Immunogenicity Analysis of the Lytic Mycobacteriophage Preparation
Received Date: September 20, 2024 Accepted Date: October 20, 2024 Published Date: October 23, 2024
doi: DOI: 10.17303/ejmrc.2024.6.105
Citation: Avdeev VV, Vladimirsky MA, Rybina OA, Tiulkova TE, Nikitina NA (2024) Immunogenicity Analysis of the Lytic Mycobacteriophage Preparation. Eur J Med Res Clin Trials 6: 1-7
Abstract
The immune response to the injection of the liposomal form of lytic mycobacteriophages D29 on a model of intact nonlinear mice was studied. In particular, the formation of specific antibodies that could potentially inactivate the effectiveness of the studied drug was studied using enzyme immunoassay. The level of induced antibodies to mycobacteriophage did not exceed a titer of 1:16. Inhibition of the lytic, plaque-forming activity of the bacteriophage in vitro was also found to be no more than twice as a result of incubation with native immune plasma.
Keywords: Mycobacteriophages D29; Immune Responses; Specific Antibodies; Inhibition of the Lytic Activity of the Mycobacteriophages
Introduction
The uncontrollable increase in antimicrobial resistance recorded in the 21st century requires the search for new means to combat bacterial infection [1]. One of the most promising areas is therapy using specific bacteriophages [2]. Historically, only a few countries in the world, including Georgia, Russia and Poland, continue to use bacteriophages for therapeutic purposes, mainly for the treatment of intestinal infections [3], diseases of the ear, throat, nose organs [4], mycobacteriosis [5], etc. In silico studies [6] the possibility of using mycobacteriophages in the treatment of tuberculosis (TB) is being considered. The mycobactericidal effect of mycobacteriophages is due to their ability to multiply in the presence of metabolically active M. tuberculosis with their subsequent lysis.
To improve the penetration of mycobacteriophages into granulomas in order to increase their bactericidal activity, packaging of bacteriophages in liposomes is used [7]. Experimental studies [8,9] have shown a significant lytic effect of the liposomal form of mycobacteriophage D29, both on a model of tuberculous granuloma formed by human mononuclear blood cells in vitro, and on a model of tuberculosis infection in C57BL/6 mice. Considering that bacteriophages are used to create therapeutic biopreparations [10], attention should be paid to the specific characteristics of the preparations created on their basis, including the formation of antibodies that can have a negative impact on the effectiveness of treatment. Due to the formation of neutralizing antibodies, the effectiveness of using biopreparations based on monoclonal antibodies, cytokines used primarily for the treatment of diseases of non-infectious etiology decreases: rheumatoid arthritis, psoriasis, cancer, etc. [11-13]. Interaction between the pathogen and bacteriophages in the case of development of complex multicomponent reactions in humans with subsequent feedback [10]. Due to detection of bacteriophage proteins in macroorganisms, the development of characteristic antibodies is also possible. There are reports of this in isolated cases of mycobacteriosis [14], as well as in the treatment of diseases of other bacterial etiologies [15]. Thus, immunogenicity risks are subject to mandatory control at all stages of the development of biotechnological drugs [16].
Considering that mycobacteriophage is a virus with polypeptide proteins in its structure, the human body can consider it as an antigen and, as a result of the immune response, specific antibodies can be synthesized to bind to the bacteriophage as an antigen. Based on this, a hypothesis was formed that repeated administration of the biopreparation can be accompanied by the formation of specific antibodies that bind mycobacteriophage proteins, thereby reducing its effectiveness.
To test this hypothesis, the goal was set to evaluate the formation of specific antibodies in the plasma of laboratory animals with repeated administration of a liposomal preparation of mycobacteriophages and their effect on lytic activity.
Materials and Methods
Study preparation: liposomal preparation of mycobacteriophage D29 with a liposome size of 0.8 μm was produced by extrusion according to the standard technique from a preparation of mycobacteriophage D29 purified by ion chromatography with subsequent dialysis [8], the activity of which was 108 plaque-forming units/ml (lysis zones,PFU/ml). The preparation was a colloidal solution containing liposomes with included bacteriophage. Inclusion of bacteriophage in liposomes was 40%; phage not included in liposomes, accordingly, constituted 60% of the total amount of mycobacteriophage.
The studied samples: plasma of male outbred mice, which were injected intraperitoneally with the liposomal mycobacteriophage D29 at a dose of 330 mg/kg (3.3 ˣ108 PFU/kg) daily for 20 days – the experimental group or solvent (phage buffer solution - FBS: 0.1 M Tris-HCl MgSO4 0.1 M NaCl pH 7.5) – the control group. Each sample represents a plasma pool from 25 individuals of the experimental group or 10 individuals of the control group.
Microbiological Analysis
The presence of specific antibodies was determined by changing the titer and biological activity of the mycobacteriophage after incubation with the experimental plasma. The titer of the mycobacteriophage was determined by tenfold titration on plates with M.smegmatis. The biological activity of the mycobacteriophage was determined by multiplying the number of obtained plaque-forming units (lysis zones on plates with a lawn of M.smegmatis) by the corresponding dilution. The preparation of mycobacteriophage D29 with an activity of 106 PFU/ml in a volume of 10 μl was incubated with the plasma of immune animals, animals of the control group and with FBS - (K-) 90 μl for 30 minutes at 37oC. The mycobacteriophage titer was then determined by counting the colonies grown in a tenfold titration on plates with M.smegmatis. In addition, the amount of mycobacteriophage D29 was determined in the titrated samples using RT-PCR.
Immunological Analysis
Determination of the presence of specific antibodies using enzyme immunoassay [17]. Optimized for mycobacteriophages.
Pre-purified mycobacteriophage preparation with an activity of 108 PFU/ml with carbonate-bicarbonate buffer pH=9.6, in a 1:1 dilution was applied to the wells of a polystyrene flexible plate (TiterTek) in a volume of 100 μl/well; incubated for 2 hours in a thermostat at 37oC. Then the wells were washed 4 times with 200 μl of FBS with 1% Tween 20. All wells were filled with a 2% bovine serum albumin solution in a volume of 100 μl/well, incubated for 1 h at 25oC and washed once with distilled water in a volume of 200 μl/well. Then, dilutions of immune and control plasma were prepared with a diluting buffer solution in ratios of 1:1- 1:128, a total of 7 points, and added in duplicate to the wells of the plate in a volume of 100 μl. After incubation for 1 hour at 37oC and washing, staphylococcal protein A conjugate with horseradish peroxidase P-S Paa was added to all wells and incubated for 30 min at 37oC. Then they were washed as standard, a substrate buffer solution was added in a ratio of 7:1; After 30 min, the reaction was stopped to read the optical density on a spectrophotometer (BIO-RADModel 680) at a wavelength of 450 nm.
Results
According to the experimental data, minor changes were observed, within one order of magnitude, in the activity of the mycobacteriophage when determining its titer on a solid nutrient medium on plates with a lawn of M.smegmatis.
The obtained data on determining the vitality of the bacteriophage during incubation with animal plasma are presented in Table 1 and Figure 1.
Table 2 presents the results of PCR analysis of the bacteriophage DNA content in the experimental samples. A decrease in the amount of mycobacteriophage DNA is expressed in an increase in the threshold PCR cycles relative to the control group by more than 1 unit.
According to the PCR analysis data, there are no differences in the mycobacteriophage content in the control and experimental plasma, which confirms the absence of the effect of antibodies on the phage DNA content.
Table 3 presents results of antibody determination using the enzyme-linked immunosorbent assay (ELISA) - optical density indicators in the wells of the plate for the control and immune groups of animals
Discussion
The obtained results indicate the presence of specific antibodies to mycobacteriophage. This may be due to the presence of bacteriophage in the studied preparation in a form not included in liposomes. In the study by Luvi et al. [18], it was shown that liposomal packaging of the preparation prevents the appearance of specific antibodies. Gembara K et al. [19] studied the primary immune response of the body to bacteriophages and showed the formation of IgM immunoglobulins after taking the bacteriophage for a week, IgG immunoglobulins - after 2-4 weeks, IgA - after 2-3 months. Considering that the duration of therapy with the developed preparation was 20 days, the authors detected specific IgG. It is important to note that antibodies to bacteriophages are mainly polyclonal, due to the multicomponent protein structure of epitopes [20] and do not always lead to a neutralizing effect. This was proven in the described experiment using the microbiological method of analysis. However, the presence of such a quantity of antibodies does not affect the lytic activity of mycobacteriophage D29 since the decrease in titer relative to the control and control plasma is observed within the same order. The biological activity of the phage incubated with the control plasma was 1.9×108 PFU/ml; with the experimental one - 1×108 PFU/ml.
Conclusion
The conducted experiment demonstrated the possibility of antibody formation after multiple (for 20 days, daily) administration of a biotherapeutic drug based on mycobacteriophage. This is probably due to the presence of free bacteriophage in the liposomal drug. Moderate immunogenicity did not affect its bactericidal activity against mycobacteria, which indicates possible good prospects for the future clinical use of the developed drug. The degree and nature of the immune response are generally phage-specific [21]. In the course of clinical studies, it was shown that the immune response to phage therapy was often lower than expected and did not lead to a significant decrease in the effectiveness of therapy or adverse events [22, 23]. Thus, the results of the work are consistent with the literature data, the demonstrated moderate immunogenicity of the drug after 20 days of daily administration is not an obstacle to therapeutic use [24]. Moreover, the expected regimen for the use of the drug in the clinic will be shorter and lower in phage load, which, in turn, will have a positive effect on the issues of immunogenicity [25]. The data presented in the work are part of preclinical studies of the safety of therapy using lytic mycobacteriophages.
- Marc Mendelson, Joseph A Lewnard, Mike Sharland et al. (2024) Ensuring progress on sustainable access to effective antibiotics at the 2024 UN General Assembly: a target-based approach, The Lancet, 403: 2551-64
- Osman AH, Kotey FCN, Odoom A et al. (2023) The Potential of Bacteriophage-Antibiotic Combination Therapy in Treating Infections with Multidrug-Resistant Bacteria. Antibiotics, 12: 1329.
- Jin Y, Li W, Zhang H, et al. (2023) The Post-Antibiotic Era: A New Dawn for Bacteriophages. Biology (Basel). 12: 681.
- Kakasis A, Panitsa G (2019) Bacteriophage therapy as an alternative treatment for human infections. A comprehensive review. Int J Antimicrob Agents. 53: 16-21.
- Dedrick RM, Guerrero-Bustamante CA, Garlena RA et al. (2019) Engineered bacteriophages for treatment of a patient with a disseminated drug-resistant Mycobacterium abscessus. Nat Med. 25: 730-3
- Ana PB. Silva1, Christian S et al. In silico Bacteriophage D29 characterization of potential specific antimicrobial peptides against Mycobacterium tuberculosis and their phage-loaded in vitro activity in nanoliposomes against infected macrophages.
- Subramanian A (2024) Emerging roles of bacteriophage-based therapeutics in combating antibiotic resistance. Front Microbiol.
- Avdeev VV, Kuzin VV, Vladimirsky MA, Vasilieva IA (2023) Experimental Studies of the Liposomal Form of Lytic Mycobacteriophage D29 for the Treatment of Tuberculosis Infection. Microorganisms, 11: 1214.
- Lapenkova MB, Alyapkina YS, Vladimirsky MA (2020) Bactericidal Activity of Liposomal Form of Lytic Mycobacteriophage D29 in Cell Models of Tuberculosis Infection In Vitro. Bull Exp Biol Med. 169: 361-4.
- Perepanova TS et al. (2021) Therapeutic Use of Bacteriophages Clinical Microbio and Antimicrobial Chemotherapy, 23: 55-65
- Dalakas MC (2022) Role of complement, anti-complement therapeutics, and other targeted immunotherapies in myasthenia gravis. Expert Rev Clin Immunol. 18: 691-701.
- Bittner B, Schmidt J (2024) Advancing Subcutaneous Dosing Regimens for Biotherapeutics: Clinical Strategies for Expedited Market Access. BioDrugs. 38: 23-46.
- Penny HL, Hainline K, Theoharis N et al. (2023) Characterization and root cause analysis of immunogenicity to pasotuxizumab (AMG 212), a prostate-specific membrane antigen-targeting bispecific T-cell engager therapy. Front Immunol. 14: 1261070.
- Dedrick RM, Smith BE, Cristinziano M, et al. (2023) Phage Therapy of Mycobacterium Infections: Compassionate Use of Phages in 20 Patients with Drug-Resistant Mycobacterial Disease. Clin Infect Dis. 76: 103-12.
- Pagava KI, Gachechiladze KK, Korinteli IA, et al. (2011) What happens when the child gets bacteriophage per os? Georgian Med News. 196-7: 101-5.
- Avdeeva Zh I, Soldatov AA, Bondarev VP, Mosyagin VD, Merkulov VA (2021) Problems associated with the manifestation of immunogenicity of biotherapeutic proteins and ways to solve them. Immunology, 42: 706-19.
- Bochkareva SS, Karaulov AV, Aleshkin AV et al. (2019) Methodological approaches to assessing some parameters of the humoral and cellular immune response to bacteriophages. Clinical laboratory diagnostics. 64: 237-42.
- Luwi, Nur Ellene Mat; Ahmad, Suhana; Azlyna, Ahmad Suhaimi Nurfatihah et al. (2022) Liposomes as immunological adjuvants and delivery systems in the development of tuberculosis vaccine: A review January 2022 Asian Pacific Journal of Tropical Medicine, 15: 7.
- Gembara K, Dąbrowska K (2021) Phage-specific antibodies. Curr Opin Biotechnol. 68: 186-92.
- Dabrowska K, Miernikiewicz P, Piotrowicz A, et al. (2014) Immunogenicity studies of proteins forming the T4 phage head surface. J Virol. 88: 12551-7.
- Van Belleghem JD, Dabrowska K, Vaneechoutte M, et al. (2018) Interactions between bacteriophage, bacteria, and the mammalian immune system. Viruses, 11.
- Bruttin A, Brussow H (2005) Human volunteers receiving Escherichia coli phage T4 orally: a safety test of phage therapy. Antimicrob Agents Chemother, 49: 2874-8.
- Kaźmierczak Z, Majewska J, Miernikiewicz P, et al. (2021) Immune Response to Therapeutic Staphylococcal Bacteriophages in Mammals: Kinetics of Induction, Immunogenic Structural Proteins, Natural and Induced Antibodies. Front Immunol. 12: 639570.
- Zou G, He L, Rao J, et al. (2023) Improving the safety and efficacy of phage therapy from the perspective of phage-- mammal interactions. FEMS Microbiol Rev. 47: fuad042.
- Łusiak-Szelachowska M, Międzybrodzki R, Rogóż P et al. (2022) Do Anti-Phage Antibodies Persist after Phage Therapy? A Preliminary Report. Antibiotics (Basel). 11: 1358.
FIGURE 1
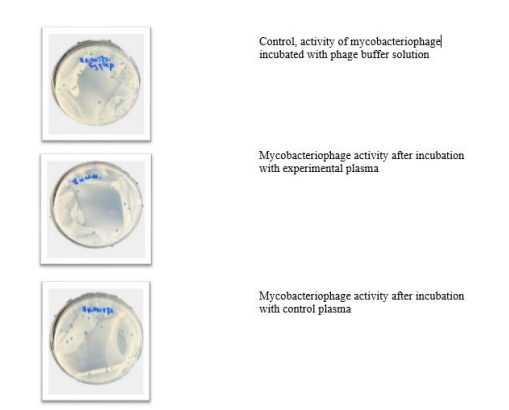
Figure 1: Representative images of mycobacteriophage D29 PFU on a solid nutrient medium with M.smegmatis after incubation with animal plasma after a 20-day administration of the liposomal bacteriophage preparation.
Tables at a glance
Figures at a glance