Association of Serum Albumin and Cardiovascular Risks in a Hiv Cohort on Art at a Tertiary Care Hospital
Received Date: April 29, 2023 Accepted Date: May 29, 2023 Published Date: June 02, 2023
doi: 10.17303/jaid.2023.10.101
Citation: Arun kumar R, Nithyananda Chowtha (2023) Association of Serum Albumin and Cardiovascular Risks in a Hiv Cohort on Art at a Tertiary Care Hospital. J HIV AIDS Infect Dis 10: 1-14
Abstract
Background
The introduction of antiretroviral therapy led to drastic change in mortality and morbidity related to HIV and AIDS. Particularly now cardiovascular disease has emerged as most important cause of death in HIV individuals [2]. In additional to traditional risk factors of cardiovascular events, chronic inflammation, immune activation and endothelial dysfunction further attribute to cardiovascular risk in HIV population. It is vital to assess the cardiovascular risk in all PLHIV so as to mitigate and initiate risk reduction techniques [4].
Low serum albumin levels have been linked to an increased risk of cardiovascular death. In this study, we compared the cardiovascular risk score which is calculated by HIV specific CVD risk assessment tool (D:A:D score) with serum albumin.
Aim
To evaluate the relationship between serum albumin and calculated cardiovascular risk using D:A:D calculator in PLHIV on stable ART.
Patients and Methods
A hospital based cross- sectional analytical study was conducted among 159 patients attending ART clinic in a tertiary care center, who was on stable ART for minimum 2 years between age group of 18-60 was included.
Results
Among 159 patients, 37(23.3%) patients had low Albumin. D:A:D CVD risk at 5 years distribution among participants was calculated, around 28.9% (n=46) had very high risk of D:A:D CVD at 5 years and 20.8% (n=33) showed high risk.
Among patients with low risk of CVD at 5 years, the mean (SD) serum albumin was highest, 4.19 (0.25) mg/dl as compared to other risk categories and this difference was found to be statistically significant (p=0.04)
Among patients with low serum albumin, 40.5% (n=15) showed moderate and very high risk of CVD at 5 years whereas only 2.7% (n=1) showed low risk of CVD at 5 years. This difference was not found to be statistically significant
Conclusion
We found out that low risk of CVD at 5 years was significantly associated with high mean serum albumin levels. Lower levels of serum albumin can be used a predictor for cardiovascular risk among PLHIV. Serum albumin measurements could potentially improve the prediction of short-term adverse outcomes in HIV-infected individuals.
Keywords: Hiv Cardiovascular Risk; Serum Albumin; Hiv; Serum; Infectious Diseases
Introduction
In 2021, around 6,50,000 people have died due to causes related to HIV and 1.5 million people were infected by HIV. Globally, 38.0 million people are living with HIV as of 2019, of those 68% people were receiving lifelong antiretroviral therapy [1].
The introduction of antiretroviral therapy led to drastic change in mortality and morbidity related to HIV and AIDS. With recent advances in the treatment mortality and wide spread availability of more effective ART, the deaths due to HIV related events decreased in comparison to non HIV related events, most deaths in HIV population are now attributable to non-communicable illnesses [2]. Particularly now cardiovascular disease has emerged as most important cause of death in HIV individuals. In a meta-analysis and systemic review in comparison to general population there is a 2.16-fold increase in cardiovascular disease in HIV population. They also found association of HIV infection with risk of cardiovascular disease was stronger in younger than older individuals [3]
It is vital to assess the cardiovascular risk in all PLHIV so as to mitigate and initiate risk reduction techniques. Traditional risk factors for non-communicable diseases such as smoking, dyslipidaemia, diabetes mellitus, and hypertension are prevalent in HIV affected population. In addition to this chronic inflammation and immune activation, endothelial dysfunction is related to cardiovascular risk in HIV (even in setting of successful viral suppression using ART). Specific HIV medication like Abacavir, Protease inhibitors also showed to increase cardiovascular risk in HIV individuals. The relationship between HIV infection and atherosclerotic disease has been linked to endothelial dysfunction and arterial inflammation, according to studies. Cardiovascular risk prediction equations and scores have been developed worldwide and are widely used to predict individuals who are at risk of CVD. Still it is not very clear which is the most accurate and optimal one to predict risk of CVD.
D:A:D score developed in a study on Data Collection on Adverse Effects of Anti-HIV Drugs Cohortby Friis-- Moller et al was based on incorporation of some HIV related factors such as IND,LPV/r,ABC exposure in cardiovascular risk assessment tool and it has improved the predictability [6].
In HIV infected individuals the serum albumin has been recognized as an independent prognostic factor in cardiovascular risk assessment. The two mechanism which are directly related to pathogenesis of cardiovascular disease is chronic inflammation and hypertriglyceridemia. Low serum albumin levels have been linked to an increased risk of cardiovascular death. In patients with HIV, lower serum albumin concentration has been associated with an increased risk of mortality. In people living with HIV, low serum albumin concentration may be associated with the development of serious non-AIDS events (SNAEs).
There is paucity of data regarding association of serum albumin and cardiovascular risk in HIV population. In this study, we compared the cardiovascular risk score which is calculated by HIV specific CVD risk assessment tool (D:A:D score) with serum albumin. If an association between serum albumin which is easily available and low of cost is found, it can be used as an additional tool in cardiovascular risk stratification in patient living with HIV.
Material and Methods
A hospital based cross-sectional analytical study was conducted among patients attending ART clinic in a tertiary care center. The study was conducted over a period of 2 years.
Total sample size calculated was 159. Sample size was calculated based on the assumption that 11.7% of PLHIV will have hypoalbuminemia based on previous studies, with following assumptions Z= 1.96, 5% level of significance, 80% power, 95% confidence interval.
Inclusion criteria
Patients with the following criteria were included in the study. On stable ART at least for 2 years and age group between 18- 60 years.
Exclusion criteria
Factors affecting albumin levels (CLD, Nephrotic syndrome, malnutrition syndrome, trauma, surgery), on statins, Patient not adherent to ART (< 95%), Terminal illness (malignancy), Pregnancy
Results
The mean age of the population was 43.7 years. 54.1%(n=86) were male and 45.9%(n=73) were females. 45.9%(n=73) from urban and 54.1%(n=86) from rural, The body mass index distribution among participants. 35.9% (n=57) were normal weight, whereas 33.9% (n=54) were found to be in obese BMI category. 14.5% (n=23) had positive family history of CVD and 85.5% (n=136) had no famiy history of CVD. 4.4% (n=7) were found to be diabetic and 95.6% (n=152) were non-diabetic. Only 9.4% (n=15) were found to be hypertensive and 90.6% (n=144) were non-hypertensive. ART duration distribution among participants. 24.5% (n=39) had less than 5 years of ART duration, 70.4% (n=112) had 6-10 years of ART duration and only 5.1% (n=8) had more than 10 years of ART duration.
Only 23.3% (n=37) had low serum albumin and 76.7% (n=122) had normal level of serum albumin. D:A:D CVD risk at 5 years distribution among participants is described in Table 22. Around 28.9% (n=46) had very high risk of D:A:D CVD at 5 years and 20.8% (n=33) showed high risk.
Among patients with low serum albumin, 40.5% (n=15) showed moderate and very high risk of CVD at 5 years whereas only 2.7% (n=1) showed low risk of CVD at 5 years. This difference was not found to be statistically significant (p=0.30).
Correlation between Serum albumin and D:A:D CVD risk at 5 years with Pearson correlation coefficient is -0.005 (weak correlation) and it is not statistically significant (p=0.95).
Among patients with low risk of CVD at 5 years, the mean (SD) serum albumin was highest, 4.19 (0.25) mg/dl as compared to other risk categories and this difference was found to be statistically significant (p=0.04).
Discussion
In this study, we aimed to evaluate the relationship between serum albumin/albumin globulin ratio and cardiovascular risk using D:A:D calculator in PLHIV on stable ART. According to our study results around 50% of the population are coming under high and very high risk category of cardiovascular risk. A significant association between mean serum albumin level and CVD risk at 5 years was also found among the study patients.
The increased risk of CVD among PLWH has been clearly demonstrated in earlier studies [11,12]. Hence in this population, the development of interventions for cardiovascular health promotion and CVD prevention is war-ranted. However, most of the CVD risk assessment tools have been derived from the general population and not from PLHIV. So, their ability to predict CVD in PLHIV is inconsistent and inaccurate. Therefore, to accurately predict CVD risk in PLHIV, a new CVD risk assessment tool derived from PLHIV accounting for variables specific to HIV infection such as CD4 count, treatment and duration of ART along with various traditional risk factors. This tool could determine which patients would most benefit from primary prevention strategies [13,14].
In our study we found males had high risk of CVD at 5 years than females. In a cross-sectional study conducted among people with HIV undergoing ART treatment in South Africa, males showed higher prevalence of metabolic CVD risk factors than females [16]. Our study showed high risk of CVD scores among age group between 40-60 years of age. These findings were consistent with other study where people above 50 years of age showed risk factors of CVD as compared to younger age groups [16].
Around 50% of the participants in our study had higher BMI and were overweight and obese. Overweight people have been demonstrated to have higher rates of cardiovascular disease mortality and morbidity, especially when there is central adipose tissue accumulation [17].
We found a high proportion of patients with HTN, DM, and dyslipidemia. The findings are similar to other Indian studies that have shown high prevalence of these diseases in the Indian population. In India, non-communicable diseases account for over 63% of all fatalities, with cardiovascular disease accounting for 27% of these deaths and affecting 45% of adults between the ages of 40 and 69 [18]. Overall prevalence for hypertension in India was 29.8% (95% con) [19]. Prevalence of DM and impaired fasting blood glucose (IFG) in India was 9.3% and 24.5% respectively. In India, 25-30% urban population and 15-20% rural population have dyslipidemia [21].
The results of our study are in line with those of previous studies. A previous study indicated that a low serum albumin level is a predictor for both short- and longterm significant non-AIDS events, including cardiovascular events. This finding was independent of other prognostic factors, including both traditional cardiovascular disease risk factors (age, lipid profile, hemoglobin level, and blood pressure), HIV-specific risk factors (HIV-1 RNA load and CD4+ T-cell count). The authors highlighted that a low serum albumin level may be a useful marker of risk of non-- communicable diseases, particularly in resource-limited settings [10]. An association between serum albumin levels and subsequent clinical events, including cardiovascular events, has been demonstrated previously in PLHIV [23,24]. Like in our study, several observational studies have also demonstrated the association between serum albumin and mortality in HIV-infected persons. The researchers of these studies have shown a uniform and strong inverse association between serum albumin level and incident health-related outcomes, including overall mortality and AIDS-related cardiovascular morbidities [24,25].
In our study, we could not find a correlation between serum albumin level and D:A:DCVD risk at 5 years and between serum albumin level and CD4 count at the time of the initiation of ART. Likewise, an earlier study also found no association between serum albumin and AIDS [8]. However, contradictory results were also obtained. In an earlier study, in HIV/AIDS patient’s serum albumin level was found to correlate with CD4 counts and was used as a marker of immune suppression. The discrepancy in the results might be due to the small sample size of our study [26].
The findings of this study are relevant in the context of low- and middle-income countries like India. Serum albumin is also more easily obtained than other expensive biomarkers that have previously been associated with nonAIDS disease and related morbidity and mortality (e.g., chronic inflammatory markers, microbial translocation, hypercoagulation, and immune activation markers) [28,29]. None of these biomarkers have been found to be reliable to be used in routine clinical practice. Thus, based on our data, and previous reports, serum albumin may be considered to be included in future HIV prognostic indices for non-AIDS morbidity, especially cardiovascular morbidity. Thus, identification of serum albumin level as a clinically available prognostic marker may help inform non-communicable disease pathogenesis (e.g. cardiovascular diseases) in PLHIV as well as provide added value for a personalized approach to these conditions to stratify the risk.
Conclusion
In our study, we calculated cardiovascular risk score at 5 years for people with HIV which is calculated by HIV specific CVD risk assessment tool (D:A:D score) and compared with serum albumin as a prognostic factor. We also studied demographic and clinical profile of PLHIV undergoing stable ART. A significant association between mean serum albumin level and CVD risk at 5 years was also found among the study patients. We found out that low risk of CVD at 5 years was significantly associated with high mean serum albumin levels. Lower levels of serum albumin can be used a predictor for cardiovascular risk among PLHIV. Serum albumin measurements could potentially improve the prediction of short-term adverse outcomes in HIV-infected individuals.
- World Health Organization. HIV [Internet]. World Health Organization. 2021
- Montessori V, Press N, Harris M, Akagi L, Montaner JSG (2004) Adverse effects of antiretroviral therapy for HIV infection. C Can Med Assoc J 170: 229.
- Shah S, Smith CJ, Lampe F, Youle M, Johnson MA, Phillips AN et al. (2007) Haemoglobin and albumin as markers of HIV disease progression in the highly active antiretroviral therapy era: relationships with gender. HIV Med 8: 38-45.
- Dirajlal-Fargo S, Kulkarni M, Bowman E, Shan L, Sattar A, Funderburg N et al. (2018) Serum Albumin Is Associated With Higher Inflammation and Carotid Atherosclerosis in Treated Human Immunodeficiency Virus Infection. Open Forum Infect Dis 1: 5.
- Ronit A, Kirkegaard-Klitbo DM, Dohlmann TL, Lundgren J, Sabin CA, Phillips AN et al. (2020) Plasma Albumin and Incident Cardiovascular Disease: Results From the CGPS and an Updated Meta-Analysis. Arterioscler Thromb Vasc Biol 40: 473-82.
- Friis-Møller N, Ryom L, Smith C, Weber R, Reiss P, Dabis F et al. (2016) An updated prediction model of the global risk of cardiovascular disease in HIV-positive persons: The Data-collection on Adverse Effects of Anti-HIV Drugs (D:A:D) study. Eur J Prev Cardiol 23: 214-23.
- Dirajlal-Fargo S, Kulkarni M, Bowman E, Shan L, Sattar A, Funderburg N et al. (2018) Serum Albumin Is Associated With Higher Inflammation and Carotid Atherosclerosis in Treated Human Immunodeficiency Virus Infection. Open Forum Infect Dis. 2018 Nov 1: 5.
- Ronit A, Kirkegaard-Klitbo DM, Dohlmann TL, Lundgren J, Sabin CA, Phillips AN et al. (2020) Plasma Albumin and Incident Cardiovascular Disease: Results From the CGPS and an Updated Meta-Analysis. Arterioscler Thromb Vasc Biol 40: 473-82.
- Chien SC, Chen CY, Lin CF, Yeh HI (2017) Critical appraisal of the role of serum albumin in cardiovascular disease. Biomark Res 5.
- Ronit A, Sharma S, Baker JV, Mngqibisa R, Delory T, Caldeira L et al. (2018) Serum Albumin as a Prognostic Marker for Serious Non-AIDS Endpoints in the Strategic Timing of Antiretroviral Treatment (START) Study. J Infect Dis 217: 405.
- Shah ASV, Stelzle D, Ken Lee K, Beck EJ, Alam S, Clifford S et al. (2018) Global Burden of Atherosclerotic Cardiovascular Disease in People Living with the Human Immunodeficiency Virus: A Systematic Review and Meta-Analysis. Circulation 138: 1100.
- Bavinger C, Bendavid E, Niehaus K, Olshen RA, Olkin I, Sundaram V et al. (2013) Risk of cardiovascular disease from antiretroviral therapy for HIV: a systematic review. PLoS One 8.
- Lewden C, May T, Rosenthal E, Burty C, Bonnet F, Costagliola D et al. (2008) Changes in causes of death among adults infected by HIV between 2000 and 2005: The “Mortalité 2000 and 2005” surveys (ANRS EN19 and Mortavic). J Acquir Immune Defic Syndr 48: 590-8.
- Triant VA, Perez J, Regan S, Massaro JM, Meigs JB, Grinspoon SK et al. (2018) Cardiovascular Risk Prediction Functions Underestimate Risk in HIV Infection. Circulation 137: 2203-14.
- Chien SC, Chen CY, Lin CF, Yeh HI (2017) Critical appraisal of the role of serum albumin in cardiovascular disease. Biomark Res 5: 1–9.
- Chien SC, Chen CY, Lin CF, Yeh HI (2017) Critical appraisal of the role of serum albumin in cardiovascular disease. Biomark Res 5: 1–9.
- Akil L, Anwar Ahmad H (2011) Relationships between Obesity and Cardiovascular Diseases in Four Southern States and Colorado. J Health Care Poor Underserved 22: 61.
- Hypertension in India [Internet]. [cited 2022 Oct 27].
- Anchala R, Kannuri NK, Pant H, Khan H, Franco OH, Di Angelantonio E et al. (2014) Hypertension in India: a systematic review and meta-analysis of prevalence, awareness, and control of hypertension. J Hypertens 32: 1170.
- Mathur P, Leburu S, Kulothungan V (2022) Prevalence, Awareness, Treatment and Control of Diabetes in India From the Countrywide National NCD Monitoring Survey. Front Public Heal 10: 205.
- Dyslipidemia | National Health Portal of India [Internet]. [cited 2022 Oct 27].
- Scherzer R, Heymsfield SB, Rimland D, Powderly WG, Tien PC, Bacchetti P et al. (2017) Association of serum albumin and AST with 5-year all-cause mortality in HIV/HCV Coinfection and HIV Monoinfection. AIDS 31: 71.
- Sudfeld CR, Isanaka S, Aboud S, Mugusi FM, Wang M, Chalamilla GE et al. (2013) Association of serum albumin concentration with mortality, morbidity, CD4 T-cell reconstitution among tanzanians initiating antiretroviral therapy. J Infect Dis 207: 1370–8
- Feldman JG, Burns DN, Gange SJ, Bacchetti P, Cohen M, Anastos K et al. (2000) Serum albumin as a predictor of survival in HIV-infected women in the Women’s Interagency HIV study. AIDS 14: 863–70.
- Siedner MJ, Hunt PW (2018) All About the Albumin? Prognostic Capacity of Serum Albumin in Patients With Treated HIV Infection. J Infect Dis 217: 347.
- Balgi V, Nayak V, K SD (2019) Study of Serum Albumin Level in Subjects with HIV Infection, in Relation to CD 4 Count, as a Marker of Immune Suppression ORIGINAL RESEARCH.
- Mooney S, Tracy R, Osler T, Grace C (2015) Elevated Biomarkers of Inflammation and Coagulation in Patients with HIV Are Associated with Higher Framingham and VACS Risk Index Scores. PLoS One 1; 10.
- Duffau P, Wittkop L, Lazaro E, Le Marec F, Cognet C, Blanco P et al. (2015) Association of immune-activation and senescence markers with non-AIDS-defining comorbidities in HIV-suppressed patients. AIDS 29: 2099–108.
- Ndlovu KCZ, Chikobvu P, Mofokeng T, Gounden V, Assounga A (2019) Serum albumin and mortality in patients with HIV and end-stage renal failure on peritoneal dialysis. PLoS One 14.
FIGURE 1
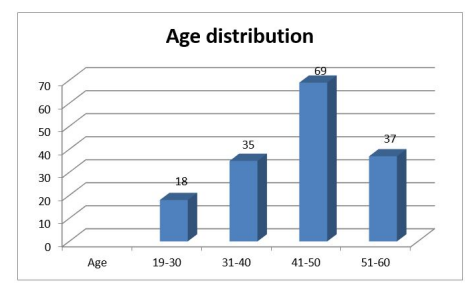
Figure 1: Age distribution of participants (N=159)
FIGURE 2
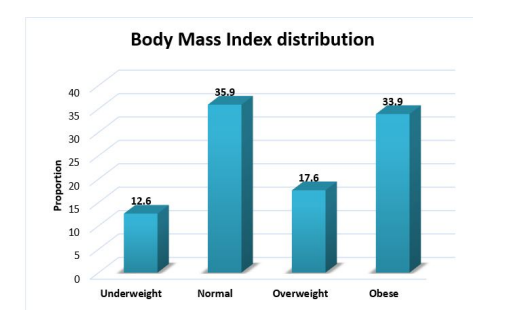
Figure 2: Body Mass Index distribution of participants (N=159)
FIGURE 3
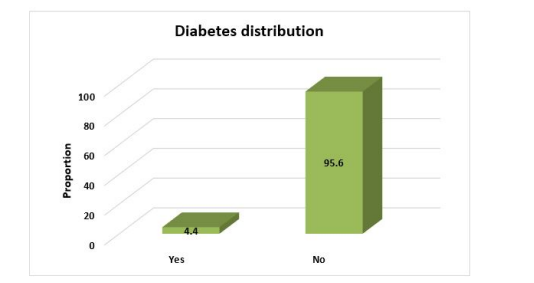
Figure 3: Diabetes distribution among participants (N=159)
FIGURE 4
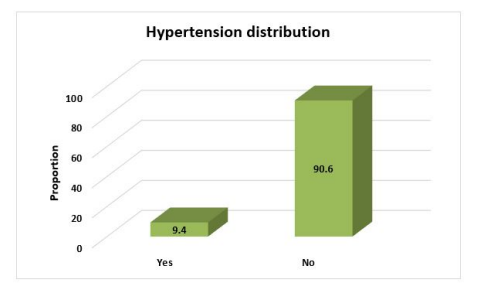
Figure 4: Hypertension distribution among participants (N=159)
FIGURE 5
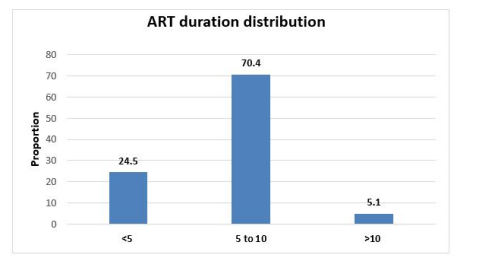
Figure 5: ART duration distribution
FIGURE 6
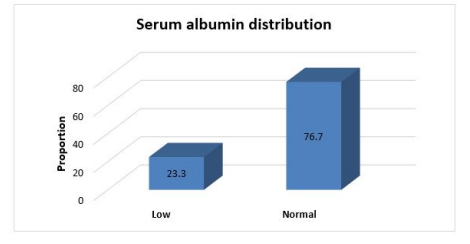
Figure 6: Serum albumin distribution among participants (N=159)
FIGURE 7
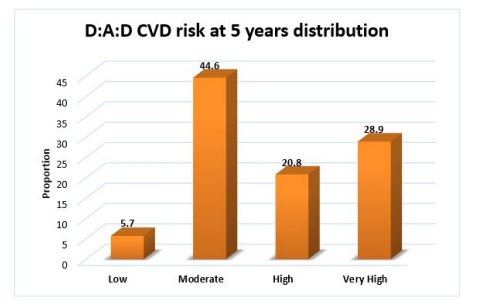
Figure 7: D:A:D CVD risk at 5 years distribution among participants (N=159)
Tables at a glance
Figures at a glance