Families and Care in the Intensive Care Unit
Received Date: August 03, 2024 Accepted Date: September 03, 2024 Published Date: September 06, 2024
doi: 10.17303/ijnsp.2024.3.101
Citation: Thiago Gomes Romano, Guilherme Bittar Cunha, Fernanda Aparecida Franco, Valdinéia Rocha Costa dos Santos (2024) Families and Care in the Intensive Care Unit. Int J Nur Man Pat Car 3: 1-10
Abstract
The provision of family-centered care in the intensive care unit (ICU) is crucial for both patients and their loved ones. In this review manuscript, we underscore the significance of family care in the ICU setting and present a comprehensive analysis of the existing literature on this topic.
We highlight the vital role of families in the care of ICU patients and emphasize the positive impact of family involvement on patient outcomes and overall satisfaction with care.
Furthermore, we propose a systematic approach to family care during ICU daily routines, with a specific focus on the ABRACOS protocol.
The ABRACOS protocol emphasizes fostering a collaborative relationship between healthcare providers and families, promoting open communication, and providing support and education to family members.
Through our review of the literature and the proposed systematic approach, we aim to encourage the implementation of structured family care practices in the ICU setting, ultimately enhancing the overall well-being of patients and their families.
Keywords: Intensive Care Unit; Patients; ABRACOS Protocol; Healthcare Providers; Family Care Practices
Introduction
The technical side of medicine has undeniably advanced in recent years, and we have reached the 21st century with the possibility of removing tumors through robotic surgery, prolonging life with mechanical ventilation and hemodialysis, and reducing maternal and infant mortality. The current development agenda was unthinkable decades ago, but the essence of medical practice remains, as it has always been, a relationship of trust between human beings, with decision-making processes that concern not only the disease itself but also ethical, religious and philosophical dimensions [1].
Understanding how each of these dimensions impacts each individual patient is the core of so-called patient-- centered care and the first step toward ethical decisions and the establishment of care goals on the basis of beneficence, nonmaleficence, justice and autonomy.
The term patient-centered care was first used in 1988 by Picker et al. in the Commonwealth Program for Patient-Centered Care in the United States of America and is defined according to the following aspects (Figure1):
1. Respect for the values, preferences and needs expressed by the patient,
2. Coordinated and integrated care,
3. Quality care
4. Clear and quality information,
5. Family patient education,
6. Physical comfort (including pain control, emotional support and alleviation of fear and anxiety),
7. Involvement of family and friends, and
8. Continuity, with appropriate transition of care.
Subsequently, the Institute of Medicine (IOM) included patient-centered care as a quality practice of the American health system, defining it as “care that is respectful of and responsive to the preferences, needs and values of the patient, such that clinical decisions are guided by patient values”. Intrinsic to this definition is the need for patients and health professionals to work together.
Patient-centered care and the decision-making process
In some situations, there is one clear, scientifically well-defined path regarding treatment; for example, bacterial meningitis requires antimicrobials, and a hip fracture requires surgical correction [2]. However, most clinical cases entail more than one plausible decision, including the decision not to intervene. In these cases, patient involvement can impact the decision-making process.
In this process, both parties share information: the physician presents the options and potential impacts of each choice, and the patient/family expresses their values and preferences. Several tools proposed in the literature can facilitate this process.
Although the above makes sense, transforming these theoretical points into practice is a challenging process,and it includes a cultural change exemplified by the change from the question of “What is your problem?” to “What impact does your problem have on you?”.
One of the most interesting articles we reviewed was the publication by Bokhour et al. [3], who studied how American veterans’ hospitals worked. They observed that the shift from a model centered on disease and health care provision to care centered on patients involved 7 domains of practical action (Figure 2):
1. Leadership involvement,
2. Engagement of patients and family,
3. Staff engagement,
4. Innovations related to patient-centered care, here citing a committee of patient-centered care or experience
5. Focus on the concept within the organizational structure and processes, breaking the idea of working in silos and developing an integrated approach between areas,
6. Involvement in specific points of care,
7. Dissemination of experiences lived in the hospital in relation to the subject.
In summary, the authors state that patient-centered care does not concern only the clinical level but should involve all spheres and levels of contact with the patient, starting with the top leadership of the organization.
Considering the above, we believe that the work routine of an intensive care unit should contain points that meet the need for patient-centered care. When such processes are part of the daily routine of the multiprofessional team, the inclusion of the concept becomes natural.
One aspect, within the concept of care centered on the patient and their family, is the so-called patient-reported outcomes (PRO), defined as the ability of the patient himself to describe his health status and expected outcome.
Within this aspect (PRO) some quantitative data can be brought into discussion. Austin et al, at the University of Washington, evaluated 14 PRO implementation models and found that only 47% of them captured clinical data in common between them (such as depression), demonstrating that there is still a long way to go in standardizing the model [4].
Although data on PRO are well studied in specialties such as plastic surgery [5] dentistry [6], endocrinology [7] and neuro-ophthalmology [8], little is commented on intensive care setting. A very interesting proposal, in our opinion, was brought by Granholm et al, that the traditional outcome of randomized controlled studies in the ICU, mortality, is replaced by patient-focused outcomes such as support-free days, functional outcomes and quality of life, the authors included 687 outcomes of 167 studies, only 32% of them with important patient outcomes other than mortality, of the “non-mortality” outcomes the most common were cognitive functionality (62%) and quality of life (89%) [9].
Patient-centered care in the routine of an intensive care unit
In the process of admitting a patient to the intensive care unit, two feelings are commonly present: fear and anxiety
In an aviation analogy, when passengers board an aircraft, moments before takeoff, they are subjected to a routine of guidance on flight procedures, including the usual steps as well as how to proceed in case of a flight emergency.
While the hospital environment shares many features with aviation, such as the need for strict safety protocols, anxiety about the unusual situation and team multitasking, patient briefing is not so well structured. Therefore, we developed a mnemonic rule to guide patients admitted to the ICU, the so-called ABRACOS (hugs) protocol (Figure 3), in which we outline the unit’s routine using each letter of the mnemonic:
Alarms (Alarmes): Here, we explain that the patient will be monitored and that, eventually, alarms will sound, and the team will be attentive to them. The alarms of drug infusion pumps and the importance of not changing their parameters is also highlighted at this point.
Good practice (Boas práticas): The companion/- family is invited to be the protagonist for the patient’s safety, a barrier for every health professional who examines, medicates or even enters the patient’s room to wash their hands.
Routine (Rotinas): We indicate the times of feeding, exams and multiprofessional visits.
Companions (Acompanhantes): Companions are instructed about the unit’s visitation policy.
Care (Cuidado): The importance of a multiprofessional approach in the ICU is explained to the patient, who will be cared for by a team composed of physicians, nurses, physical therapists, clinical pharmacists, speech therapists, psychologists, nutritionists and, eventually, any other specialist that may be appropriate according to the patient’s needs.
Listening (Ouvir): Here, we express openness to questions or doubts.
Emergency situations (Situações de emergência): We explain that although we have a policy promoting monitoring by family members, with the possibility of a 24-hour stay, there may be situations of emergency care when they are invited not to be present. This item is included in a consent form upon admission to the ICU, along with items and procedures that may be necessary throughout the patient’s care in the unit.
Notably, sometimes, upon patient admission, there is such anxiety, fear and expectation of care that clear communication is difficult, and selective listening can occur. In such cases, the ABRACOS protocol may be given the day following admission but still within the patient’s first 24 hours in the unit.
Family presence in the ICU as a tool for patient-centered care
The relationship between hospitals and families has been ongoing for the last 200 years. Historically, hospitals made their access policies more restrictive at the end of the 19th century, considering that companions could become a means for the transmission of infectious diseases and potentially introduce prohibited items into the hospital [10,11]. The cultural change toward more permissive policies fostered a scientific research agenda on the subject.
Rosa et al. evaluated the impact of so-called extended visits (up to 12 hours a day) compared with traditional visits (up to 4.5 hours a day). The findings did not demonstrate an impact on the primary outcome, which was the reduction in acute mental confusion, a situation described as delirium, but a reduction in anxiety and depression was observed in families who were able to spend more time with their loved ones during hospitalization in the intensive care environment [12].
The unrestricted presence of the family in the intensive care unit was also studied by Bailey et al. from the point of view of health professionals. Through a questionnaire answered by 1,255 professionals, 74% of whom were nurses working in units with an average daily family visit time of 20 hours (ranging from 10 to 24 hours a day), the authors reported that the professionals perceived great benefits of unrestricted visits to family members but expressed concerns regarding the potential for burnout, occupational violence and the workload for health professionals [13].
For the successful inclusion of the family as part of the patient-centered care strategy, one point is essential: the way we communicate, especially in the establishment of care goals and mutual respect.
Curtis et al. demonstrated that a strategy aimed at improving communication between the ICU team and the family reduced the length of stay both in the ICU and in the hospital, as well as hospitalization-related costs [14].
The NICU environment is a fertile ground for learning about family-centered care and communication, concepts that impact preterm infant weight gain, length of hospital stay, reduction in maternal stress and even minor structural changes in infant brains, as demonstrated by magnetic resonance imaging [15-17], in addition to better preparation for the care of vulnerable patients after hospital discharge.
The practical application of this concept involves family participation in multidisciplinary ICU visits, skin-- to-skin contact with the baby, engagement in care safety issues, and a welcoming culture with a written information leaflet accompanied by a debriefing explaining hand hygiene, equipment, the role of ICU staff, companion policy and other aspects of care in the unit.
Through the observation of this good practice in the neonatology scenario, we brought the routine of the multiprofessional visit with the presence of the family into the scenario of the adult patient. The family/loved ones are informed, through the ABRACOS protocol, that routinely at 17:00, they will be invited to join the multidisciplinary team for discussion of the case. The phrase “We will discuss the case of your family member; there will be various technical terms, but in the end, we will summarize the next steps in care” is used the first time they are invited to participate.
We believe that, in addition to being a technical routine, the moment when we check the achievement of the established care goals in the morning also represents a routine that establishes a bond of trust between the intensive care unit team and the family.
The COVID-19 pandemic was a recent experience revealing the impact of limiting the presence of the family in the environment and in the ICU, and visiting restrictions negatively impacted the well-being of both patients with COVID-19 and those without COVID-19 [18]. An example of the impact was the difficulty in mourning due to the impossibility of saying goodbye to loved ones at the end of life [19].
Despite all the theories described above, nothing is put into practice if there is not a relationship between patients/families and health care providers, including health institutions. In an article published in 2017, Dugdale provides an interesting perspective of how relationships become more pleasurable for both sides when there is a relationship of “exchange” of experiences and perspectives of care [20].
In this context, a question is imperative: what are the determinants of a bond of trust?
Although we instinctively know what the feeling of trust means, there is no single definition. Two are presented here:
1. Trust is the expectation that the other person will behave with good intentions, keep his promises and avoid doing evil, implying the ability to delegate something valuable to the other person.
2. Trust is the willingness we have to make ourselves vulnerable to someone, on the basis of the expectation that the other will act according to our expectations regardless of whether we can control or monitor their actions.
There are initiatives to measure trust, both interpersonal and institutional, such as the Australian General Social Survey (AGSS), the Canadian General Social Survey (CGSS), the European Social Survey (ESS) and the Gallup World Poll, and they consider the sphere of diverse subjects, such as sociology, political sciences, psychology and economics. Interestingly, the degree of confidence is correlated with well-being, per capita income and quality of life.
Note that, regardless of the definition used, the word expectation is present, such that there is a link between trust and expectation. Thus, the establishment of trust entails the alignment of expectations of care, although there are intrinsic factors of the person that have a strong impact on the patient’s confidence in his doctor, vulnerability [21] and mental health situation [22], and patients may be from groups that have historically been discriminated against as minorities [23].
However, what interpersonal characteristics lead people to trust each other?
Zanger and Folkman, in a publication in the Harvard Business Review, analyzed 87,000 people/leaders and identified 3 points:
1. Quality of relationships. The ability we have to recognize important points in others, cooperate and give honest feedback,
2. Judgment. The technical capacity and expertise of the person in a given subject.
3. Consistency. In English, this is called “walk their talk”, that is, whether the person acts according to their speech, honoring their commitments.
A concept that goes hand in hand with that of patient-centered care is the “culture of transparency”. Easy access to information is another beneficial point in this discussion, as it supports a greater ability to engage in the decision-making process [24], a greater degree of trust in the doctor [25] and an understanding of the care plan [26].
In this discussion, cultural aspects must also be put into perspective. Alshammari et al, through a qualitative study demonstrated that the nationality of the nursing staff influenced the perception of quality of communication, aspects of respectful and non-verbal communication, regardless of the barrier language, religious or work overload [27].
Danjoux et al published the experience of a Canadian center in Ontario in a workshop with its collaborators, raising cultural barriers experienced in everyday routine, of which both cultural and religious aspects stand out [28]. Despite the cultural heterogenicity that may exist within an intensive care environment, some initiatives such as that of Brooks et al, in Australian centers with a cohort of patients in the process of death, demonstrated that looking at each family member is viable, 224 patients (52%) were of another nationality, 64 (14.9%) spoke a language other than English, 216 (50.2%) were christians, 8 (1.9%) muslims and 13 (3%) buddhists, this personalized approach was possible through multidisciplinary help with leaders local clergy, translators and social workers [29].
What do we believe?
In this book, the reader can come into contact with various experiences that illustrate patient-centered care. However, such care is focused not only on these experiences but also on the daily role of the patient in his or her care. The successful application of such a concept requires a vision not only of the professionals who perform the care but also of the institution that supports them.
To us, it is reasonable to work to continually improve communication and mutual respect and to design processes and routines of the units that provide moments supportive of the application of this concept.
- Maldonado F, Medicine CEBftSoHiC (2020) The Humanities in Chest Medicine and CHEST: The Case for a Holistic, Patient-Centered Approach to Delivering Pulmonary, Critical Care, and Sleep Medicine in the Twenty-First Century. Chest. 158: 3-4.
- Barry MJ, Edgman-Levitan S (2012) Shared decision making--pinnacle of patient-centered care. N Engl J Med. 366: 780-1.
- Bokhour BG, Fix GM, Mueller NM, Barker AM, Lavela SL, Hill JN, et al. (2018) How can healthcare organizations implement patient-centered care? Examining a large-scale cultural transformation. BMC Health Serv Res. 18: 168.
- Austin E, LeRouge C, Hartzler AL, Segal C, Lavallee DC (2020) Capturing the patient voice: implementing patient-reported outcomes across the health system. Qual Life Res. 29: 347-55.
- Talwar AA, Niu EF, Broach RB, Nelson JA, Fischer JP (2023) Patient-reported outcomes: A primer for plastic surgeons. J Plast Reconstr Aesthet Surg. 86: 35-47.
- Hua F (2024) Dental Patient-Reported Outcomes Update 2023. J Evid Based Dent Pract. 24: 101968.
- Geer EB (2022) Patient-Reported Outcomes in Endocrinology. Endocrinol Metab Clin North Am. 51: 15-6.
- De Lott LB, Ehrlich JR (2021) Patient-Reported Outcomes Research in Neuro-Ophthalmology. J Neuroophthalmol. 41: 141-6.
- Granholm A, Anthon CT, Kjaer MN, Maagaard M, Kaas-Hansen BS, Sivapalan P, et al. (2022) Patient-Important Outcomes Other Than Mortality in Contemporary ICU Trials: A Scoping Review. Crit Care Med. 50: e759-71.
- Mooney G, Reinarz J (2009) Hospital and asylum visiting in historical perspective: themes and issues. Clio Med. 86: 7-30.
- Berwick DM, Kotagal M (2004) Restricted visiting hours in ICUs: time to change. JAMA. 292: 736-7.
- Rosa RG, Falavigna M, da Silva DB, Sganzerla D, Santos MMS, Kochhann R, et al. (2019) Effect of Flexible Family Visitation on Delirium Among Patients in the Intensive Care Unit: The ICU Visits Randomized Clinical Trial. JAMA. 322: 216-28.
- Bailey RL, Ramanan M, Litton E, Yan Kai NS, Coyer FM, Garrouste-Orgeas M, et al. (2022) Staff perceptions of family access and visitation policies in Australian and New Zealand intensive care units: The WELCOME-ICU survey. Aust Crit Care. 35: 383-90.
- Curtis JR, Treece PD, Nielsen EL, Gold J, Ciechanowski PS, Shannon SE, et al. (2016) Randomized Trial of Communication Facilitators to Reduce Family Distress and Intensity of End-of-Life Care. Am J Respir Crit Care Med. 193: 154-62.
- O'Brien K, Bracht M, Macdonell K, McBride T, Robson K, O'Leary L, et al. (2013) A pilot cohort analytic study of Family Integrated Care in a Canadian neonatal intensive care unit. BMC Pregnancy Childbirth. 13: S12.
- Smith GC, Gutovich J, Smyser C, Pineda R, Newnham C, Tjoeng TH, et al. (2011) Neonatal intensive care unit stress is associated with brain development in preterm infants. Ann Neurol. 70: 541-9.
- White-Traut RC, Rankin KM, Yoder JC, Liu L, Vasa R, Geraldo V, et al. (2015) Influence of H-HOPE intervention for premature infants on growth, feeding progression and length of stay during initial hospitalization. J Perinatol. 35: 636-41.
- Hugelius K, Harada N, Marutani M (2021) Consequences of visiting restrictions during the COVID-19 pandemic: An integrative review. Int J Nurs Stud. 121:104000.
- Kentish-Barnes N, Cohen-Solal Z, Morin L, Souppart V, Pochard F, Azoulay E (2021) Lived Experiences of Family Members of Patients With Severe COVID-19 Who Died in Intensive Care Units in France. JAMA Netw Open. 4: e2113355.
- Dugdale LS (2017) Re-Enchanting Medicine. JAMA Intern Med. 177:1075-6.
- Plomp HN, Ballast N (2010) Trust and vulnerability in doctor-patient relations in occupational health. Occup Med (Lond). 60: 261-9.
- Chanfreau-Coffinier C, Gordon HS, Schweizer CA, Bean-Mayberry BA, Darling JE, Canelo I, et al. (2018) Mental Health Screening Results Associated with Women Veterans' Ratings of Provider Communication, Trust, and Care Quality. Womens Health Issues. 28: 430-8.
- Saarinen AO, Rasanen P, Kouvo A (2016) Two dimensions of trust in physicians in OECD-countries. Int J Health Care Qual Assur. 29: 48-61.
- DesRoches CM, Delbanco T, Bell SK (2019) Patients Managing Medications and Reading Their Visit Notes. Ann Intern Med. 171: 774.
- Gerard M, Chimowitz H, Fossa A, Bourgeois F, Fernandez L, Bell SK (2018) The Importance of Visit Notes on Patient Portals for Engaging Less Educated or Nonwhite Patients: Survey Study. J Med Internet Res. 20: e191.
- Delbanco T, Walker J, Bell SK, Darer JD, Elmore JG, Farag N, et al. (2012) Inviting patients to read their doctors' notes: a quasi-experimental study and a look ahead. Ann Intern Med. 157: 461-70.
- Alshammari M, Duff J, Guilhermino M (2022) Adult patient communication experiences with nurses in cancer care settings: a qualitative study. BMC Nurs. 21: 201.
- Danjoux N, Hawryluck L, Lawless B (2007) Cultural and religious aspects of care in the intensive care unit within the context of patient-centred care. Healthc Q. 10: 42-50.
- Brooks LA, Manias E, Bloomer MJ (2022) How do intensive care clinicians ensure culturally sensitive care for family members at the end of life? A retrospective descriptive study. Intensive Crit Care Nurs. 73: 103303.
FIGURE 1
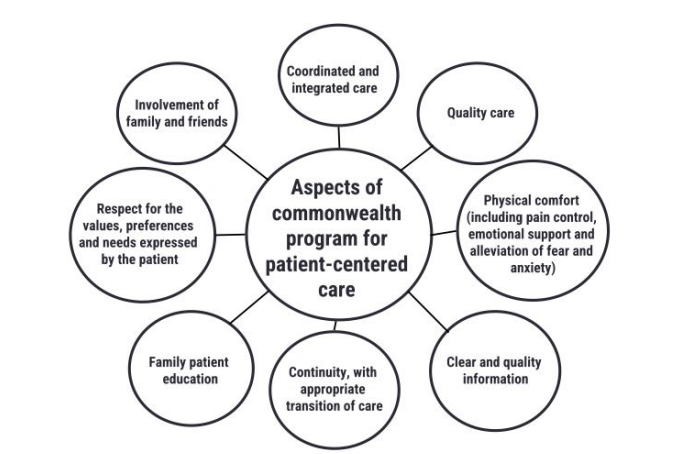
Figure 1: Aspects of patient centered care
FIGURE 2
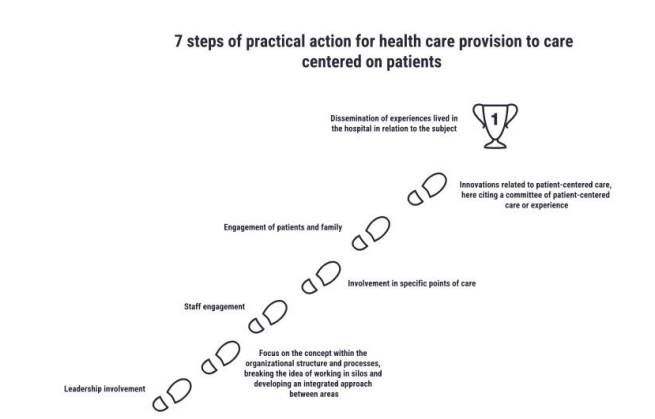
Figure 2: Seven practical actions towards a patient centered care model
FIGURE 3
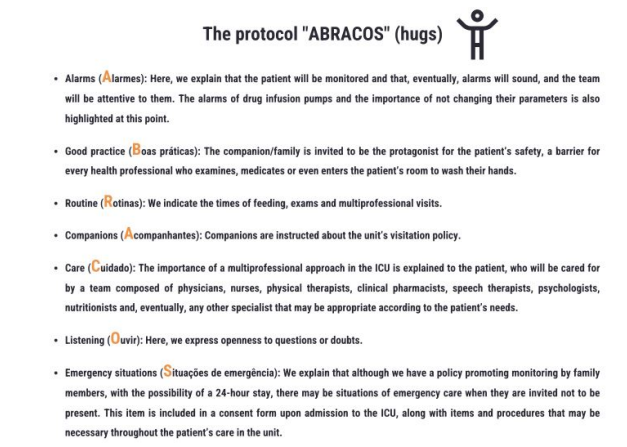
Figure 3: The protocol "ABRACOS"
Figures at a glance