Characterization of Staphylococcus Aureus Carriage Among Asymptomatic Individuals in the Republic of Congo
Received Date: August 11, 2025 Accepted Date: August 26, 2025 Published Date: August 30, 2025
doi:10.17303/jaaa.2025.2.102
Citation: Claujens Chastel Mfoutou Mapanguy, Jealvie Narcia Limingui, Frieder Schaumburg, Linzy Elton, Euphra Dareine Bitoumbou, et al. (2025) Characterization of Staphylococcus Aureus Carriage Among Asymptomatic Individuals in the Republic of Congo. J Antibiot Antimicrob Agents 2: 1-12
Abstract
Purpose:Staphylococcus aureus is a significant contributor to bacterial-related mortality globally, often stemming from pre-existing asymptomatic colonization, including strains resistant to antibiotics. Despite its importance, data on S. aureus colonization and asymptomatic carriage remains limited in some African region. Here, we conducted a cross-sectional study to assess S. aureus carriage among healthy adults in the Republic of Congo, while also investigating molecular markers of antimicrobial resistance.
Methods:Methods: Healthy adult volunteers residing in Brazzaville were recruited at the Centre de Recherche sur les Maladies Infectieuses Christophe Mérieux (CeRMI-CM) of the Fondation Congolaise pour la Recherche Médicale (FCRM). After informed consent, nasal and oropharyngeal swabs were collected and prcnessed using standard microbiological procedures to isolate S. aureus. Antimicrobial susceptibility testing was carried out by disc diffusion, with confirmation of Methicillin resistance and Panton-Valentine Leukocidin (PVL) by PCR.
Results:Among 175 adults examined, 39 (22%) were colonized with S. aureus. Of these, 29/39 (74%) were nasal carriers, 6/39 (15%) were oropharyngeal carriers and 4/39 (10%) were dual carriers. Methicillin-resistant S. aureus (MRSA) was detected in 4/39 (10%) of asymptomatic individuals. Among all isolates, 9/39 (23%) were positive for PVL (2 MRSA, 7 methicillin-susceptible S. aureus [MSSA]). Resistance to other antibiotics was prevalent among MSSA strains, notably Azithromycin and Erythromycin resistance rates of 21% each.
Conclusion: Our study reveals a 22% prevalence of S. aureus colonization among healthy Congolese adults in an urban community. Moreover, the presence of multi-antibiotic resistant strains underscores the need for further investigation into nationwide prevalence, decolonization strategies, and their implications for the management of hospitalized patients.
Keywords: Bacteria, Staphylococcus Aureus; Carriage; Commensal; Pathogen; Republic of Congo; Central Africa
Introduction
Globally, Staphylococcus aureus is one of the leading causes of bacterial infections related mortality [1], S au. reus is also an important pathogen identified in nosocomial infections caused by Gram-positive bacteria [2]. *Ihe recent increase in the incidence and severity of Staphylococcal in- fections has revived interest in studies the burden of asymptomatic carriage of S aureus in different communi- ties [3]. This bacterial species is ranked first or second among bacterial pathogens responsible for in- fections, pneumonia and complicated skin and soft tissue in. fections [4,5]. These infections commonly arise from pre-ex- isting asymptomatic colonization. The known sites of S. au- reus colonization are the nostrils, mouth, skin, and gastroin- testinal tract [6-8]. It is estimated that up to 30% of the hu- man population is colonized by S aureus, including 50% of adults presenting persistent or intermittent carriage [9,10], Given the risk of progression from colonisation to infec- tion, decolonization or eradication of carriage prior to an in. tervention is common in clinical practice for prevention of S. aureus related sepsis.
Importantly, several circulating strains of S aureus have developed resistance to commonly used antimicro- bials, a phenomenon closely linked to their inappropriate us. age [2]. Managing infections caused by resistant S. aureus therefore remains a major challenge for healthcare systems [11]. Severe skin and soft tissue infection, the most com. mon expression of S. aureus infection in the community setting, is strongly associated with the Panton Valentine Leukocidin (PVL), a virulence factor independent of methi- cillin resistance: both methicillin-resistant and methi- cillin-sensitive strains of Staphylococcus aureus [MRSA and MSSAI can produce PVL [12,131. To identify the reservoir of S aureus infection in the general population, epidemio- logical investigations involving asymptomatic carriers of S. aureus are of interest. Indeed, colonization has been shown to a reservoir for pathogenic strains and/or a pre infectious stage [3] as well as the starting point for the development of nosocomial infections by drug-resistant pathogens, a major cause of mortality worldwide [14].
Across Africa, the data on S. aureus colonisation remains scarce. In the Republic of Congo reports from hos- pital Settings on S. aureus infections are limited, with preva- lences ranging from 28% to 80% [ 15,161. So far, no investiga- tion in the community has been reported. primary ob- jective of this study was to determine S. aureus carriage among healthy Congolese adults, with a secondary aim to characterize molecular markers of antimicrobial resistance.
Materials and Methods
Study PopulationThis cross-sectional study was conducted from 1st March to 31st July 2022 in Brazzaville, the capital of the Re- public of Congo. Participants were recruited from all three areas of Brazzaville, which include the nine districts of the city. area 1 in south (Makélékélé, Bacongo, Madibou); area 2 in the center (Poto-Poto, Moungali and Mfilou) and area 3 in the north (Ouenzé, Talangai and Djiri) as shown in fig- ure l. As of 2023, the estimated population of the Republic of the Congo was 6,142,180 inhabitants, with the majority residing in urban areas such as Brazzaville, a densely populated city which hosts one-third of the Congolese population [17]. Recruitment efforts included widespread distribution Of flyers across Brazzaville, targeting locations such as universities, schools, civil society associations and NGOs. Participation was voluntary, and inclusion criteria required participants to at least 18 years old. Pregnant women, individuals known to be HIV seropositive, and those with compromised immune systems were excluded from the study.
Patient Recruitment and Sample CollectionEligible participants were recruited by trained personnel. Clinical (date of previous hospitalization, use of antibiotics, history of skin and/or soft tissue infection, smoking, use of hormone contraception for women, socio-demographic data (age, sex, residence, number of household members, contact with animals) were recorded at enrolment. While the nasal samples were collected by swabbing both nostrils of everyone with a sterile cotton swab, the oropharyngeal swab was collected from the same participant by dabbing the larynx behind the tongue. Each swabwas preserved in Stuart Amie transport solid medium (Oxoid, Brescia Italy: 202485200) and transferred immediately to the microbiology laboratory at room temperature (28°C).
Bacterial Culture and Identification of S. Aureus StrainsConventional bacterial culture was performed within 2 hours of the laboratory receiving the swab. Swabs were inoculated onto sheep Columbia blood agar (CM0331B, Oxoid™, Germany) prepared 24 hours in advance bv followin the manufacturer's instructions. The inoculation onto sheep blood agar of both swabs collected from each participant were cultured on two separate plates and incubated at 370C for 18 to 24 hours. S. aureus was identified on the basis of the colony morphology followed by catalase and coagulase activity by a Staphytect Plus latex lutination test (Oxoid) or by rabbit plasma agglutination in tubes (Becton Dickinson & Co. Lane Santa Maria, Canada) when the Staphytect agglutination test provided ambiguous results.
Antimicrobial Susceptibility TestingAntimicrobial susceptibility testing was performed using the disc diffusion method according to Clinical Labo- ratory Standards Institute (CLSI) guidelines (18), Briefly, colonies of pure bacterial strains were suspended in sterile normal saline with a McFarland standard turbidity equiva- lent to 0.5, and streaked evenly onto Muller Hinton Agar (MHA, Oxoid, Strasbourg-France) plates. After allowing the plates to dry, the following antibiotic discs were placed onto the plate Cefoxitin (30 gg), Azithromycin (15 gg), Ery- thromycin (15 pg), Tigecycline (30 gg), Linezolid (30 pg) and Vancomycin (10 gg). Plates were then incubated at 37 oc for 18 to 24 hours. After the incubation, the inhibition diameters around each antibiotic disc were measured and in- terpreted as susceptible (S), intermediate (I) or resistant (R) in accordance with CLSI guidelines [18]. All isolates resis- tant to Vancomycin according to disk diffusion were re-test- ed using the gradient diffusion (E.TEST, bioMérieux, Mar. cy l'Étoile, France).
Molecular Testing for MRSA and PVL Strain IdentificationDNA was extracted from pure colonies using 10% Chelex (Bio Rad; California, US). In a labelled 2-ml tube, an equal volume of pure bacterial suspension and Chelex was incubated at for I hour. 'Ihe tube was then centrifuged at 22378 g, the supernatant was used for PCR.
For the conventional PCR (using the Red Taq Mix kit, Oxoid), different genes were targeted to confirm the positivity of the S. aureus using different primer pairs (supplementary table). Firstly, S. aureus species isolated by culture were confirmed by conventional PCR amplification of the nuc gene as described [19]. For the identification of MRSA, we targeted the mecA gene, using the protocol described by Murakami et al [20]. For PVL detection, we lukS-PV and lukF-PV [13]. For quality control of culture and PCR confir- mation, we used S. aureus strain (ATCC 33591). Gel elec- trophoresis was undertaken on all PCR amplicons in paral- lel with the I kb ladder (Thermofisher, Vilnius, Lithuania) which served as the rule to estimate the size of amplicons by using a 2% agarose gel and were visualized using the Gel Doc CZ instrument.
Data AnalysisStatistical analysis included descriptive analysis for calculation of percentage, frequency, mean and median val. ues and 95% confidence interval (95% CI). Associations of socio-demographic and clinical variables to S. aureus colonization were evaluated with the Pearson Chi-square test and crude Odds Ratios were estimated to quantify effect of risk factors. GraphPad software (version 9) was used for data analysis. A P value SO.05 was considered significant.
Ethical ApprovalThe study obtained ethical approval from the inde- pendent institutional ethics committee of the Fondation Cnngolaise pour la Recherche Médicale under number 021D,/CIE/FCRM/2021 , Prior to enrolment, participants provided written informed consent, Additionally, an administra. tive authorization was granted by the Ministry of Public Health,
Results
Socio-demographic Characteristics of the Recruited ParticipantsOne hundred and seventy-five (175) participants were included in this study, of whom 35 (20%) were wom- en. The median age was 26 years (range 23-29 years). Most of the participants were aged between 18 and 28 years (n=129, 73.7%). As shown in Table I, most of the partici- pants were living in the area 1 (50.9%) following by area 2 with 423% and for area 3.
Staphylococcus Aureus PrevalenceS. aureus was detected in 39 of the 175 partici- pants, corresponding to an S aureus colonization of 22%. Of the 39 participants colonized with S. aureus, a greater proportion of women were colonized (11/35, 31%) compared to 20% Of men (28/ 140as, Table I). The highest rate Of S. aureus carriage was identified in the age group 240 years, accounting for 29% (6/21) (Table I).
S. aureus carriage according to sampling site was identified as follows: of the participants carrying S. aureus, 29/39 (74%) carried S. aureus only in the nostrils, 6/39 (15%) carried S. aureus only in the oropharynx and 4/39 (10%) were dual carriers of S. aureus (Figure 2).
Evaluation of Risk Factors Associated to S. Aureus ColonizationIn Table II the risk factors associated to S- aureus colonization were assessed. None of the variables was signifi- cantly associated with S. aureus colonization. No significant differences (p. value 0.05) were observed for the risk fac- tors assessed.
Antibiotic Resistance RatesIn this study, a prevalence of (4/39) of isolates carrying the mecA gene (MRSA) and a prevalence of 23% (9/39) of isolates carrying the PVL gene were reported. It has been found 5% (2/39) of these strains were simultaneously PVL and mecA positive. 'Ihese two strains were isolated from men aged of 24 and 26 years old respectively who lived in the same neighborhocxi; Moungali, a densely populated area
Single, dual and multi-antibiotic resistances were common and of seven antibiotics tested, there was no resistance to tigecycline. Cefaclor had highest resistance rates (26%) expressed by the tested, followed by Azithromycin and Erythromycin (21 % each) with resistance rates of up to 20%. Although most of these strains presented a high level of resistance to the antibiotics tested, however some of them were effective on S, aureus, such as Cefoxitin (15%) and Vancomycin (13%) with a resistance rate of less than 16%, as shown in Table III. The comparison of the rate of resistance between MRSA and MSSA showed that MRSA strains were susceptible to almost all the antibiotics tested in this study. Methicillin-sensitive S aureus (MSSA) presented an important resistance heno Interestin , none of the PVL+ MRSA strains were resistant to any of the tested antibiotics. One of the PVL-negative MRSA strain was resistant to only one antibiotic which is Cefoxitin.
Resistance Rate Between Antibiotics Users and NonUsersThe prevalence of antibiotic resistance between participants who had used antibiotics within the last three months, and those who have not used, was investigated (Table IV). An increase in resistance rates of S. aureus, iso- lated from participants who had not used antibiotics in the last three months, to three specific antibiotics (CC2, LZD and VA) was observed (P— 0.03; 0.001 and respective. ly). No difference was observed with other antibiotics what- ever the study group.
Discussion
This study has several important findings. This is the first study of S aureus colonization in healthy Congolese adults from the urban community. It shows a high prevalence (22%) S. aureus carriage and a high proportion Of MRSA (15%). These findings could have significant impact on management of hospitalized patients for elective or emergency surgical procedures where preoperative decolonization is important for preventing S. aureus infection and requires appropriate use of specific targeted antibiotics. Whilst these results provide baseline data for future investi• gations, further studies are required to ascertain country. wide prevalence, decolonization and impact on management of hospitalized patients.
Colonization by S aureus represents a potential risk for the development of subsequent infections [21], There is a paucity of available data in the Central Africa re- gion, but the prevalence of 22% S. aureus carriage in healthy Congolese participants in this study is lower compared to that reported by Schaumburg et 2013 [22] in Gabonese population showing the prevalence of 40% and 42%, after one month delivery, of S. aureus carriage respectively from mothers and their children. Indeed prevalence from this was higher compared to what reported from DRC at 133% from population in the community [23] Nasal carriage has been shown to be the main reservoir involved in human-- to-human transmission of S. aureus in hospitals, as well as in the community, and is also the main risk factor for infec- tion, since colonization may be a prerequisite for S. aureus infection [24]. S. aureus infections in humans are most of- ten due to the bacteria present at the site of colonization [25]. In the present study, it is important to note that in the present study most represented gender was male.
More importantly, of the 39 S. aureus carriers detected in this study, 75% were nasal carriers, only 15% were oropharyngeal carriers and the remaining 10% were carriers in both sites. 'Ihese results suggest that nasal colonization is the main site for S. aureus colonization in the community in the Republic of Congo, as demonstrated by Von. Eiff et al., 2001 [251, who reported that 86% of S. aureus strains collected from blood and nasal have identical clones using the Pulsed-Field Gel Electrophoresis method. It is therefore important to control nasal carriage of S. aureus in order to reduce the incidence of S. aureus infections in tx»th community and nosocomial settings.
Another parameter that needs to considered in interpretation of the results is the age of the participants. It has been reported that S aureus colonization rates are high immediately after birth, compared with the elderly in whom colonization rates appear to decrease over time [26,27].
Although in the present study in Brazzaville (RoC), the age group of 18-28 years was the most represented, S. aureus colonization was reported to the highest in the adult age group 240 years including more but not significant nasal S. aureus infection.
In this study, a prevalence of 23% of PVL+ among S. aureus isolates was reported in the MRSA and MSSA groups, It is lower than those from Saudi Arabia and Tunisia with 30% and 4196, respectively (10,28). Among PVL+ S. aureus, a prevalence of 22% (2/9) MRSA was identified, similar results were observed also in Tunisia 1291. Carriage of this toxin within the Congolese community poses a threat, as PVL has been shown to reduce the effectiveness of the immune system by killing neutrophils and other immune cells [301. In addition, PVL+ isolates are particularly difficult to treat if nasal carriage develops into infection.
In this study, a prevalence of 23% of PVL+ among S. aureus isolates was reported in the MRSA and MSSA groups, It is lower than those from Saudi Arabia and Tunisia with 30% and 41%, respectively 110,281. Among PVL+ S. aureus, a prevalence of 22% (2/9) MRSA was identified, similar results were observed also in Tunisia [29]. Carriage of this toxin within the Congolese community poses a threat, as PVL has been shown to reduce the effectiveness of the immune system by killing neutrophils and other immune cells [301. In addition, PVL+ isolates are particularly difficult to treat if nasal carriage develops into infection,
The molecular profile of only two PVL+ MRSA strains identified in the present study were sensitive to all tested antibiotics. In contrary to the work reported by Sadar et al, 2022 showing that PVL+ MRSA strains presenting higher resistance rate vs PVL+ MSSA strains [311, Discrep- ancies in findings may be attributed to sample size, type of sample, geographical area, methodology used and the preva- lence of strains with specific antibiogram profile. In com- parison with the results of Baran et ale, 2010 1321 who detect- ed PVL only among MRSA isolates in Turkey and Santosan• ingsih et ale, 2016 who reported positive PVL only among MSSA isolates in Indonesia [33], in the current study the P VL in both MSSA and MRSA isolates were detected, which represents a major public health problem for the Con- golese population.
A prevalence of 10% of MRSA isolates was found in this study. In DRC, a prevalence of (33%) MRSA isolates was reported in healthy participants and these isolates were significantly resistant to many more classes of antibiotics [23]. At least 20% of MSSA isolates were resistant to azythromycin, and erythromycin indicating that antibiotics are less effective in therapy against S aureus.
Malaria is a major cause of hospitalization and inhospital mortality among children in Africa [341, and in the Republic of Congo the disease is endemic, where treat. ment is almost always combined with at least one antibiotic tested in this study, The high level of resistance to these antibiotics (Azythromycin and Erythromycin) may be linked to their frequent use in the treatment of malaria. Of the 6 antibiotics used, only one, Tygecycline, was effective on all S aureus isolates tested. This antibiotic must be used with care, as it conserved its effectivity among all the antibi- otics we have used against S. aureus isolates. Unfortunately, no strong legislation in the Cnngo controls the use or sale of antibiotics in the community. Antibiotic resistance is a glob. al public health problem. These results underline the importance of adopting control measures against the misuse of antibiotics.
Limits have been identified in this study, First, the sample collection time was very short. Consequently, the dynamics of S. aureus isolates over a longer period like 12 months could not be assessed. Second, a multilocus sequence typing (MLST) was not performed, so the association between MRSA or MSSA and circulating MIST could not be established. Third, the use of selective media would have increased the detection and therefore colonization rates of S. aureus in addition to the small selection of antimicrobial. Fourth, rural or semi-urban areas were not consid- ered in this study. Differences in the profile of these ecosystems are also important for understanding the mechanism of resistance in different regions. Ihese shortcomings should be considered in future studies to provide more information on S. aureus colonization in the community.
Conclusion
A prevalence of 22%, of S aureus carriage was re. ported including the presence of MRSA isolates (10 % of the S. aureus found in carriers). Among S. aureus isolates, 23% of isolates tested carried the p VI, gene. The profile of P VL positive MRSA strains was identified, showing the importance of investing in intensive surveillance of S. aureus in the community
Conflicts of Interest
The authors declare that they have no conflicts Of interest.
Funding
This study was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Founda- tion, grant 404893180 to FS and FN). This work received support from the Central Africa Clinical Research Network, CANTAM (EDCTPCSA2020NoE3100) and from the cm. tral Africa Humboldt research Hub (HRH.Coca) funded by the Alexander von HumtX)ldt foundation. CCMM was sup- ported by the Fondation Merieux.
Authors' Contributions
Study design: FN, FS. Implementation of the study. CCMM, JNGI, NM, KB, AMM. Analysis of the results: CCMM, CJV, RA, LE- All authors contributed to writing the manuscript, read and approved the final version.
Acknowledgements
The authors thank all the participants for their cooperation. We appreciate Ms Provindence SITA for her technical assistance in the laboratory. Ihe funders did not play a role in the design of the study, collection, analysis, and interpretation of data, as well as the writing of the manuscript.
- Piewngam P, M Otto (2024) Staphylococcus aureus colonisation and strategies for decolonisation. Lancet Microbe.
- Deyno S, et ale (2017) Antimicrobial resistance profile of staphylcxoccus aureus isolates isolated from ear discharges of patients at University of Hawassa comprehensive special. ized hospitaL BMC Pharmacol Toxicol, 18:35.
- Pires FV, et al. (2014) Nasal carriage of Staphylococcus aureus in Botucatu, Brazil: a population-based survey. PLOS one, 9: e92537.
- Bartoloni A, et al. (2013) Low prevalence of methi- cillin-resistant Staphyloccxcus aureus nasal carriage in urban and rural community settings in Bolivia and Peru. Int J Infect Dis, 17:839-42.
- Riya Mukherjee AP, Ramendra Pati Pandey, Vethakkani Samuel Raj (2021) Antimicrobial Resistance in Staphylococcus aureus. IntechOpen.
- Ndhlovu GON, et al. (2021) Molecular epidemiology of Staphylococcus aureus in African children from rural and urban communities with atopic dermatitis. BMC Infect Dis, 21: 348.
- Onanuga A, TC Temedie (2011) Multidrug-resistant intestinal Staphylococcus aureus among self-medicated healthy adults in Amassoma, South-South, Nigeria. J Health Popul Nutr, 29: 446-53.
- Schaumburg F, et al. (2014) Transmission of Staphylococcus aureus between mothers and infants in an African setting. Clin Microbiol Infect, 20: O390-6.
- Laux C, A Peschel, B Krismer, (2019) Staphylococcus aureus Colonization of the Human Nose and Interaction with Other Microbiome Members. Microbiol Spectr, 7.
- Bazzi AM, et al. (2015) Prevalence of Panton-Valentine leukocidin-positive methicillin-susceptible Staphylococcus aureus infections in a Saudi Arabian hospital. J Infect Public Health, 8: 364-8.
- Chen X, et al. (2015) Rapid detection of Staphylococcus aureus in dairy and meat foods by combination of capture with silica-coated magnetic nanoparticles and thermophilic helicase-dependent isothermal amplification. J Dairy Sci, 98: 1563-70.
- Leistner R, et al. (2022) Skin Infections Due to Panton-Valentine Leukocidin-Producing S. Aureus. Dtsch Arztebl Int, 119: 775-84.
- Shallcross LJ, et al, (2013) 'lhe role Of the Panton-Valentine leucocidin toxin in staphylococcal disease: a systemat- ic review and meta-analysis. Lancet Infect Dis, 13:43-54,
- Flora Cruz-L6pez I-VT, Rayo Morfin-Otero, Adriån Martinez-Meléndez„ Adriån Camacho-Ortiz, Eduardo Rodriguez-Noriega, Elvira Garza-Gonzålez (2020) Dynamics of colonization in patients with health care-associated infections at step-down care units from a tertiary care hospital in Mexico. American Journal oflnfection Control, 48: 1329-35.
- Rachel Moyen EN, Gabriel Ahombo, Nina Esther Ontsira, Claudette Gatsele Yala, Obengui, Simon Charles Kobawila, Delphin Louembe (2014) Comparative Study to Amino Glycoside Antibiotics Resistance of Staphylococci Strains Isolated from Wounds at Brazzaville. International Journal of Science and Research (IJSR) 6.
- Ahombo Gabriel MR, Baloki Ngoulou Tarcisse, Kayath Aimé Christian, Ontsira Ngoyi Nina Esther (2019) Genetic Determinism in Community Staphylococcus and Methicillin-Resistant Clinics in Brazzaville, Republic of Congo. International Journal of Innovative Research in Medical Science (IJIRMS), 4: 454-9.
- Institut National de la Statistique, R.o.C. (2023) Communiqué relatif à la publication des résultats préliminaires du RGPH-5. Google.
- (CLSI), C.L.S.I. (2020) Performance standards for antimicrobial susceptibility testing.
- Brakstad K Aasbakk, JA Maeland (1992) Detection of Staphylococcus aureus by polymerase chain reaction amplification of the nuc gene. J Clin Microbiol, 30: 1654-60.
- Murakami K, et al. (1991) Identification of methicillin-resistant strains of staphylococci by polymerase chain reaction. J Clin Microbiol, 29:2240-4.
- Schaumburg F, et al. (2014) New epidemiology of Staphylococcus aureus infection in Africa. Clin Microbiol Infect, 20: 589-96.
- F Schaumburg, ASA, G Mombo-Ngoma, H Kaba, RM Zoleko, DA Diop, JR Mackanga, et al. (2013) Transmission of Staphylococcus aureus between mothers and infants in an African setting. Clinical Microbiology and Infection, 20: O390-6.
- Phaku P, et al. (2016) Unveiling the molecular basis of antimicrobial resistance in Staphylococcus aureus from the Democratic Republic of the Congo using whole genome sequencing. Clin Microbiol Infect, 22: 644 e1-5.
- Miller M, et al. (2009) Staphylococcus aureus in the community: colonization versus infection. PLoS One, 4: e6708.
- Christof Von EiffKB, Konstanze Machka, Holger Stammer, Georg Peters, (2001) Nasal Carriage as a Source Of Staphylococcus Aureus Bacteremia. The New England Jour- nal of Medicine, 344: 11-6.
- Kinabo GD, et al. (2013) Dynamics of nasopharyngeal bacterial colonisation in HIV-exposed young infants in Tanzania. Trop Med Int Health, 18: 286-95.
- Olalekan AO, et al. (2012) Clonal expansion accounts for an excess of antimicrobial resistance in Staphylococcus aureus colonising HIV-positive individuals in Lagos, Nigeria. Int J Antimicrob Agents, 40: 268-72.
- Chaouch C, KS Tilouche L, Ketata S, Bouallegue O, Boujaafar N, (2015) Panton-Valentine leukocidin-positive osteoarticular infections. Médecine et Santé Tropicales, 25: 184-8.
- Dohin B, GY Kohler R, Lina G, Vandenesch F, Vanhems P, et al. (2007) Pediatric bone and joint infections caused by Panton-Valentine leukocidin positive Staphylococcus aureus. Pediatry Infection Disease Journal, 26.
- Genestier AL, et al. (2005) Staphylococcus aureus Panton-Valentine leukocidin directly targets mitochondria and induces Bax-independent apoptosis of human neutrophils. J Clin Invest, 115: 3117-27.
- Sadat A, et al. (2022) Prevalence and Characterization of PVL-Positive Staphylococcus aureus Isolated from Raw Cow's Milk. Toxins (Basel), 14.
- Baran CB, et al. (2010) [Investigation of Panton-Valentine leukocidin gene, SCCmec gene cassette types and genotypes of methicillin-resistant Staphylococcus aureus strains isolated from outpatients]. Mikrobiyol Bul, 44: 533-45.
- Santosaningsih D, et al. (2016) Characterisation of clinical Staphylococcus aureus isolates harbouring mecA or Panton-Valentine leukocidin genes from four tertiary care hospitals in Indonesia. Trop Med Int Health, 21: 610-8.
- Kazembe LN, I Kleinschmidt, BL Sharp (2006) Patterns of malaria-related hospital admissions and mortality among Malawian children: an example of spatial modelling of hospital register data. Malar J. 5: 93.
FIGURE 1
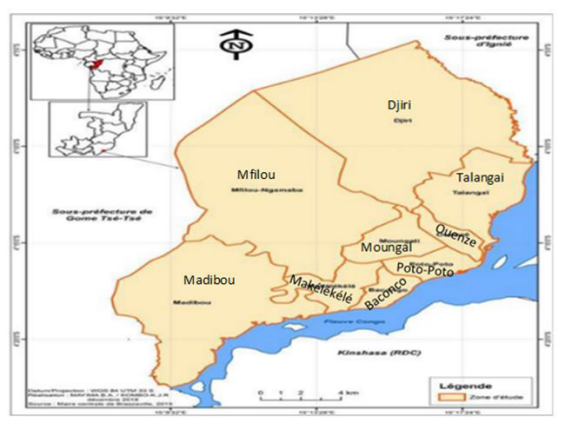
Figure 1: Brazzaville city localisation, study area circumscriptions
FIGURE 2
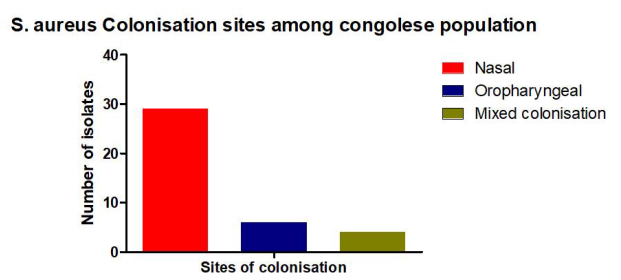
Figure 2: S. aureus colonization prevalence by collection site, in the 39 patients who were found to be positive.
Tables at a glance
Figures at a glance