The Effect of Shared Decision-Making Cognition on Value Co-creation and the Motivation and Behavior of Patients during Value Co-creation Engagement
Received Date: February 10, 2024 Accepted Date: March 10, 2024 Published Date: March 13, 2024
doi: 10.17303/ijnsp.2024.1.101
Citation: Yu-Hua Yan, Shih-Chieh Fang, Chih-Ming Kung (2024) The Effect of Shared Decision-Making Cognition on Value Co-creation and the Motivation and Behavior of Patients during Value Co-creation Engagement. Int J Nur Man Pat Car 1: 1-13
Abstract
Background: In 2016, Taiwan embraced the Shared Decision-Making (SDM) concept to shift from a one-way authoritative healthcare model to a collaborative approach, fostering two-way communication and addressing the strained doctor–patient relationship.
Purpose: Positioning SDM as the catalyst for value co-creation, this study explores the influence of SDM cognition on value co-creation. Additionally, the research evaluates patient motivation and behavior in SDM.
Methods: Utilizing questionnaires distributed among SDM participants, we analyzed data from 173 valid responses using the chi-square test, Pearson correlation analysis, and path analysis.
Results: Significant correlations were observed: SDM cognition correlated passively with participation behavior (p< 0.001); stronger participant motivation and behavior led to increased value co-creation (p< 0.001); heightened interaction positively impacted doctor–patient value co-creation (p< 0.001).
Conclusions: Sustained SDM promotion enhances patients' information-seeking and sharing behaviors, improves doctor–- patient interactions, and aligns with governmental SDM policies.
Patient or Public Contribution: Patients actively participated in study design, recruitment, and analysis, emphasizing the collaborative nature of SDM and its impact on healthcare dynamics.
Keywords: Shared Decision-Making; Cognition; Motivation; Behavior During Engagement; Value Co-Creation
Introduction
Assistance for and collaboration with patients in pursuing the greatest value and setting the patient’s ultimate treatment effect as the prime goal are the new strategic thoughts of medical institutions [1]. The doctor–patient relationship (DPR) refers to the interaction between doctors and patients [2], which is a multidimensional social relationship [3]. As the DPR evolves, patients have changed their roles in the self-maintenance or self-promotion of health from the “passive audience” into the “active co-producer.” Instead of the past medical authority model, customer engagement is encouraged for value co-creation [4,5].
Taiwan’s Ministry of Health and Welfare (MOHW) began to actively implement and use Shared decision-- making (SDM) in 2016 and set the year as the year zero of SDM. Apart from encouraging medical institutions nationwide to support and promote the SDM concept, the MOHW established an SDM Platform for hospitals to promote resource sharing and reduce resource wastage [6]. Goal #8 in the “Hospital Healthcare Quality and Patient Safety Goals 2018–2019” that the MOHW announced in 2018 is to “provide the public with multiple participation channels, encourage the public to care about patient safety and promote SDM, promote sound doctor–patient communication, encourage active participation in healthcare decision-making of patients and family, and thereby enhance healthcare quality and reduce healthcare disputes” [7].
SDM gives patients greater choice over their healthcare [8]. An SDM approach may be applicable to a variety of treatment-related decisions and patient issues, including but not limited to the selection of specific treatment options [9]. To be essential for good SDM to occur, because it creates the feeling of safety, respect and trust that patients need to be actively involved in the decision-making process [10-12].
SDM is by nature a type of evidence-based risk communication for doctors and patients to reach a consensus over the interests, risks, advantages, disadvantages, and uncertainties. Hence, in SDM, both parties share information: the clinicians offer options and describe their risks and benefits, and the patients express their preferences and values [13,14]. SDM resolved decisional conflicts and improved decision self-efficacy [15]. Healthcare personnel must provide patients with the necessary assistance, guide them to choose the healthcare options that meet their own preferences in a well-informed condition, and track the performance of their options to make win-win decisions for both doctors and patients [16,17]. Key characteristics of SDM are as follows: (1) at least two participants (physician and patient) are involved; (2) both parties share information; (3) both parties take steps to build a consensus on the preferred treatment; and (4) an agreement is reached on the treatment to be implemented [14].
Value co-creation is a new link between organizations (participants) encouraging participants to create value mutually [18,19]. While value co-creation between doctors and patients is emphasized in the treatment process, this can be considered the value of collective collaboration between suppliers and consumers of healthcare [20,21]. Thus, SDM highlights how healthcare consumers maintain close interaction with healthcare providers to create a unique and exclusive experience, thereby creating and acquiring value mutually (together) [22,23] to practice value co-creation between the government/healthcare providers and healthcare consumers. The promotion and deepening of the SDM concept can promote doctor–patient interaction and set the paradigm of co-creation [24].
Although many studies have reported on SDM, most focused on the experience or skills in clinical implementation [25,26].As only a few empirical studies have explored the effects of the cognition and implementation of SDM on value co-creation and the motivation and behavior of patients during participation in SDM [27], this study collects, analyzes, and concludes empirical data through a questionnaire survey and makes practical recommendations for future SDM development.
Methods
Research Design
The research employed a cross-sectional design to capture a snapshot of physicians' views on Shared Decision-- Making (SDM). A structured questionnaire was chosen to facilitate a systematic and efficient collection of data from a diverse group of participants.
Rationale for Questionnaire Survey
The questionnaire survey method was selected for its ability to quantify physicians' perspectives on SDM in a standardized format. This approach allowed for a broad and uniform assessment, ensuring consistency in data collection across a varied sample.
Data sources and research variables
The research questionnaire was designed based on the related literature. To enhance the validity of the questionnaire, apart from conducting a pretest on 30 SDM participants and reviewing the results with scholars and field experts, we rephrased ambiguous questionnaire items before the survey was conducted between March 2020 and May 2020. This study distributed the questionnaire to 296 respondents and received 173 responses with a response rate of 58.45%.
To ensure that the survey has no non-response bias, we performed the F-test to analyze the two groups of respondents (non-respondents and respondents) to determine whether a significant difference among all variables exists. The results showed that the F-value of each variable is insignificant, suggesting no significant bias.
Reliability and validity
In reliability analysis, we measured the fairness of reliability using Cronbach’s α [28], the composite reliability (CR) using confirmatory factor analysis (CFA), and the average variance extracted (AVE) [29]. According to the recommendations by Cuieford [30] and Nunnally [29], the internal consistency is high when the Cronbach’s α is >0.7, and reliability is low when the Cronbach’s α is < 0.35. According to Bagozzi and Yi [29], the internal consistency is fair only when the CR is greater than 0.6 and the AVE is greater than 0.5 for all variables. We measured the convergence validity of all variables using the CFA. Good convergence validity requires that (1) standardized factor loading must be significant and greater than 0.4, which is the acceptable range of validity [30], and a value of 0.5–0.95 suggests high validity [29]; (2) the CR must be greater than 0.6 [30]; and (3) the AVE must be greater than 0.5 [30]. This study has used a Likert five-point scale for respondents to measure their agreement with each item from 1 to 5.
Common Method Variance
To prevent same-source bias under the common method variance (CMV) of this study from reducing the reliability of the conclusions, we have enhanced the reliability of the research results through the questionnaire design (reverse item coding, respondent de-identification, and item context concealment) [31]. In addition, we determined the CMV using Harman’s one-factor test. As this study has used respondent de-identification, reverse item coding, and item context concealment to prevent reliability reduction of the conclusions, the CMV has been reduced through the questionnaire design. As claimed by scholars, Harman’s one-factor test discerns whether all questionnaire items could extract multiple variables required by the research topic using principal component analysis (PCA). If a major factor could explain the majority covariance of all variables, a CMV exists among variables [31]. Thus, we performed the PCA on all questionnaire items and extracted 10 factors (not one factor) without rotation from the results. As the eigenvalue of each factor is greater than 1 and the cumulative variance explained is 47.74%, the “variance explained of individual factors” of the research variables is less than onehalf of the cumulative variance explained. In conclusion, the CMV is insignificant in this study.
Questionnaire Design and Validation
The questionnaire was meticulously developed based on a thorough review of existing literature, incorporating established constructs related to SDM. To ensure content validity, the questionnaire underwent expert reviews and pilot testing. Additionally, the reliability and validity of the questionnaire were assessed through statistical methods, including factor analysis and internal consistency measures.
Ethical Approval
The protocol was approved by the institutional review board with Good Clinical Practice guidelines, the principles of the Declaration of Helsinki, and local laws (IRB-1081101).
Results
Table 1 shows the demographic data of the 173 respondents including 116 females and 57 males: most respondents were aged between 35 and 44 years (35.3%), university graduates (51.5%), and married (71.1%) and had their last appointment with other specialties (51.5%). The research questionnaire has good reliability and validity as factor loading is >0.614, CR is >0.765, AVE is >0.495, and Cronbach’s α is >0.7 (Tables 2–3).
Table 3 consolidates the analysis results of descriptive statistics. The SD of the overall variables falls between 0.520 and 0.773; the mean of the collective value (4.85) and SDM knowledge cognition (4.38) are the highest and second highest, respectively. Table 4 shows the Pearson correlation coefficients among all variables, which are positively and significantly correlated.
We analyzed the research structure model using partial least squares to determine the strength and direction of the correlations among research variables. The results are shown in Figure 1. First, in terms of SDM cognition and participation motivation, the greater the SDM cognition is, the stronger the participation motivation will be. The research results show that SDM cognition has a positive and significant effect on participation motivation (path coefficient = 0.652; p < 0.001). Second, in terms of motivation and behavior during participation, SDM cognition has a positive and significant effect on participation behavior (path coefficient = 0.670; p < 0.001). Third, in terms of the relationship between participation behavior and value co-creation, participation behavior has a positive and significant effect on participation behavior (path coefficient = 0.744; p < 0.05). Lastly, this study found that doctor–patient interaction has a moderating effect on participation behavior and value cocreation (path coefficient = 0.799; p < 0.001) (as shown in Figure 1). In other words, the greater the SDM cognition is, the stronger the participation motivation will be. Recently, an important change has been observed in the DPR model: the stronger the patient’s motivation is, the more significant the moderating effect of doctor–patient interaction will be and the greater the effect on value co-creation.
The questionnaire was meticulously developed based on a thorough review of existing literature, incorporating established constructs related to SDM. To ensure content validity, the questionnaire underwent expert reviews and pilot testing. Additionally, the reliability and validity of the questionnaire were assessed through statistical methods, including factor analysis and internal consistency measures.
Discussion
With value co-creation as the theoretical foundation, this study proposes a theory model and proves that SDM cognition and the motivation and behavior during SDM participation have positive effects on value co-creation, and doctor–patient interaction has a moderating effect on participation behavior and value co-creation. This study found that SDM cognition and participation motivation have positive effects on value co-creation, and doctor–patient interaction and participation behavior have moderating effects on value co-creation, which are consistent with the related literature [5]. Value co-creation as the interactive communication between healthcare providers and patients facilitates the results of healthcare service provision by doctors during the interaction [32]. Therefore, doctors are willing to understand the true thoughts of patients and patients are willing to participate in the process of healthcare service provision to make a healthcare decision with doctors [33], making the doctor’s work more valuable [34]. Hence, the process of doctor–patient interaction is the key to the success of value co-creation, building a long-lasting and stable DPR for sharing common goals and missions.
Furthermore, this study found that doctor–patient interaction has a moderating effect on participation behavior and value co-creation. In participation motivation, although most literature emphasizes the claim on value cocreation [35,36], studies have proven that consumers have changed their roles from “passive audience” into “active coproducers” [35]. In addition, Zeithaml [37] has found that good-quality and satisfactory clinical results require the motivated participation of customers. Lehtinen et al., [38] have also proven that patients’ motivation to participate in value co-creation activities contributes in the success of value creation. Although participation motivation is diverse in various value co-creation activities, if we consider ways to create value in different activities, the performance will differ [36]. This study believes that patients with stronger participation motivation are more willing to engage in the process of the healthcare service provision and will have more opportunities to make positive choices based on the goals of the healthcare service. Apart from reducing the uncertainties in healthcare, participation motivation can facilitate the output of healthcare benefits. When patients lack participation motivation, no value will be co-created. This result can serve as a reference for hospitals to co-create value with patients.
Lastly, the empirical results of this study affirm the feasibility and suitability of this study’s framework and provide useful information in promoting SDM among health authorities and hospital administrators. Furthermore, a study has found that SDM can be taught and achieved using patient decision aids (PDAs) [39] and other decision support tool [40]. Health authorities and hospital administrators can improve the public’s SDM cognition to encourage the participation of patients and their families in SDM, thereby creating a unique experience and value.
Theoretical Implications
Proposing a theoretical framework for value cocreation research is the theoretical contribution of this study. Taiwan introduced and promoted the SDM concept in 2016, hoping to eliminate the one-way and authoritative healthcare model by implementing SDM, which encourages patient and family participation to achieve two-way communication and improve the increasingly tense DPR. Hence, in the healthcare industry, SDM requires patient participation. By sharing the known evidence-based medical results, both doctors and patients can make healthcare decisions through discussion based on the patients’ own preferences and value [41].
Most SDM studies in Taiwan have focused on the experience of clinical implementation and its effectiveness in clinical application, with little concern about the effect of SDM cognition on value co-creation and the motivation and behavior of participants during SDM. The promotion and practice of SDM require not only the support and participation of patients and their family but also the intervention and guidance from health professionals to maximize its effect. Therefore, this study has extended to the patients’ perspectives. The empirical results of this study affirm the feasibility and suitability of its framework and provide useful information regarding SDM implementation for the MOHW and hospital administrators. Furthermore, this study found that SDM can be taught and achieved using PDAs [39]. Health authorities and hospital administrators can improve the public’s SDM cognition to encourage the participation of patients and their families in SDM, thereby creating a unique experience and value.
Management Implications
This study found that SDM cognition has a positive and significant effect on participation behavior. Therefore, the MOHW and hospitals can enrich the SDM knowledge and improve the SDM attitude of patients through education to enhance SDM participation. In the SDM process, the patient’s health knowledge is a major factor affecting the doctor–patient consensus [42].Introducing SDM to people with less health knowledge can enrich their health knowledge, provide them with adequate information for making choices and decisions, enhance their self-efficacy in SDM participation and decision-making, and reduce decision conflicts [43]. Hence, enhancing patients’ SDM cognition can encourage patient participation in value co-creation.
Contribution to Existing Literature
Unique aspects and novel insights derived from the research are thoroughly examined and contextualized. Comparative analysis with relevant studies in the field is undertaken to underscore the distinctiveness of the current findings.
Recommendations
This study has interviewed many physicians on their views on SDM. Most physicians agree that SDM is an ideal decision-making model; however, Taiwan’s current healthcare environment is too busy to practice it in the field. Although the MOHW implemented a trial SDM program and called for nationwide hospitals to promote and use the “SDM Platform” in 2015, most hospitals still develop their own PDAs and keep data for their own. As a result, patients cannot access standardized information from a universal channel. This study recommends that the MOWH builds a well-laid platform and develops related applications to integrate the PDAs of individual hospitals and standardize information presentation for patients to acquire disease-related knowledge from the platform more conveniently and efficiently. Furthermore, this study recommends the inclusion of patients’ concerns and expectations in designing PDAs for them to understand their own preferences and value right at the beginning of information search to facilitate effective interaction and communication with physicians in an appointment.
Limitations
Although this study has attempted to collect and analyze data thoroughly, limitations are unavoidable. For example, due to the lack of steady scales for measuring SDM cognition, participation motivation and behavior, DPR, and value co-creation in the research constructs and operating variables proposed by this study, there is still room for improvement for future research. Future value co-creation research can develop a refined theoretical framework based on the findings of this study to further investigate different forms of value co-creation in terms of the DPR. Lastly, future research can include more shapable research topics.
For example, further physician sampling and patient matching can further analyze the integrity of value co-creation to enrich the sectional data and make the research results more representative. In conclusion, research topics more worthy of investigation in future studies of value creation exist. This study hopes that the findings can bring different thoughts to the problem and provide a broad scope of research thinking.
Author Contributions
Study conception and design: YHY, SCF
Data collection: YHY, CMK
Data analysis and interpretation: YHY
Drafting of the article: SCF, CMK
Critical revision of the article: YHY
Conflicts of Interest
The authors declare no conflicts of interest.
Funding
This research project was financially supported by the Ministry of Science and Technology (MOST).
Acknowledgments
The authors would like to thank the Ministry of Science and Technology (MOST), Taiwan for financially supporting this research under Contract No. MOST 109-2410-H-217-001-SSS
- Porter ME, Lee TH (2013) The strategy that will fix health care. Harv Bus Rev 91: 24-4.
- Szasz TS, Hollender MH (1956) The basic models of the doctor-patient relationship. Arch Intern Med 97: 585-92.
- Ong LML, de Haes JCJM, Hoos AM, et al. (1995) Doctor patient communication: A review of the literature. Soc Sci Med 40: 903-18.
- Banyte J, Tarute A, Taujanskyte I (2014) Customer engagement into value creation: Determining factors and relations with loyalty. Eng Econ 25: 568-77.
- McColl-Kennedy JR, Vargo SL, Dagger TS, et al. (2012) Health care customer value co-creation practice styles. J Serv Res 15: 370-89.
- Soon MS (2017) SDM hospital introduction strategy and experience sharing. J Healthc Qual 11: 16-21.
- Ministry of Health and Welfare. 2018-2019 Hospital medical quality and patient safety goals.
- Kunneman M, Hargraves IG, Sivly AL, et al. (2022) Co-creating sensible care plans using shared decision making: Patients’ reflections and observations of encounters. Patient Educ Couns 105: 1539-44.
- Hargraves IG, Fournier AK, Montori VM, et al. (2020) Generalized shared decision making approaches and patient problems. Adapting AHRQ’s SHARE Approach for Purposeful SDM. Patient Educ Couns 103: 2192-9.
- van der Weijden T, Post H, Brand PL, et al. (2017) Shared decision making, a buzz-word in the Netherlands, the pace quickens towards nationwide implementation…. Z Evid Fortbild Qual Gesundhwes 123: 69-74.
- van Veenendaal H, van der Weijden T, Ubbink DT, et al. (2018) Accelerating implementation of shared decision-- making in the Netherlands: an exploratory investigation. Patient Educ Couns 101: 2097-104.
- Driever EM, Stiggelbout AM, Brand PL (2020) Shared decision making: physicians’ preferred role, usual role and their perception of its key components. Patient Educ Couns 103: 77-82.
- Barry MJ, Edgman-Levitan S (2012) Shared decision making-pinnacle of patient-centered care. N Engl J Med 366: 780-1.
- Charles C, Gafni A, Whelan T (1997) Shared decision-making in the medical encounter: What does it mean?(or it takes at least two to tango). Soc Sci Med 44: 681-92.
- Ho YF, Chen YC, Huang CC, et al. (2020) The effects of shared decision making on different renal replacement therapy decisions in patients with chronic kidney disease. J Nurs Res 28: e109..
- Elwyn G, Durand MA, Song J, et al. (2017) A three- -talk model for shared decision making: Multistage consultation process. BMJ 359: J4891.
- Lee YK. SDM clinical implementation and guidance skills. J Healthc Qual 2017; 11: 22-4. [in Chinese]
- Tiwana A (2014) Platform ecosystems: Aligning architecture, Governance, and strategy.
- Van Alstyne MW, Parker GG, Choudary SP (2016) Pipelines, Platforms, and the new rules of strategy. Harv Bus Rev 94: 54-62.
- Barrett M, Oborn E, Orlikowski W (2016) Creating value in online communities: The sociomaterial configuring of strategy, platform, and stakeholder engagement. Inf Syst Res 27: 704-23.
- Bridoux F, Stoelhorst JW (2016) Stakeholder relationships and social welfare: A behavioral theory of contributions to joint value creation. Acad Manage Rev 41: 229-51.
- Grönroos C, Voima P (2013) Critical service logic: Making sense of value creation and co-creation. J Acad Mark Sci 41: 133-50.
- Vargo SL, Lusch RF (2016) Institutions and axioms: An extension and update of service-dominant logic. J Acad Mark Sci 44: 5-23.
- Ramaswamy V, Ozcan K (2014) The co-creation paradigm.
- Bunn F, Goodman C, Russell B, et al. (2018) Supporting shared decision making for older people with multiple health and social care needs: A realist synthesis. BMC Geriatr 18: 165.
- Nijhuis FA, Elwyn G, Bloem BR, et al. (2018) Improving shared decision-making in Advanced Parkinson’s disease: Protocol of a mixed methods feasibility study. Pilot Feasibility Stud 4: 94.
- Osei-Frimpong K, Wilson A, Lemke F (2018) Patient co-creation activities in healthcare service delivery at the micro level: The influence of online access to healthcare information. Technol Forecast Soc Change 126: 14-27.
- Cuieford JP (1965) Fundamental Statistics in Psychology and Education.
- Bagozzi R, Yi Y (1988) On the evaluation of structural equation models. J Acad Mark Sci 16: 74-94.
- Hair JF, Black WC, Babin BJ, et al. (2010) Multivariate data analysis. ISBN 13: 978-0138132637.
- Podsakoff PM, MacKenzie SB, Lee JY, et al. (2003) Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol 88: 879.
- Payne AF, Storbacka K, Frow P (2008) Managing the co-creation of value. J Acad Mark Sci 36: 83-96.
- Lee D (2019) Effects of key value co-creation elements in the healthcare system: focusing on technology applications. Serv Bus 13: 389-417.
- Pieterse AH, Stiggelbout AM, Montori VM (2019) Shared decision making and the importance of time. JAMA 322: 25-6.
- Fernandes T, Remelhe P (2016) How to engage customers in co-creation: customers’ motivations for collaborative innovation. J Strateg Mark 24: 311-26.
- Roberts D, Hughes M, Kertbo K (2014) Exploring consumers' motivations to engage in innovation through cocreation activities. Eur J Mark 48: 147-69.
- Zeithaml VA (1981) How consumer evaluation processes differ between goods and services. 1981; In Donnelly J. H., & George W. R. (Eds.), Marketing of Services (pp189-190.) Chicago: American Marketing Association.
- Lehtinen J, Peltokorpi A, Artto K (2019) Megaprojects as organizational platforms and technology platforms for value creation. Int J Proj Manag 37: 43-58.
- Legare F, Thompson-Leduc P (2014) Twelve myths about shared decision making. Patient Educ Couns 2014; 96: 281-6.
- Yu CH, Ke C, Jovicic A, et al. (2019) Beyond pros and cons–developing a patient decision aid to cultivate dialog to build relationships: insights from a qualitative study and decision aid development. BMC Med Inform Decis Mak 19: 1-12.
- Hoffmann T, Legare F, Simmons M, et al. (2014) Shared decision making: What do clinicians need to know and why should they bother? Med J Aust 201: 35-9.
- Wang YW (2016) SDM-decision aid tool and clinical application. J Healthc Qual 10: 15-24.
- Durand MA, Carpenter L, Dolan H, et al. (2014) Do interventions designed to support shared decision-making reduce health inequalities? A systematic review and meta-analysis. PloS One 9: e94670.
FIGURE 1
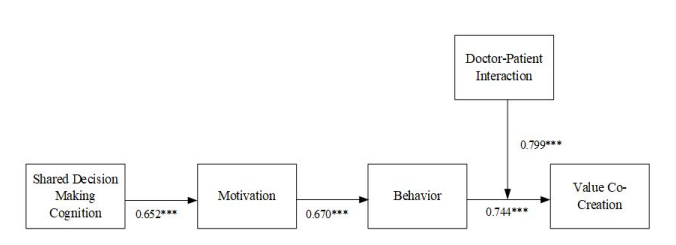
figure:1 Path analysis
Tables at a glance
Figures at a glance