Costing Health Care Associated Infections: Meta-analysis and modelling of selected African Countries
Received Date: May 20, 2024 Accepted Date: June 20, 2024 Published Date: June 23, 2024
doi: 10.17303/ijnsp.2024.1.103
Citation: Daniel Epeh (2024) Costing Health Care Associated Infections: Meta-analysis and modelling of selected African Countries. Int J Nur Man Pat Car 1: 1-8.
Abstract
Although about a fifth of all in-patient clients in health care facilities in Africa are exposed to nosocomial infections (NI) with an average mortality of 9 percent, less than a third of all countries in Africa have ever carried out NI studies. Already encumbered by staggering bottlenecks, African health systems cannot afford additional inefficiencies. There is a need to address the paucity of evidence on the true cost of NI in Africa.
The study aimed to review the evidence on the economic effects of all-cause NI in Africa and to estimate the cost of NI in Ghana. Our systematic review searched PubMed and the Africa Journal Online databases using the following keywords: ‘Health Care Associated (or Nosocomial)’ AND ‘Infections’ AND ‘Cost (or Economic Impact)’ AND ‘Length of Stay’. Studies in French and English were included if they contained LOS or pecuniary data.
Following full text data extraction, 13 relevant publications of diverse quality from 10 countries in Africa were reviewed. Studies were mainly retrospective, had relatively small sample sizes and presented only descriptive statistics. Studies hardly reported comprehensive cost categories (direct/indirect, adult/paediatric, pathogen specific) or geographies. NI costs in for Ghana the year 2019 show a significant burden, totalling almost half of all locally funded health expenditure ($414,503,004). NI costing literature is extremely limited in Africa. Although the quality of publications is generally weak, some more recent studies show improvements. Methodological standardisation and enhanced infection control protocols are needed.
Keywords: Costing Nosocomial Infections; Cost of Health Care Associated Infections; Length of Stay; Health Expenditure; HAI, HCAI Expenditure
Introduction
When Imhotep isolated honey, resins and metals for their antimicrobial action in the treatment and management of wounds almost 5,000 years ago[1] in ancient Egypt, he was privy to the dynamics of infection control. His insight continues to be strikingly contemporaneous with the recent inroads into the biocidal efficacy of nanoparticles of zinc, copper and silver recently deployed in antimicrobial coatings in healthcare settings [2]. These millennial techniques still hold significant promise for diminishing pathogen transmission today, especially during the ongoing COVID-19 pandemic, particularly with respect to shielding common surfaces such as door handles, tables and other hard surfaces [3, 4] in public places including health facilities.
Further clarity on nosocomial or Health Care Associated Infections (HCAI or HAI) was achieved thanks to Holmes and Semmelweiss [5, 6] who expanded understanding of the condition in the mid-1800s theorising on the aetiology of puerperal fevers, a post-partum infection of the female reproductive tract following childbirth or miscarriages. Their recommendation to placate the vectors of microbial remain relevant today, i.e. hand hygiene[6, 7]. Regrettably many health care workers (HCW) and physicians in particular, fail to comply with this basic infection control mechanism [8, 9] with catastrophic consequences for immune compromised patients given the significant HIV burden in Africa [6, 10, 11].
Global NI prevalence and incidence in 2010 were reported at 3-21 percent and 5-10 percent respectively [6, 12]. In Africa the highest prevalence of HCAI (specifically surgical site infections - SSI) was reported at 25 percent in Nigeria[13]. In Ghana, the Komfo-Anokye Teaching hospital reported almost 87 percent prevalence of NI in a 4 year study of 248 post-operative complications in the year 2007 [14]. The socio economic impact of these NI is noteworthy since HCAI account for a significant part of patient mortality and morbidity and in some cases are responsible for more than sixty percent of ICU costs [15].
Seen under the prism of mortality, NI loom even larger. HCAI related mortality globally has been estimated at double that of community acquired infections over the past decade. In the US for example, community onset bacteraemia triggered mortality was reported at 10-13 percent while nosocomial bacteraemia fatality rate was 23 percent[16]. Departmental and geographic differentials are also noted. Critical care units (ICU) as opposed to other departments (25 percent v 11 percent) [17], less developed versus more developed (24 versus 53 percent in a 2011 paediatric study in Kenya[16] whereas a similar study reported NI fatality rate at 7.4 in South Africa[18]). This appears paradoxical since health facilities are designed to restore, protect and promote health.
Definition
HCAI are distinguishable from conditions with a community onset (incubation triggered prior to admission into health facility). An infection triggered 48 hours after admission into a health facility is said to be nosocomial, regardless of the services sought or received. The diagnostic window escalates to 72 hours in the case of neonates [19].
HCAI are also defined with respect to health care facility discharge. A readmission and/or identification of an infection which occurs up to 30 days after surgery or 12 months in the case of prostheses or implants may be identified as being health care associated [15, 20].
Problem
African health systems are already burdened by multiple bottlenecks; low insurance coverage and high out-of-pocket payments[21, 22], demographic and epidemic transitions (Maghreb and middle income SSA)[23], the burden of HIV, weak infrastructure as well as logistical and human resource challenges[9]. Even though the Maghreb (<50 percent coverage)[21, 23], Ghana (40 percent coverage) and South Africa have had diverse health insurance systems with particular emphasis on coverage for the indigent, the afore-mentioned constraints and other policy bottlenecks have significantly limited the scope and effectiveness of these social protection mechanisms. These countries will therefore be hard pressed to leverage additional resources to confront a looming HCAI crisis if interventions are not promptly undertaken.
In Ghana, over 90 percent of health insurance expenditure is tax funded with only 3 percent accounted for by member premiums. The country is the first to deploy a system based on the ad valorem tax (VAT) positioning it well within reach of universal access as per-capita outpatient visits to health facilities soared from 0.5 to 1.1 in the decade to 2014 [24-26]. This suggests some prospects for sustainability since the funding sourceis likely to expand with the economy. Although the Maghreb and South Africa, unlike the rest of SSA proxy Ghana’s public funding approach and a relative decrease in non-communicable diseases [18, 27, 28], significant household contributions persist for all three countries. The Maghreb and South African models remain vulnerable to discretionary policies which mediate health funding, keeping it below desirable levels although they appear better resourced in terms of infrastructure and personnel than the Ghanaian. Health systems are much weaker and insurance coverage much lower in other African countries. Kenya’s 11 percent public health insurance coverage[22] towers above all purpose insurance coverage for women in Togo (3.31%), Mada�gascar (2.23%) and Mali (2.2%). Geographical differentials even within countries are severe as depicted by the rural urban health insurance coverage gap in Niger (7.73 versus 0.54 percent)[29].
Consequently, the predecessor institution of the African Union, the Organisation of African Unity, in 2001 documented the commitment of African heads of state, meeting in Abuja, to increase funding for health systems to confront the infectious disease burden which plagued the continent. Health spending was earmarked for 15 percent of annual budgets for the first quarter of the 21st century [30]. Several reports throughout the years have revealed ebbs and flows for many countries but overall, an inability to meet this target for all but 3 countries in Africa[31, 32]. HCAI constitute an additional and a most unwelcome cost centre which further complicates the vision of mitigating the continent’s infectious disease burden.
The incidence of HCAI in Africa is on the rise and expectedly so. Notably, more recent studies estimate HCAI prevalence at levels thrice earlier reported ranges [6, 33]. Health infrastructure and coverage is expanding in tandem with the complexity of invasive procedures performed on the continent. Additionally, antibiotic stewardship programs continue to be operated at suboptimal levels midwifing in the process a looming crisis of drug resistance [15].
Indeed while the aetiology of nosocomial infections is relatively well documented [34-38], the study of their economic costs is of more recent vintage [11, 19, 33]. As at 2016, it is reported that only 20 percent of sub Saharan African countries had carried out studies in the area with a skew towards Nigeria[13]. The said studies focused on incidence, pathogenesis and other socio economic and clinical determinants of the condition as well as treatment outcomes with no reference to economic impact.
Dixon[39] in one of the earliest economic impact contributions to the field, estimated the cost of NI in the US at US$ 4.8 billion in 1978. Inflated to 2018 figures (5.48 percent/year) this amounts to US$76.54 billion [40]. Notwithstanding improvements in infection control programmes (ICP), excess direct healthcare costs of NI continue to be huge even for single organisms. Clostridium Difficile for example was estimated to cost the US health system around 7 billion US$ in 2016[41]. In contrast to the extensive work on NI costs in the developed world, in almost four decades, less than a score studies have been undertaken in the area on the continent with one of the earliest being a doctoral thesis by Samou in 2005[42]. Although estimates at facility level in a smattering of countries exist, no study to our knowledge, has comprehensively addressed the economic impact of HCAI at national or sub regional level in Africa. Additionally, whereas productivity losses in the US are estimated at US$35 billion for antibiotic resistant HCAI infections alone, no comprehensive estimates have been attempted at any indirect costs for NI in any African country [15, 43]. In the context of the current paucity of information, this study aims to contribute to the knowledge currently available on the economic burden of nosocomial infections in selected African countries.
Methods
Search Strategy
A systematic search for French and English language works with no time restriction was effected in the PubMed and Web of Science databases (via the Endnote X8© online search interface). The Africa Journal Online (Ajol) database was also queried with various configurations of the following keywords without time restrictions:
English: Health Care Associated (or Nosocomial) AND Infections AND Cost (or Economic Impact) AND Length of Stay
French: Coût (or surcoût) AND Infections associées aux soins (or Nosocomiale).
Search results were supplemented by snowballing through the reference lists of the included studies using Google Scholar.
Study selection
The design, selection, and analysis of included studies was a joint effort by the co-authors. DE developed the search strategy and was responsible for implementing the exclusion and inclusion criteria while AF reviewed each stage of the selection and analysis for fidelity to the study protocol.
Studies were included if they reported direct or indirect costs of nosocomial infections relating to human subjects. The costs were expressed either in Length of Stay (LOS) or in financial/pecuniary terms or both. Studies were included even if they focused on a single or specific pathogen or condition. Inclusion was achieved as long as the infection was considered a hospital or healthcare associated condition and control data was available to express the marginal cost attributable to the nosocomial condition.
There was no date or time restriction for published materials.
Studies were excluded if they were not conducted on the African continent and/or did not include HCAI costs. Studies which reported costs in monetary or time terms but did not disclose a non-nosocomial base for comparison were also excluded.
Guidelines, reviews, minutes, seminar and conference proceedings and reports were also excluded from the final analysis.
Data extraction
We selected articles independently in two phases (phase 1: December 2018, phase 2: January 2019). Having achieved significant overlap of selected studies in line with the selection protocol, we combined the results in February 2019 and did a final review in August 2020.
In the absence of explicit case controls (studies with matched patients not subjected to HCAI) HCAI costs were extracted from estimates in the articles themselves or computed by the reviewer by subtracting the resource use per estimated baseline conditions from the resource use under HCAI. Resource use in this review refers to length of stay (LOS) or pecuniary estimates were available or both.
The bibliographic reference of the studies, statistical methods, population information, study design and the nature of economic data reported constitute the study characteristics reported. These were collected using a form and used for quality assessment.
Disambiguation was approached such that in the presence of multiple classes or groups of cost data, matched data always took precedence over unmatched data and unit/detailed costs over subgroup costs, re-working a total from detailed unit costs when available. In the case of pooling data for country profiles, weighted averages were used for epidemiologic data including LOS to reflect the study characteristics of the component studies. Wherever applicable, weighted averages always took precedence over medians particularly when the distribution was skewed, all other aggregate data were cast as simple averages.
All cost data were inflated to Consumer Price Index (CPI) adjusted 2018 US$ equivalent prices using the Official Data Foundation’s electronic model[40].
Quality assessment
A quality trichotomy was established with studies adjudged to be of low quality when they reported neither regression nor matching methods. These also did not employ any statistical techniques to estimate association between HAI outcomes and reported determinants.
High quality studies used adjusted regressions and matched populations in estimating HCAI outcomes and determinants. All other studies made use of either matching or regression or some other bivariate techniques in isolation to measure levels of association between determinants and HCAI outcomes. These were adjudged to be of medium quality.
Results
Search results
The search strategy produced 8,090 entries declining to 13 which were included in the final analysis after full text review for eligibility. This process commenced with the elimination of duplicates and screening of titles and abstracts in search of inclusion criteria. Sixty-three full text articles were scoured for primary HCAI cost data. Relevant articles were supplemented by additional records culled from Google Scholar. Study characteristics are summarized in Table 1.
Study characteristics
Surgical and recovery wards, intensive or acute care units and neo natal facilities are regarded as epicentres for HCAI due to the underlying conditions of the patients therein[44]. For example neonates would have an immune system that is not yet developed, invasive surgical procedures would escalate the portals of entry for bacteria while HIV and its comorbidities mount a formidable challenge on any infection control mechanism that is put in place [5] .
There is concordance within the 13 selected studies with this trend as 70 percent of the health facilities which hosted the studies are either ICU or other acute care departments of advanced medical centres or University Teaching Hospitals (UTH). Fifteen percent of the studies included both advanced care facilities and lower-level facilities while the rest of the studies were comprised of exclusively lower-level facilities and maternity homes (Table 1) (Figure 1). The studies collected data ranging from as early as the year 1994 to 2017. Only thirty eight percent of the data was collected within the 3 years to 2018 and reported an average prevalence of 16 percent (n=5). The next 3-year segment ending in 2015 represented 15 percent of all data collected (n=2) and also posted an average HCAI prevalence of 16 percent. With an average HCAI prevalence of 12 percent, the remaining studies related to data collected more than 6 years prior to 2019 (n=6).
The weighted average age of patients across time has plateaued around 40 years of age since 1994, having dropped to 38 years between 2013 and 2015. Upon observation, prevalence also indicated some relationship with the technical capacity of the health facility averaging 25 percent from a low of 6.7 percent to a high in excess of 92 percent. The highest prevalence of HCAI was located amongst the most advanced hospital facilities in South Africa and in Ghana. These studies involved facilities which experienced significant transfers-in of patients from other facilities and play pedagogic roles within their ecosystem[49].
Studies had an average sample size of 679 and a median of 300 participants, a clear indication that the data in general was skewed suggesting that medians be used cautiously in relation to the true effect of NI[15]. A significant number of studies (n=4) exclusively from West and North Africa were doctoral theses and all countries reported one study each except South Africa, Gabon and Mali which reported two studies each, see Figure 2.
Sub regional trends are easily discernible as West and Central Africa with the exclusion of the dissertations record the same proportion of studies (23 percent each). HCAI Prevalence in West Africa however is reported at double (33 percent) the ratio in Central Africa (16 percent) which is at par with South Africa’s reported pooled prevalence and is twice the pooled prevalence for North Africa (8 percent) without the student theses (n=4).
The theses are the largest subgroup within the studies under review representing 30 percent of the sample as depicted in Figure 3
They depict a more uniform prevalence between North and West Africa with a pooled prevalence of 16 percent and 14 percent respectively.
All the studies which were adjudged of high quality used either the STATA statistical software package or SPSS. One study did not report the use of any statistical package[47]. The studies adjudged to be of low quality used either EpiInfo or SPSS. The studies reported data on NI which comprised 57 percent males in line with the determinants identified by several studies which put the male gender as a significant risk factor [49, 51].
The sex ratio was therefore 1.32 with a skew towards males. Few studies involved paediatric cases (n=5) representing 38.5 percent of the studies, see Table 2.
Only one study did not provide determinants[45] see Table 1. The determinants spoke to some of the realities of the respective countries. For example, in Southern Africa, HIV was often cited among comorbidities which accounted for NI while sickle cell, clinical skill, quality of care and nutritional status where frequent markers for NI in West Africa.
In North Africa comorbidities such as diabetes and obesity as well as invasive procedures were often related to the onset of NI see Table 2.
Outcome measures such as mortality and length of stay (LOS) have often been used to estimate the economic impact of HAI [11, 33, 52]. It is unclear if this arises as a result of data paucity[15] or merely as a matter of disciplinary preference. The review did encounter a significant number of studies which took this approach and expressed economic impact solely in mortality and LOS terms (46 percent). A similar proportion expressed economic impact in monetary terms without provisioning for the cost of infection control programs (n=6). Only one study (7.6 percent – based in Fès, Morocco) was able to extract the said costs net of ICP.[15]
Routinely (n=6) costs were estimated using the following formula:
X = (H+Y+Z)x(Additional LOS)
Where:
X is the HCAI cost, H is the housekeeping, human resource and overhead costs while Y and Z represent the laboratory and diagnostic costs and the cost of antibiotic therapy respectively.
This amount is multiplied by the additional LOS days to establish the cost per episode for each individual and further multiplied by the case load to establish total HCAI costs in the facility (n=3). Of the three studies which provided cost estimates beyond episodic charges per individual, two were classified as being of high quality, had relatively large sample sizes (n=1347 & n=2172) and used the Stata (College Station, TX: StataCorp LP) statistical package while the third was adjudged to be of medium quality and used the EpiInfo software.
Figure 6 depicts the market share among selected stud�ies of the relevant statistical packages. It is worth noting that the Epi-Info software appears to be the software of choice among francophone countries and represents 46.2 percent of the studies (n=6) while STATA and SPSS together account for less than 39 percent of the studies (n=5) see Figure 6: Statistical software use.
Figure 4 denotes compliance with World Health Organisation (WHO) estimates which suggests in 2017 that 25 percent is a key threshold for HCAI prevalence in developing countries[33]. As seen in the histogram, all but 2 studies depict prevalence below 20 percent.
The studies which report HCAI prevalence beyond 20 percent acknowledge that their HCAI prevalence is unusually high because of their status as referral and teaching facilities[49]. It is also worth noting that these high prevalence numbers are skewed towards surgical interventions which are typically noted for higher NI rates [15, 50] . Median prevalence was reported at 14 percent and median sample size at 300 as reported earlier.
The studies also denote under-recovery of health expenditure within the health system in much of Sub Saharan Africa (SSA)[53]. Except for Morocco and South Africa (non SSA) the studies reflect costs that cannot be said to fully cover HCAI care costs (all are less than US$20 per episode except for Mali and Senegal [US$100-US$150]). As respondents can only report direct payments made by themselves[42], or in the case of studies which restricted expenditure data to official price schedules of the hospital facilities, subsidised health services tend to skew HCAI costs towards under-reporting[15]. Pooled mortality was generally below 10 percent except for Senegal, Gabon and Algeria. Median additional length of stay was about 10 days.
Table 2 demonstrates the predominance of enterobacteriaceae across the region with various colonies accounting for a third on average of all reported HCAI. Escherichia coli, staphylococcus aureus and klebsiella pneumoniae figure prominently across all reported studies. Twenty three percent of the studies (n=3) did not report any pathogens by name although the Centres for Diseases Control (CDC) protocols were used to identify the existence of HCAI within the health facilities which hosted the studies. Less than 10 percent of studies addressed hospital surfaces as a possible response to HCAI in the studied facilities[33].
Discussion
There is extreme paucity of data particularly on inpatient or HCAI related mortality and economic costs. Pooled or regional taxonomies in sub-Saharan Africa are even less common[13] whether for adult cases or paediatric cases. Studies usually estimate mortality and LOS as estimates of economic impact[54] and very few works exist which assign monetary value to the economic impact of HCAI. We reviewed 13 studies which expressed economic impact of HCAI in LOS terms only (n=6), in pecuniary terms (n=6) or both. The dearth of literature may point to human resource challenges within the sector particularly for skills which combine economic or financial disciplines and clinical expertise[21, 26, 55].
The studies reported average additional LOS in the Africa region at about 10 days while costs indicated significant variation due to the funding architecture of the countries concerned and the living standards therein.
Average daily costs for one additional LOS day in West Africa averaged US$10.17 while the Maghreb and South Africa average in excess of US$178. Combined at the regional level average episodic costs of HCAI amounted to US$ $773.4. This regional variability in price reflects the underlying co-morbidities (non-communicable diseases for North Africa reflecting the epidemic transition) as well as the higher level of access to care, funding, infrastructure and skill in the Maghreb and South Africa [16, 21, 23]. The average episodic costs may therefore serve as a marker for an interim funding gap for policy purposes in the West African countries which typically have more adverse outcomes and coverage which is approximately a tenth of the better performing countries in Southern and north Africa [6, 33].
The scope, nature and quality of healthcare services available in a health facility can be guessed from the prevalence of HAI within its departments. Advanced services typically would keep patients in healthcare facilities longer and therefore expose them more to nosocomial infections [7, 11]. This may be the reason for the relatively high HCAI prevalence numbers recorded in
Figure 4. Similar outcomes were noted in Ngaroua’s re�view[13] when he noted that larger facilities with more advanced equipment and ability to record and provide surveillance data for pathogens tended to report larger sample sizes in their studies and ultimately report higher HCAI prevalence figures. It can be inferred from the circumstances that better quality studies and a more competent, skilled and equipped technical team would lead to improved measurements of HCAI dynamics and better outcomes for patients.
Studies in the area typically involved median sample sizes of 300 with a sex ratio (57%) in favour of males and consistent with general hospitalisation in Ghana for example[56]. Similarly, Ngaroua [13] in a review entailing 11 studies carried out in 9 sub Saharan African countries also found a median sample size of 322 with an average greater than twice the said median. These findings may reflect the gender and geographical inequalities in access to health services particularly advanced care such as is delivered within ICU[29].
HCAI prevalence was noted to have plateaued at 16 percent on average, having risen from 12 percent on average among studies carried out more than 6 years ago. The increase in prevalence can also be attributed to the improvements in the technical range of services available to the health care facilities in Africa and to improvements in the quality of the studies themselves [13]. The prevalence reported in this group of studies lies well below the threshold prevalence (25 percent) reported by the WHO for Africa in [33]. This is not necessarily positive news as it might also reflect the scarcity of advanced health care facilities and not simply improvements in clinical practice and ICP.
Facilities in SSA though funded with a significant amount of donor resources are faced with rather intractable issues. In Mali[12] the question of shortage of hospital beds is compounded as it is in Ghana [14, 56] with concerns over the cost of ICP in surgery or in regular wards with queries over the handling of long lasting insecticide (LLIN) mosquito nets (beddings) within the context of malaria and HCAI prevention. In a resource constrained environment with 1.5 million inpatient cases per year as is the case in Ghana[56], complying with the 20-wash replacement protocol may prove difficult to manage. Very often under such circumstances, prioritising may mean making budget allocations which result in the death of some persons. It is therefore important to consider all efficiencies and work towards mitigating opportunity costs.
Tentative population based HCAI costing for Ghana using review data:
2016 – In-patient Population – 1,532,839[56] Annual growth (2.5%)[56] 2019 – In-patient estimate - 1,650,700 2019 – HCAI exposure – (14% of 1,650,700 ) = 237,701
D1 - Estimated direct costs per year:
$773.4 x 237,701= $183,837,953
Estimated indirect costs per year:
I1 - Morbidity
Minimum wage [57] x lost – man hours US$2 x 10 days x 237,701 = $4,754,020
I2 - Mortality
Minimum wage [57] x lost – TTL $2 x 22 days x 12 x 20 x 237,701 x MR = $225,754,020
Where: Lost Time to Live (TTL) represents the difference between the retirement age in Ghana (60 years) and the average age of patients denoted by the studies i.e. (40 years).
MR represents the median mortality rate denoted by the studies i.e. 9%. A working month is also assumed to be 22 days only.
A conservative estimate of HCAI costs in Ghana could therefore be reported as follows:
HCAI Costs = D1+I1+I2
HCAI Costs =$183,837,953+$4,754,020+$225,754,020
Therefore, in Ghana ICP advocacy could report the following as HCAI costs from which ICP costs could be offset in carrying out a cost benefit analysis:
HCAI Costs =$414,503,004
Unanswered Questions and Prospects for Future Work
HCAI is an increasing burden on health systems in Africa and should attract more rigorous qualitative and quantitative studies that will address costing taxonomy and other data quality issues.
NI costs in Africa are significantly lower than NI costs elsewhere in the world and costs for North and South Africa are significantly higher than costs for West and Central Africa. The costs for NI are almost 184 times higher for some advanced countries (e.g. USA [39, 58]) than it is for African countries although health investment differentials between Africa and OECD countries are generally only tenfold[32]. The differential between equatorial (SSA) Africa and its more developed parts (North/South) is about twenty-fold. There is a need to clarify the drivers of these differentials. Also, a lot less is known about the economic impact of NI in East Africa than for other regions on the continent. This signals a need to undertake work in that area particularly with respect to NI and HIV comorbid effects.
What outcomes would be achieved in terms of key variables such as incidence, prevalence and mortality of HCAI if the frequency, specificity and obsolescence of data as well as the overall quality of studies were addressed?
If greater homogeneity was achieved in study designs in the Africa region would the costing formula evolve from hospitality costs + laboratories & diagnostics + antibiotic therapy to reflect all other overheads and bureaucratic costs whether provided by public subsidy or development assistance? Would the cost differentials between regions (North/South versus West/Central) be mitigated by convergence in costing approaches within these regions?
In the matter of costs, it is not yet clear what portion of HCAI cost estimates is borne by subsidy and what portion is borne by international development assistance. Cost estimates in the selected studies often cull costs either from bills paid directly by patients and their families or rely on costing schedules provided by managers of the health facilities. Both approaches often do not provision for costs that are not reflected in the cost sheets of managers, or which were not paid for directly by the beneficiaries of the services. HCAI costs are therefore typically under cast[19]. The ambiguity in reported costs across the region is compounded by differences in quality of care which also may account for cost differentials, but which are not readily evident in the costing. Such a disparity is noticeable in the Komfo Anokye Teaching Hospital Study in Kumasi wherein significant changes to perioperative protocols led to sub regional and 30 year records in terms of declines in mortality[14]. Clearly the costs of the improved ICP are yet to be established.
What pathogens are the main cost drivers of HCAI in Africa? 23 percent of the studies (generally district and other inferior level facilities) did not reference any pathogens in their report. Ngaroua[13] noted that this trend could be attributed to the technical capacity of the health facilities concerned. Subsequent inquiries in this area could explore whether HCAI cost convergence in SSA is attributable to similarities in the disease burdens or the nature of pathogens. Further studies could also explore similarities in baseline hygienic and sanitary conditions within the health facilities and/or the community at large or analogous pricing and quality of care as explicators of HCAI cost convergence in SSA.
Improvements in technical abilities of health facilities have been noted over time and NI prevalence within facilities is also known to decline with increased knowledge and investment.
Limitations
This study is burdened by some noteworthy limitations. Selected studies are restricted by search engine access (Ajol, PubMed, Web of Science and Google Scholar). A significant number of the studies are dated, and it was unclear if the increasing NI prevalence noted over time (15 to 16 percent) was related to better metrics or greater access.
Over a third of the studies (n=4) made use of data collated 3 or more years before the publication of the paper, yet they made no attempt to inflate the reported costs to reflect contemporary costs.
Of all the studies listed only one study collected data for more than 24 months[14], there is therefore a dearth of longitudinal data that would facilitate incursions into the impact of various infection control programs which have been introduced over the years.
Additionally, over 85 percent of all studies were located in urban areas where the tertiary health care institutions and ICU are located. Finally, the economic conditions as well as the reporting standards and design of the papers was diverse and varied making attempts to standardise the summary and meta-analysis tenuous. Nonetheless, the bibliographic snowballing approach and the blend of the French and English languages significantly expanded the study sample frame, enabling the combination of countries with similar socio-economic conditions but from different linguistic blocks in a swathe which covered over 80+ percent of the continent’s geo political entities. This should provide an acceptable listing of works to stimulate the discourse on the subject within the geographies of interest.
Conclusions & Recommendations
Clearly questions of HCAI are complex and multifaceted and driven by community-based infection transmission realities. Traditionally HCAI related research has focused on the aetiology and developments in clinical care and management. There is therefore a need for greater health economic research in the area.
Inquiry into costing of HCAI is nascent and so far, indicates the potential for huge fiscal gains if well addressed. There is significant variability in costs across regions in Africa with North (Maghreb) and South Africa recording almost 20 times the costs reported in West and Central Africa. Studies estimating the economic impact of nosocomial infections should take a more holistic approach to costing in order to better capture all related expenditure. Economic impact studies for NI should also be expanded to include many more African countries particularly in East Africa.
Ghana experiences a significant economic burden of NI infections estimated at $414,503,004 in 2019. This excessive burden represents about 48 percent of the entire locally funded health budget for the year 2018[59], a figure which justifies any reasonable investments in ICP.
ICP across facilities in Africa should be enhanced and enforced while other clinical practices are optimised. In the same vein the methodology for HCAI costing studies should be standardised with emphasis on inflation and detailing clear taxonomies and expenditure classes (adult/paediatric, pathogen specific etc.) to ease comparisons over time and across countries and regions.
The quantitative mettle of studies in the area should be strengthened and greater rigour applied. A case in which a study proposes to address indirect costs yet applies itself only to direct costs is unacceptable[45].
Future research could consider costing specific pathogens as well as the use of innovative coatings and nano materials for ICP in tandem with more long-term studies and standardise key economic variables such as LOS and monetary expenditure disaggregated by cost type (direct and indirect) as well as by patient type (paediatric and adult). Such study designs would further clarify the economic impact of infection control programs within health facilities.
There is a need to implement a sentinel survey mechanism to provide up to date information on the economic impact of NI to improve policy interventions.
Finally, if Africa is to truly experience its independence, duty bearers must understand that partnerships with the research community which explore innovative cost saving approaches to health economics is a principal path to sustainable health financing and development in general.
Declarations
Availability of data and material
The datasets during and/or analysed during the current study are available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AF conceptualised the study and provided guidance on literature. DE developed the search strategy and was responsible for implementing the exclusion and inclusion criteria. AF reviewed each stage of the review for fidelity to the study protocol. All authors read and approved the final manuscript.
- Highfield R (2007) How Imhotep gave us medicine, in The Telegraph, Telegraph Media Group: London.
- Ahonen M (2017) Proactive Approach for Safe Use of Antimicrobial Coatings in Healthcare Settings: Opinion of the COST Action Network AMiCI. Int J Environ Res Public Health 2017: 14.
- Bouchnita A, AJC Jebrane, Solitons, Fractals (2020) A hybrid multi-scale model of COVID-19 transmission dynamics to assess the potential of non-pharmaceutical interventions. 2020: 109941.
- Tamayo L (2016) Copper-polymer nanocomposites: An excellent and cost-effective biocide for use on antibacterial surfaces. Materials Science and Engineering: C 69: 1391-409.
- Uwaezuoke S, H Obu (2013) Nosocomial infections in neonatal intensive care units: cost-effective control strategies in resource-limited countries. Nigerian Journal of Paediatrics 40: 125-32.
- Samuel S (2010) Nosocomial infections and the challenges of control in developing countries. African J clinical and experimental microbiology, 2010: 11.
- Yadi SN (2012) Epidémiologie des infections nosocomiales dues aux bactéries à Gram négatifs à l’unité de néonatologie de l’EHS de Tlemcen du.
- Adegboye MB (2018) Knowledge, awareness and practice of infection control by health care workers in the intensive care units of a tertiary hospital in Nigeria. Afr Health Sci 18: 72-8.
- Holmen IC (2017) Challenges to sustainability of hand hygiene at a rural hospital in Rwanda. Am J Infect Control 45: 855-9.
- Vincent JL (2003) Nosocomial infections in adult intensive-care units. Lancet 361: 2068-77.
- Dramowski AA, Whitelaw MF (2016) Cotton, Burden, spectrum, and impact of healthcare-associated infection at a South African children’s hospital. J Hosp Infect 94: 364-72.
- Togo A (2010) Fighting nosocomial infection rates in the general surgery department of the teaching hospital Gabriel Toure in Bamako, Mali. The Open Biology J 2010: 3.
- Ngaroua N (2016) Incidence des infections du site opératoire en Afrique sub-saharienne: revue systématique et méta-analyse. Pan African Medical Journal, 2016: 24.
- Oheneh-Yeboah M (2007) Postoperative complications after surgery for typhoid ileal perforation in adults in Kumasi.West Afr J Med 26: 32-6.
- Suso HS (2012) Coût de l’infection nosocomiale au CHU Hassan II de Fes (A Propos de 50 Cas), in Faculte de Medicine et de Pharmacie. 2012, Université Sidi Mohammed Ben Abdellah: Fes: 105.
- McKay R, C Bamford (2015) Community- versus healthcare-acquired bloodstream infections at Groote Schuur Hospital, Cape Town, South Africa. S Afr Med J 105: 363-9.
- Vincent JL (2009) International study of the prevalence and outcomes of infection in intensive care units. JAMA 302: 2323-9.
- Dramowski A, M Cotton, AJSAMJ Whitelaw (2017) A framework for preventing healthcare-associated infection in neonates and children in South Africa 107: 192-5.
- Ndir A (2015) Epidémiologie et impact médico-économique des infections hospitaliéres causées par les Entérobactéries productrices de beta-lactamases à spectre étendu au Sénégal, in Ecole Doctoral Pierre Louis de Santé Publique : Epidemiologie et Sciences de L’Information Biomédicale. 2015, Université Pierre et Marie Curie-Paris VI: Paris: 136.
- Mulu W (2012) Postoperative nosocomial infections and antimicrobial resistance pattern of bacteria isolates among patients admitted at Felege Hiwot Referral Hospital, Bahirdar, Ethiopia. Ethiopian journal of health sciences 22: 7-18.
- Kaddar M (1995) Financement et dynamique des systèmes de santé au Maghreb: données et problèmes actuels. MOM Éditions 1: 185-98.
- Ouma PN, AN Masai, IN Nyadera (2020) Health coverage and what Kenya can learn from the COVID-19 pandemic. J Global Health 2020: 10.
- Mrabet M, Systeme de Sante Marocain, in Systeme de Sante Marocain Seminar- (Lesson Notes). 2017, Universite Mohammed V de Rabat: Universite Mohammed V de Rabat.
- Annan K (2001) Wealthy nations called on to boost support efforts. Five-year plan estimated to cost $9.2 billion. AIDS Alert 16: 99-101.
- Wang H, N Otoo, L Dsane-Selby (2017) Ghana National Health Insurance Scheme, Washington, DC: World Bank.
- Boakye A, O Babatunde Olumide (2021) The role of internet of things to support health services in rural communities. A case study of Ghana and Sierra Leone. Transnational Corporations Review 13: 43-50.
- GHS (2018) Ghana Health Facts and Figures 2018. Ghana Health Service: Accra: 79.
- Wang Y (2021) Sociodemographic Inequalities in Health Insurance Ownership among Women in Selected Francophone Countries in Sub-Saharan Africa. BioMed Research International, 2021.
- Organisation of African Unity. Abuja Declaration on HIV/AIDS, Tuberculosis and Other Related Infectious Diseases. in Africa Summit on HIV/AIDS, Tuberculosis and Other Related Infectious Diseases. 2001. Abuja: Organisation of African Unity.
- Sadr-Azodi N (2001) Following the 2001 Abuja Declaration of committing 15 percent government expenditure on health, is Africa making progress towards universal health coverage?.
- Afle FCD () État des lieux des infections associées aux soins dans deux hôpitaux publics du sud Benin (Afrique de l’ouest) : Centre Hospitalier Universitaire de Zone d’Abomey- Calavi/Sô-Ava et Centre Hospitalier de Zone de Cotonou 5. Journal of Applied Biosciences, 2018: 121.
- Booth ON (1968) Isolated burn unit prevents contamination. Hospitals 42: 50-1.
- Sperry HE, J Craddock (1968) It pays to spend money for infection control. Mod Hosp 111: 124-8.
- Starkweather D (1968) A pricing policy for isolation care. Hosp Top 46: 29-30.
- Roberts RB (1969) Disposable anesthetic circuit. JAMA 207: 2285.
- Weinzettel RJ (1968) Infection-control program reduces hospital stay, costs. Hosp Top 46: 53-6.
- Dixon RE (1978) Effect of infections on hospital care. Ann Intern Med 89: 749-53.
- Official Data Foundation. Hospital and related services priced at $20 in 2000 → $55.37 in 2019.
- Zhang S (2016) Cost of hospital management of Clostridium difficile infection in United States-a meta-analysis and modelling study. BMC Infect Dis 16: 447.
- Samou FHS (2005) Les Infections Nosocomiale dans le service de chirurgie B de l’Hopital du Point G, in Faculté de Médecine, de Pharmacie et d’Odonto-Stomatologie. 2005, Université du Mali: Bamako: 106.
- Cooper BS (2003) Systematic review of isolation policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literature with epidemiological and economic modelling. Health Technol Assess 7: 1-194.
- Zhang YZ, S Singh (2015) Antibiotic stewardship programmes in intensive care units: Why, how, and where are they leading us. World J Crit Care Med 4: 13-28.
- Bukasa JC (2018) Consequences of nosocomial infections in maternity in the city of Mbujimayi/DR Congo. Environmental and Water Sciences, public Health and Territorial Intelligence J 2: 18-23.
- Kuissi Kamgaing E (2017) Colonisation digestive par des germes nosocomiaux des nouveau-nés hospitalisés au CHU d’Angondjé : aspects épidémiologiques et facteurs de risque. Journal de Pédiatrie et de Puériculture 30: 193-200.
- Tchoua R (1999) Gravité des maladies de réanimation à la fondation Jeanne Ebori de Libreville. Médecine d’Afrique Noire 46: 496-9.
- Ndir A (2016) Epidemiology and Burden of Bloodstream Infections Caused by Extended-Spectrum Beta-Lactamase Producing Enterobacteriaceae in a Pediatric Hospital in Senegal. PLoS One 11: e0143729.
- Fourie T (2018) Antibiotic prescribing practices in the presence of extended-spectrum β-lactamase (ESBL) positive organisms in an adult intensive care unit in South Africa – A pilot study. Alexandria Journal of Medicine 54: 541-7.
- Bouafia N (2013) Magnitude and impact of serious adverse events related to treatment: study of incidence in a hospital in East Central Tunisia. Pan Afr Med J 16: 68.
- Zilberberg MD (2017) Carbapenem resistance, inappropriate empiric treatment and outcomes among patients hospitalized with Enterobacteriaceae urinary tract infection, pneumonia and sepsis. BMC Infect Dis, 17: 279.
- Gillespie BM (2017) Economic case for intraoperative interventions to prevent surgical-site infection. Br J Surg 104: e55-e64.
- Adu-Gyamfi M (2017) National AIDS Spending Assessment 2015-2016, Level and Flow of Resources and Expenditures to Confront HIV and AIDS. 2017, Ghana AIDS Commission: Accra: 74.
- Dramowski A (2017) Cotton, and A. Whitelaw, A framework for preventing healthcare-associated infection in neonates and children in South Africa. S Afr Med J 107: 192-5.
- Aiken AM (2012) Interventional studies for preventing surgical site infections in sub-Saharan Africa - A systematic review. Int J Surg 10: 242-9.
- GHS (2016) Annual Report. 2017, Ghana Health Service:Accra: 129.
- Rosen J, F Asante (2010) Cost of HIV & AIDS Adult and Pediatric Clinical Care and Treatment in Ghana. 2010: Washington, DC.
- Dixon RE (1985) Economic costs of respiratory tract infections in the United States. Am J Med 78: 45-51.
- Ministry of Health, Annual Financial Report - 2018. 2020, Ministry of Health - Republic of Ghana.
GSS (2018) GHS, and DHSP-ICFI, Ghana demographic and health survey, 2014 - Key Indicators. 2015, Accra: Ghana Statistical Service.
Govender V, D McIntyre, R Loewenson (2008) Progress towards the Abuja target for government spending on health care in East and Southern Africa. EQUINET Discussion Paper Series 57. EQUINET: Harare.
FIGURE 1
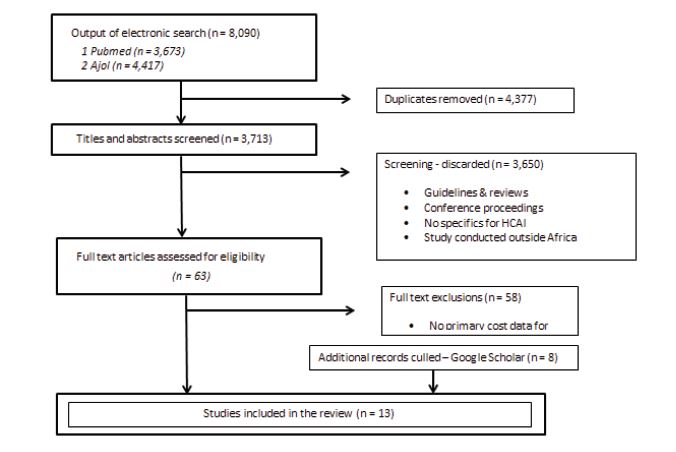
Figure 1: Study Selection Procedure
FIGURE 2
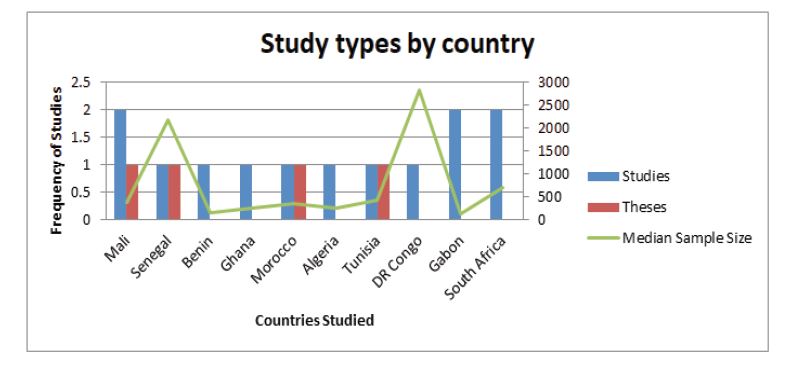
Figure 2: Study types & sample sizes across countries
FIGURE 3
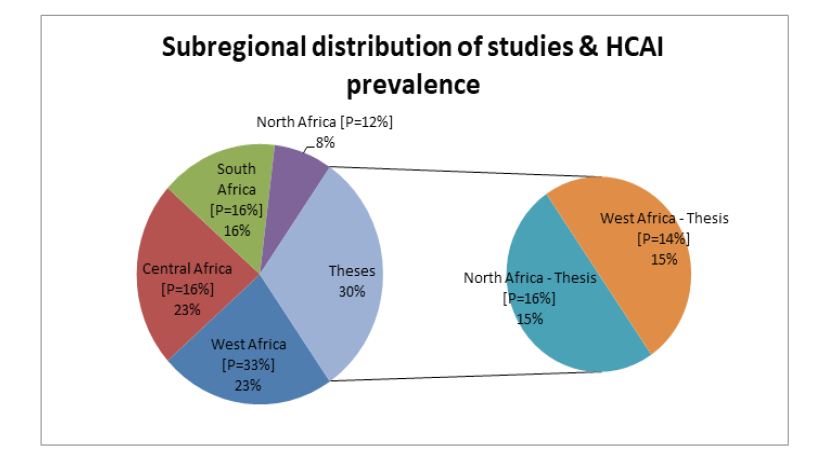
Figure 3: Sub regional distribution of studies & prevalence [P]
FIGURE 4
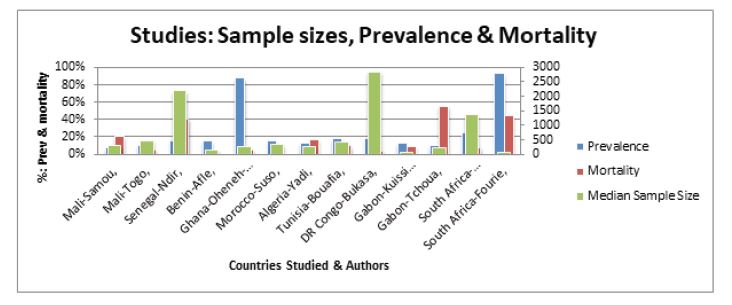
Figure 4: Prevalence & Mortality
FIGURE 5
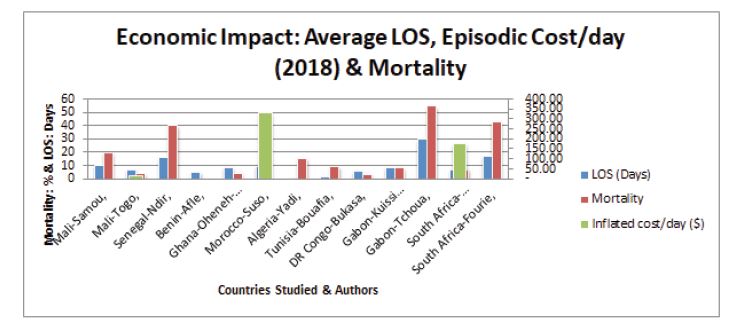
Figure 5: Economic Impact - Average LOS, Mortality & Daily Cost
FIGURE 6
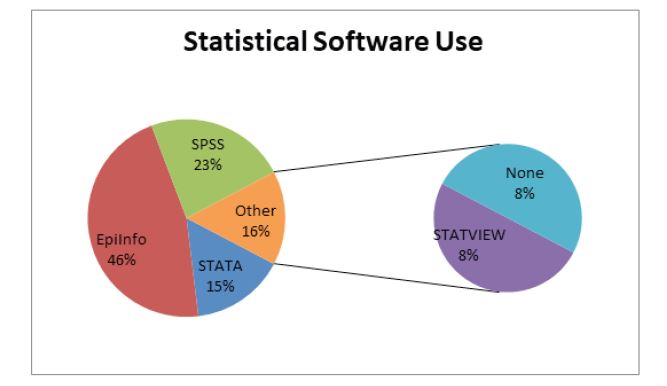
Figure 6: Statistical software use
Tables at a glance
Figures at a glance