, to have the capacity and disposition to follow the study protocol and procedures and to grant their informed consent in writing (signed and dated), accepting voluntarily to participate in the trial.
Exclusion criteria were: patients with grade 5 AMD in one or both eyes, patients with any concomitant ocular disease that, under investigator’s judgement, could influence the development, evaluation or assessment of the AMD, such as glaucoma, permanent structural damage in the centre of the fovea, geographic parafoveolar atrophy, polypoid choroidal vasculopathy etc.; patients with ocular or periocular infection; patients with any concomitant disease that, under investigator’s judgement, could influence (the disease itself or its treatment) the development, evaluation, or assessment of the AMD, such as diabetes mellitus with ocular affectation, current or active systemic infection, any ocular infection, psychiatric diseases, social situation that may affect study protocol compliance, etc.; patients treated with any intravitreal anti-VEGF agent or other intravitreal drug such as corticosteroids within the last month prior to study randomisation; pregnant or breastfeeding women (urine pregnancy test to be performed for those patients of childbearing potential); hypersensitivity to etamsylate or any of the excipients contained in the form used for the trial; patients with any of the contraindicated diseases described in the summary of product characteristics of Dycinone, such as but not limited to: porphyria, bleeding caused by treatment with anticoagulants, fibrosis/benign tumours in the uterus and patients with a recent history of stroke; patients having participated in dry-AMD clinical trials with intervention (observational, epidemiologic, or economic studies were allowed).
Ethics
Prior to initiation of the study at each investigational site, the protocol, the informed consent form(s), the patient information sheet(s), details of the patient recruitment procedures and any other relevant study documentation were submitted to the responsible local and/or central institutional review board (IRB)/ ethics committee (EC). A letter from each IRB/EC indicating approval of the investigator and study site were obtained by the study Sponsor.
The guidelines of the World Medical Association Declaration of Helsinki in its revised edition (48th General Assembly, Somerset West, Republic of South Africa, October 1996), the guidelines of ICH GCP (Committee for Proprietary Medicinal Products/ICH/135/95), as well as the demands of national drug and data protection laws and other applicable regulatory requirements, were strictly followed.
The investigators were responsible for ensuring that patients did not undergo any study-related examination or activity before giving informed consent. All patients or legal guardians gave written consent after the receipt of detailed information regarding the study. The investigators informed the patient of the aims, methods, anticipated benefits, and potential hazards of the study, including any discomfort it may entail. The patient was informed that he or she was free to either discontinue study drug and/or withdraw consent to participate at any time, without penalty or loss of benefits to which he or she was otherwise entitled.
Procedures
The study has been conducted as a 2x2 cross-over design, meaning that patients have received treatment in two different sequences over two periods of 90 days each. Group 1 has received etamsylate on day 1 and sham treatment on day 90, whilst Group 2 has received sham treatment on day 1 and etamsylate on day 90 (Figure 1). Crossover design was chosen as it has been deemed the most appropriate design given that AMD is a chronic and stable disease and the treatment is intended for improvement of patient’s quality of life, not cure, allowing to maximize the data obtained from both study groups.
Etamsylate was administered via intravitreal injection, the dose used has been 12.5 mg (100 µL of Dycinone ampoule). Preliminary results have shown an efficacy of 86.7% of BCVA improvement by etamsylate in patients with dry-AMD, in parallel with amelioration of retinal structural alterations [15].
One eye of each patient was selected for the study. More affected eye was selected in patients suffering from dry AMD in both eyes. Computer-generated randomization was performed.
Although intravitreal injection is a delicate procedure, intravitreal drug administration is a standard procedure in all the sites where the study was conducted. Most important risk of the procedure, with a very low probability of 0.1 to 0.3%, is infectious endophthalmitis[16].
Precautions for minimizing the risk included administration in an adequate facility for the injection (compliant in terms of hygiene and materials for administration), use of sterile materials and products, and disinfection of the eye with 5% povidone iodine topical in the conjunctival sac, accompanied by external cleaning of the eyelids with povidone iodine 10% (or similar disinfecting solution). Sham treatment will mimic etamsylate administration at all levels (preparation of patient, injection in the same facilities, position to receive an intravitreal injection, topic anaesthesia), but injection was not performed. In its place, the investigator pressed the conjunctival area with a blunt object.
The study design and procedure is outlined in Figure 1. After signature of the informed consent form, screening procedures were completed within 4 weeks before the intravitreal injection/sham treatment, as a basis for the evaluation of patients’ eligibility. Screening evaluation involved collection of demographic data, medical and ophthalmic history, concomitant medication, and ophthalmic examination (both eyes) that included best corrected visual acuity (BC-VA) determination and intraocular pressure (IOP) measurement. Check of all eligibility criteria was done. Selection of studied eye, randomization, group assignment and treatment/sham administration were made on study day (SD) 1. At this moment, baseline BCVA and IOP were determined prior to treatment administration. Then, intravitreal injection of etamsylate (Group 1) or sham procedure (Group 2) were administered. After the treatment, IOP was again determined and any adverse event was monitored. Revision with IOP measurement and adverse event monitoring was performed the day after treatment (SD2). Ninety days after treatment (SD90) with a tolerable range of ±15 days, BCVA and IOP were determined before the respective administration of intravitreal etamsylate (Group 2) or the sham procedure (Group 1). IOP and adverse events were monitored right after the treatment and on the following day (SD91).
Outcome Variables
Visual acuity (ETDRS)
Primary endpoint of the study was, for each subject, the difference in BCVA between the baseline values and those determined after 90 days of a single intravitreal injection of etamsylate or sham treatment. BCVA was determined by using the Early Treatment Diabetic Retinopathy Study (ETDRS) chart. This test was designed to eliminate inaccuracies in the Snellen and Sloan tests. The ETDRS score was obtained as follows: the patient started at the top of the chart and begins to read down the chart. The patient reads down the chart until he or she reached a row where a minimum of three letters on a line cannot be read. The patient was scored by how many letters could be correctly identified.
Intraocular Pressure (IOP) Measured by Tonometry
The tonometry measures the force needed to flatten an area of the cornea. The investigator shined a light into the eye to properly line up the instrument, and then delivered a brief puff of air at the eye. The machine measures eye pressure by looking at how the light reflections change as the air hits the eye.
Safety was evaluated throughout the duration of the study through the collection of adverse events (AEs) and serious adverse events (SAEs).
Statistical Analyses
Baseline characteristics were compared by unpaired t-test or Chi-square test. To correct the imbalance produced on some dates of the follow-up visit at 90 days, a time correction factor was applied, from which new corrected values were imputed to the quantitative variable number of letters read at 90 days. This adjustment was only applied for those visits at 90 days that were not within the tolerable time range (90 ± 15 days), and it was applied following these three steps: 1) the actual difference in the number of letters read between the screening visit and the 90-day visit was calculated;
2) This actual difference was multiplied by a time correction factor obtained by dividing 90 by the actual days that had elapsed between the screening visit and the 90-day visit
(in this way, an estimate was obtained of the change that would have occurred in the number of letters read if the visit had been made on the assigned date at 90 days); 3) this estimated change was added or subtracted from the number of letters read at the screening visit. In this way, an estimate was obtained of the value of the number of letters read (corrected value) that would have been obtained if the visit had been made on the assigned date at 90 days.
The difference in number of letters read in the ETDRS optotype between the baseline values and after 90 days of a single intravitreal injection of etamsylate was summarised by timepoint (baseline and Day 90) and by treatment arm. The comparison between the 2 treatments administered was performed by mean of a linear mixed model with baseline included as covariate. Treatment was included as fixed effects, with participant within sequence as random effect.
A probability less than 5% (p < 0.05) was considered significant
Role of the Funding Source
Dobecure SL, the sponsor of the Jericho-D study, did the randomisation. Otherwise, the sponsor had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
Efficacy
There were no significant differences between Group 1 and Group 2 with respect to age (79.7±8.4 yearsold vs. 76.8±8.9 years-old, respectively, p=0.232) or the eye included in the study (left in 73% vs. 56%, respectively, p=0.202). The percentage of smokers was 30.4% and 12.5 in Group 1 and Group 2, respectively, p=0.168. However, although not reaching statistical significance (p > 0.05), there was a difference in BCVA at baseline, determined as the number of letters read in the ETDRS optotype (16.54±12.53 vs. 22.32±17.81, respectively, p< 0.092). Considering this difference in baseline BCVA between Group 1 and Group 2, a linear mixed model with baseline BCVA included as covariate was applied. After this adjustment, BCVA significantly improved in patients with dry AMD 90 days after intravitreal injection of etamsylate. The difference in number of letters read in the ETDRS optotype between the baseline values and after 90 days of treatment was in terms of least square mean (SD): 8.66 (3.49), p = 0.0169. In contrast, no significant improvement was observed in sham-treated patients: 3.70 (3.41), p = 0.2838 (Figure 2).
Significant improvement in BCVA was maintained at 180 days after etamsylate injection as the difference in the number of letters read in the ETDRS optotype with respect to baseline did not decrease and was statistically significant (p < 0.01, Table 1). On the other hand, intravitreal injection of etamsylate to patients with dry AMD in Group 2 (previously sham-treated) caused an increase in the number of letters read in the ETDRS optotype leading to a significant difference (p < 0.05) with respect to baseline determined 180 days before (Table 1). Moreover, taking all patients, a significant increase in the number of letters read in the ETDRS optotype was obtained after 90 days of intravitreal etamsylate (6.39±2.36, p=0.0070; the comparison between the 2 timepoints (baseline and Day 90) was performed by mean of a linear mixed model with baseline included as covariate).
Safety
No etamsylate-related adverse effects were reported. Despite the prophylactic treatment included in the protocol, one patient suffered an aseptic endophthalmitis in the left eye, related to the intravitreal injection procedure, and was solved following standard of care therapy.
Moreover, intravitreal injection of etamsylate did not cause statistically significant alterations of IOP (15.8±2.9 mm Hg vs. 16.2±2.5 mm Hg for sham and etamsylate, respectively, p > 0.05, at 90 days follow-up).
Discussion
Main finding of the study is that intravitreal injection of 12.5 mg of etamsylate is safe and significantly improves BCVA in patients with dry age-related macular degeneration (AMD) at 3-months and 6-months follow-up. This supports the therapeutic potential of etamsylate in the clinical management of dry AMD.
AMD is the leading cause of blindness in adults over 50 years of age [17]. It encompasses two forms: wet (exudative) AMD and dry (non-exudative) AMD. Dry AMD is characterized by the development of drusen and alterations in the retinal pigmentary epithelium (RPE) that can progress to geographic atrophy of the macula [18]. Wet AMD is produced when new, immature blood vessels develop from the choroid layer of the retina leading to fluid extravasation. Since angiogenesis is the main feature of this form of AMD several therapies have been approved for treating it [19]. In contrast, dry AMD has no approved therapies [20]. Considering that dry AMD accounts for the 90% of cases of AMD [21], the lack of approved treatments represents a serious health concern.
Etamsylate is the ethanolamine salt of 2.5-dihydroxyphenyl sulfonate, which calcium salt is also known as dobesilate. Antagonistic effects by dobesilate on heparin-binding growth factors such as fibroblast growth factor (FGF) and vascular endothelial growth factor (VEGF) have been reported [9,22]. This ability would be related to its anti-angiogenic and anti-tumoral effects but also to its reported anti-inflammatory capacity. This is important since inflammation has been proposed as an important pathophysiological mechanism in dry AMD [23]. In fact, oral calcium dobesilate has demonstrated clinical efficacy in the treatment of diabetic retinopathy [24], an effect that could be related to its protective effects against oxidative stress and inflammation that were revealed in animal studies [25,26]. Moreover, in addition to the reported ability of intravitreal etamsylate to inhibit choroidal neovascularization [12,27], previous case reports and uncontrolled clinical studies reported short- (1 month) and long-term (12 months) beneficial effects of intravitreal injection of etamsylate on visual acuity and histological findings in patients with dry AMD [14,15,28]. Present results confirm such preliminary findings by demonstrating significant improvement by intravitreal etamsylate in visual acuity in patients with dry AMD after 90 and 180 days follow-up in an international, multicentric, blind, randomized and sham controlled clinical study.
Interestingly, the superiority to placebo (sham) was confirmed despite the presence of a difference in baseline visual acuity. This was achieved by application of a linear regression mixed model that allowed adjustment by baseline visual acuity.
A limitation of the study is the lack of data on the effects of intravitreal etamsylate on histological evolution of the retina in patients with dry AMD which were previously reported in uncontrolled studies [14,15]. This is relevant since it has been proposed the convenience of assessing anatomic biomarkers in clinical trials of dry AMD [29]. However, the present results demonstrating the improvement in visual acuity in dry AMD by etamsylate together with the lack of safety issues support the further clinical development of this therapeutic strategy including larger trials also evaluating the histological effects.
Other therapeutic strategies for the treatment of dry AMD are being evaluated. Relationship of genetic variants in complement related genes with AMD risk prompted to the evaluation of biological agents with antagonistic effects on complement with promising effects in reducing geographic atrophy area [29]. On the other hand, stem cell therapy has been proposed to restore damaged RPE in dry AMD. Different cell-based approaches have shown promising effects in improving vision in dry AMD patients [30]. Although these complex therapeutic strategies could show promising results in the future, genetic variation in the disease hinders the development of a unique strategy [19]. Etamsylate is a small molecule without the inconvenient of more complex developments, such as biologicals and cell therapies and is readily available in the market as injectable form for its use as anti-hemorrhagic and vascular protector, a fact that could facilitate its clinical development in dry AMD. In addition, etamsylate acts on the process of the disease (inflammation) rather than interfering with just a specific cellular pathway. In conclusion, the results of the Jericho-D international, multicenter, blinded, randomized and sham-controlled clinical trial demonstrate a significant improvement in visual acuity after 90 and 180 days after intravitreal injection of 12.5 mg etamsylate. These results support the further clinical development of intravitreal etamsylate for the treatment of dry AMD, providing a potential therapeutic tool for a disease without approved pharmacological treatment.
Authors Contribution
PC and JA wrote the manuscript. All authors critically reviewed the manuscript and provided final approval.
Acknowledgement
We thank Corina Andrei for the acquisition of data of this study. We thank Laura Muñoz, statistician, for the review of the data retrieved.
Conflict of Interest
The authors declare no conflict of interest.
- Bunce C, Wormald R (2008) Causes of blind certifications in England and Wales: April 1999-March 2000. Eye (Lond) 22: 905-11.
- Wong WL, Su X, Li X et al. (2014) Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. The Lancet Global Health 2: 106-16.
- Rein DB, Wittenborn JS, Burke-Conte Z et al. (2022) Prevalence of Age-Related Macular Degeneration in the US in 2019. JAMA Ophthalmol 140: 1202-8.
- Amin R, Puklin JE, Frank RN (1994) Growth factor localization in choroidal neovascular membranes of age-related macular degeneration. Invest Ophthalmol Vis Sci 35: 3178-88.
- Frank RN (1997) Growth factors in age-related macular degeneration: pathogenic and therapeutic implications. Ophthalmic Res 29: 341-53.
- Ambati J, Ambati BK, Yoo SH, Ianchulev S, Adamis AP (2003) Age-related macular degeneration: etiology, pathogenesis, and therapeutic strategies. Surv Ophthalmol 48: 257-93
- Donoso LA, Kim D, Frost A, Callahan A, Hageman G (2006) The role of inflammation in the pathogenesis of age-related macular degeneration. Surv Ophthalmol 51: 137-52.
- de Oliveira Dias JR, Rodrigues EB, Maia M, Magalhaes O Jr, Penha FM, Farah ME (2011) Cytokines in neovascular age-related macular degeneration: fundamentals of targeted combination therapy. Br J Ophthalmol 95: 1631-7.
- Fernandez IS, Cuevas P, Angulo J et al. (2010) Gentisic acid, a compound associated with plant defense and a metabolite of aspirin, heads a new class of in vivo fibroblast growth factor inhibitors. J Biol Chem 285: 11714-29.
- Angulo J, Cuevas P, Cuevas B et al. (2015) Diacetyloxyl derivatization of the fibroblast growth factor inhibitor dobesilate enhances its anti-inflammatory, anti-angiogenic and anti-tumoral activities. J Transl Med 13: 48.
- Oladipupo SS, Smith C, Santeford A et al. (2014) Endothelial cell FGF signalling is required for injury response but not for vascular homeostasis. Proc Natl Acad Sci USA 111: 13379-84.
- Cuevas P, Outeirino LA, Azanza C, Angulo J, Gimenez-Gallego G (2013) Clinical efficacy of intravitreal injection of Dobesilate for reversing choroidal angiogenesis in age-related macular degeneration. J Aging Gerontol 1: 1-8.
- Cuevas P, Outeirino LA, Azanza C, Gimenez-Gallego G (2013) Durable recovery of the macular architecture and functionality of a diagnosed age-related macular degeneration 1 year after a single intravitreal injection of dobesilate. BMJ Case Rep 2013: bcr2013010203.
- Cuevas P, Outeirino LA, Azanza C, Angulo J, Gimenez-Gallego G (2013) Dobesilate for dry age-related macular degeneration. J Biomed Sci Eng 6: 8-14.
- Cuevas P, Outeirino LA, Azanza C, Angulo J, Gimenez-Gallego G (2014) Intravitreal Dobesilate treatment of dry age-related macular degeneration: 12 months’ results. J Ocul Dis Ther 2: 1-6.
- Jager RD, Aiello LP, Patel SC, Cunningham ET (2004) Jr. Risks of intravitreous injection: a comprehensive review. Retina 24: 676-98.
- Pennington KL, DeAngelis MM (2016) Epidemiology of age-related macular degeneration (AMD): associations with cardiovascular disease phenotypes and lipid factors. Eye Vis (Lond) 3: 34.
- Bowes Rickman C, Farsiu S, Toth CA, Klingeborn M (2013) Dry age-related macular degeneration: mechanisms, therapeutic targets, and imaging. Invest Ophthalmol Vis Sci 54: ORSF68-80.
- Sarkar A, Jayesh Sodha S, Junnuthula V, Kolimi P, Dyawanapelly S (2022) Novel and investigational therapies for wet and dry age-related macular degeneration. Drug Discov Today 27: 2322-32.
- Rubner R, Li KV, Canto-Soler MV (2022) Progress of clinical therapies for dry age-related macular degeneration. Int J Ophthalmol 15: 157-66.
- Fleckenstein M, Mitchell P, Freund KB, Sadda S, Holz FG (2018) The Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration. Ophthalmology 125: 369-90.
- Angulo J, Peiro C, Romacho T, Fernández A, Cuevas B et al. (2011) Inhibition of vascular endothelial growth factor (VEGF)-induced endothelial proliferation, arterial relaxation, vascular permeability and angiogenesis by dobesilate. Eur J Pharmacol 667: 153-9.
- Ozaki E, Campbell M, Kiang AS, Humphries M, Doyle SL, Humphries P (2014) Inflammation in age-related macular degeneration. Adv Exp Med Biol 801: 229-35.
- Ribeiro ML, Seres AI, Carneiro AM, Stur M, Zourdani A et al. (2006) DX-Retinopathy Study Group. Effect of calcium dobesilate on progression of early diabetic retinopathy: a randomised double-blind study. Graefes Arch Clin Exp Ophthalmol 244: 1591-600.
- Bogdanov P, Sola-Adell C, Hernandez C, Garcia-Ramírez M, Sampedro J et al. (2017) Calcium dobesilate prevents the oxidative stress and inflammation induced by diabetes in the retina of db/db mice. J Diabetes Complications 31: 1481-90.
- Voabil P, Liberal J, Leal EC, Bauer J, Cunha-Vaz J et al. (2017) Calcium Dobesilate Is Protective against Inflammation and Oxidative/Nitrosative Stress in the Retina of a Type 1 Diabetic Rat Model. Ophthalmic Res 58: 150-61.
- Cuevas P, Outeirino LA, Ramos J, Angulo J, Giménez-Gallego G (2019) Single intravitreal etamsylate injection for the treatment of choroidal neovascular membrane formation in neovascular age-related macular degeneration. MOJ Clin Med Case Rep 9: 1-3.
- Cuevas P, Outeirino LA, Angulo J, Gimenez-Gallego G (2012) Treatment of dry age-related macular degeneration with dobesilate. BMJ Case Rep 2012:bcr0220125942.
- Abidi M, Karrer E, Csaky K, Handa JT (2022) A Clinical and Preclinical Assessment of Clinical Trials for Dry AgeRelated Macular Degeneration. Ophthalmol Sci 2: 100213.
- Li L, Yu Y, Lin S, Hu J (2022) Changes in best-corrected visual acuity in patients with dry age-related macular degeneration after stem cell transplantation: systematic review and meta-analysis. Stem Cell Res Ther 13: 237.
FIGURE 1
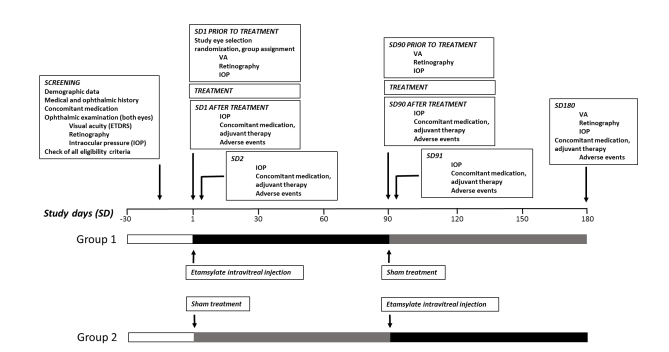
Figure 1: Schematic representation of Jericho-D study design
FIGURE 2
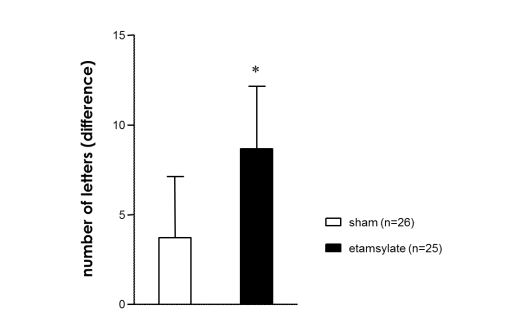
Figure 2: Intravitreal injection of etamsylate improves visual acuity in patients with dry age-related macular degeneration at 90 days follow-up
Tables at a glance
Figures at a glance