The Impact of Spiritual Health Care on HIV/AIDS Patients’ Adherence to Haart
Received Date: April 02, 2025 Accepted Date: April 15, 2025 Published Date: April 19, 2025
doi: 10.17303/jaid.2025.12.101
Citation: Che Joseph Ngwa, Ebob Besem Margaret, Doumta Charles Falang, Same Ekobo Legrand, Nsagha Dickson Shey (2025) The Impact of Spiritual Health Care on HIV/AIDS Patients’ Adherence to Haart. J HIV AIDS Infect Dis 11: 1-15
Abstract
Background: HIV infection still stands till date as a threat to human populations all over the world due to its chronicity, morbidity and mortality, related to it immunosuppressive ability. As at 2018, the prevalence of HIV/AIDS in Cameroon was 3.4%. Despite the high level of morbidity and mortality of this disease, the health system is still faced with challenges in ensuring adherence to therapy.
Objective: To Determine the Impact of spiritual health care on adherence to HIV/AIDS Therapy.
Method: This was a quantitative and an Interventional study design. The participants were recruited into an intervention and a control arm through a simple random sampling method from Limbe and Buea Regional Hospitals, Cameroon by using a sample frame. By the use of Probability Proportionate to size, 96 participants and 134 participants were sampled from Buea and Limbe Regional Hospital Respectively and were randomly assigned to the intervention and the control arms.
Result: Our results on adherence showed that, the proportion of participants adhering to HAART increased significantly from 70(70.0%) at baseline to 83 (83.0%) at post-intervention in the intervention group. (p=0.030). Though the control group witnessed an increase in adherence, the increase was not statistically significant. Being at least 38 years old (AOR=2.15, 95% CI: 1.02 – 4.54), being a female (AOR=2.15, 95% CI: 1.6 – 5.17), being female (AOR=2.03, 95% CI: 1.6 – 5.17), being a married (AOR=1.80, 95%CI: 1.21 – 8.36) and being a Christian (AOR=2.50, 95%CI: 1.61 – 5.92) were significantly associated with adherence to HAART in HIV patients on HAART.
Conclusion: Spiritual health care used as complementary medicine alongside treatment of HIV/AIDS patients on Art will lead to ; significant decrease in patients’ anxiety, significant increase in satisfaction and adherence and increase in retention and viral load suppression.
Keywords: Spiritual Care; Impact; Adherence; Religion; Spirituality; HIV/AIDS
Introduction
Adherence is defined as “the extent to which a person’s behavior – taking medication following a diet, and/or executing lifestyle changes – corresponds with agreed recommendation from a healthcare provider”. Effective therapy with HAART requires a high level of sustained adherence, to suppress viral replication and improve immunological and clinical outcomes [1]. Furthermore the risk of HIV/AIDs transmission resistance to HAART therapy is reduced [2]. Other findings have revealed that a successful treatment outcome with HAART is only possible with near perfect or perfect adherence. A more recent study have revealed 95% adherence level as that required to sustain viral suppression [3].
Patients’ adherence to HAART have been proven to have a number of predictors such as patients variables (age, income, literacy level and social status), type of regimen (type, number of pills, complexity), disease characteristics (stage of HIV, symptoms, opportunistic infections), patient provider relationship (therapeutic relationship, open communication, satisfaction) and clinical setting (accessibility, adherence programme, environment) [4,5].
Amongst the different methods used in measuring adherence; medication refill, self-report using validated questionnaire, visual analogue scale (VAS) and a rating task for 30-day adherence, medication refill adherence was reported to be the strongest predictor of viral suppression [6] Electronic monitoring, therapeutic drug monitoring, directly observed therapy, hematologic monitoring and viral load determination are other methods used to measure adherence [7]. The most effective measure of adherence documented so far is pill counts. This measure is limited by cost and issues related to logistics [8,9]. The least tasking, but most widely used method is Self-report. It is less expensive and particularly suitable for developing countries such as Nigeria with very low per capita income [10] and corresponding low per capita health spending .Several studies conducted in different countries have reported non-adherence rates ranging from 50% to 80% [5-7]. In sub-Saharan Africa, adherence rate varies depending on time and location of studies. One of the studies conducted by Weiser et al, 2003 in Botswana found self-reported and provider assessment adherence rates of 54% and 56% respectively. Other studies reported 66% in Uganda [15] 22% in Cote D’ Ivoire [9] and 71% in South Africa [10].
HIV/AIDS according revelation from literature is the most life threatening disease with great impact on every sphere of life [11–12].Most persons with HIV/AIDS turn to attach equal importance to spiritual and physical dimensions of their health [13]. When patients are diagnosed with HIV/AIDS, challenges such as fear of dead, stigma, anxiety and sometimes depression increase their need for spiritual care adjuvant to physical care [14–18]. The World Health Organization has stressed the need for spiritual care for patients as central and not peripheral to health [19]. The National Health Service Education for Scotland thus defines spiritual care as “that care which recognizes and responds to the needs of the human spirit when faced with trauma, ill health or sadness and can include the need for meaning, for self-worth, to express oneself, for faith support, perhaps for rites or prayers or sacrament, or simply for a sensitive listener. Spiritual care begins with encouraging human contact in compassionate relationship, and moves in whatever direction need requires” [20]. Although many studies have been carried out to determine the predictors of adherence, very little has been done on the effect of spiritual intervention on adherence to HAART.
Materials and Methods
Research Design
This is an intervention (Experimental) study aimed at investigating the impact of spiritual health care on HIV/AIDS patients’ response to treatment. Two groups of HIV/AIDS patients with similar characteristics such as same hospitals, similar stage in HIV/AIDS progression receiving same treatment from the same staff, within the same 6 months study period and from the same health districts in Fako (Limbe and Buea Regional Hospital). Recruitment was based on patients who have been on ART Maximum 6 months before commencement of study .Two arms, The intervention arm (receiving spiritual health/nursing care in addition to standard HIV/AIDS treatment) and the control arm (Not receiving the spiritual nursing/health care, but standard treatment) and the outcome on intervention or non-intervention will be compared for both groups after the 6months study period. This is also a mixed study, with both quantitative and qualitative designs. A qualitative design was used to determine patient’s experience (Level of anxiety, Level of satisfaction), whereas the quantitative design was used to determine the: participants’ length of hospital stay; level of adherence, retention and viral load. The intervention involved the administration of spiritual health care (Researcher’s presence to carefully Listen to Patients’ concerns, creating a spiritually supportive environment, Sensitively respond to patients’ believe system, Prayer, meditation and Spiritual counseling) with subsequent observations .Interview of participants to evaluate and record participants’ health outcomes, and participants’ health record in the hospital served as methods of getting results of study. The study was also a comparative study given that the intervention and the control group were compared in terms of health outcomes and experiences. The impact was measured in the experiment by comparing the health outcomes of the control group and the intervention group at the end of the study.
Study Area
The study was carried out in Fako Division precisely Buea and Limbe
Buea is the headquarters of the South West Region of Cameroon. There are many ethnic groups in Buea including the, Bakossi, Bakweri (indigenes), Bamileke, Bafut, Balondu, Metta and Bayangi among others. Buea has a population of about 200.000 inhabitants and is located 15kms from the Atlantic Ocean, and 60 kilometres from Douala, the economic capital of Cameroon. Limbe is surrounded by Tiko , Buea , the mountain and the Sea . It is located 53 Km from Douala the Economic Capital of Cameroon and has a populationof about 72,106 .Buea, Loum,Nkongsamba,,Mundemba, and KoruptNational Parc .It has a population of about 400,000 people .Most of the population of these two cities ( Buea and Limbe ) are engaged in agriculture as the main economic activity. They all have two seasons: the dry season from October to March and the wet season from March to September. Almost all ethnic groups in Cameroon are represented in these cities, attracted by the fertile volcanic soil and the Cameroon Development Corporation, a giant agricultural corporation that seconds the state of Cameroon in employment.
Study Design
This is an Experimental study with a quantitative design .The participants (HIV/AIDS positively diagnosed individuals who met the inclusion and exclusion criteria ) were randomly assigned to the intervention ( HIV/AIDS Positive patients currently receiving treatment plus spiritual health care intervention ) and the control group ( Those diagnosed with HIV/ AIDS , receiving treatment , but no spiritual intervention ) . The cohort was studied prospectively for a period of 6 months (June 2019- December 2019) and quantitative variables (Adherence, Retention, Viral Load, Anxiety and Satisfaction) were compared for both groups.
Study Population
Target Population
The target population was ambulatory HIV/AIDS patients receiving treatment (HAART) at Buea and Limbe and HIV/AIDS treatment centres during the study period .Selection into the study was done only for those who met the inclusion and exclusion criteria.
Inclusion Criteria
a. All HIV/AIDS patients diagnosed with HIV/AID at most 6months before commencement of study who consent to the study (Thus only Participants diagnosed with HIVAIDS from January 2019 till June 2019 were selected).
Patients aged 21 years and above. Patients below 21 years. This is because according to the Cameroon code for the classification of adults, adulthood begins at the age of 21 years
b. Conscious and ambulatory participants who could communicate.
c. Participants who consented to the study.
Exclusion Criteria
a. Patients who chose to withdraw from the study after signing the consent form
b. Patients who were unconscious.
c. The mentally disabled patients.
Sample Size Determination When Comparing two Means
Given that the levels of Viral load suppression, Levels of satisfaction , Levels of adherence, retention and anxiety for both groups were compared, the formulae for determining the sample size cited in Pagano M. and Gauvreau K., (2000) for comparing two means was used, due to its larger value in the sample size calculation.
Thus the Formulae
Considering the desired significance value for this study to be 0.05, and a desired statistical power of 90%, the Zcrit value =1.96 and Zpwr value = 1.28. The assumed value of σ =7 and that for D= 1.296
Therefore, sample size
By use of the Population of patients receiving HAART in Buea, and Limbe , we proceeded in the recruitment of participants in the two Regional Hospitals as revealed in the Table 1 below.
Sampling Techniques
The sampling method that was used was the simple random sampling method. The sample size was estimated to be 230 (115 for the intervention and 115 participants for the control group) using the formulae for determining the sample size when comparing two means or groups. Participants were recruited by random assignment to either the intervention or the control group after meeting the inclusion and exclusion criteria and consenting to the study. Randomization was done by the research assistants by the use of Random draws made from the group of patients who turned up at the treatment centres on study days. Patients who did not meet the inclusion criteria were excluded from the study.
Study Procedure
Recruitment of Participants
Participants who met the inclusion criteria were recruited into the intervention and the control groups respectively.
Six research assistants were trained for two days on how to administer the questionnaire and on administration of spiritual care. On Tuesdays and Fridays which were our study days, they would turn up at the site at 9am, get a random list of patients who consented to the study after presenting the study and then begin recruitment randomly into the intervention and the control group respectively. Baseline data which includes demographic information and variables under study like viral load were noted. Phone numbers of Participants of both the intervention and the control arm were also taken for follow up of spiritual care through text messages (Only for intervention) and for self-reported clinical outcomes as treatment with HAART proceeded with or without spiritual care.
Random Allocation
In order to eliminate bias during the recruitment, a simple random sampling method was used. In this case a simple random table was designed in each session of the study by the research assistants following random draws and codes were attributed against each name. Odd number codes were assigned to the intervention arm and even number codes to the control arm.
A random table having serial numbers and their corresponding codes was produced.
Thus if first HIV/AIDS patient consented to the study, they were given a code from the random table corresponding to their serial number and assigned to the intervention. Furthermore the second participant recruited would be assigned a code corresponding to serial number 2 and allocated to the control group. This same pattern of allocation was respected throughout the study.
Primary Outcomes
a) Compliance (adherence)
Measurement of adherence
Adherence was assessed retrospectively based on a 4-day recall as used in Adult AIDS Clinical Trials Group (AACTG) follow up questionnaire [5] Adherence index will be calculated by the formula:
Patients with more than 95% of adherence were considered as having high adherence and those with less than 95% were considered as having low adherence.
Data Management
The data collected was entered into EPI Info version 3.5.4 software in an electronic data set, in a manner that can be accessed only by the investigator. Before this was done, the data collected was assessed for accuracy of the information and later saved in an email/memory card of the principal investigator as a back-up. Furthermore, during the study, the hard copies of the filled questionnaires were saved in a personal cupboard of the principal researcher to ensure confidentiality of information provided by the participants.
Statistical Analysis
Data was entered in Epi info version 3.5.4 and analysed using SPSS version 25. Univariate analysis was be used to describe the demographic characteristics of the participants. Tables of frequencies and proportions, bar charts and pie charts were used for descriptive statistics. In order to test the statistical significance, the t-test, Chi square test, multiple logistic regression, and one way ANOVA tests were performed.
The Impact of spiritual health care on patients’ adherence to treatment was determined by comparing the level of adherence of the intervention arm with that of the control arm:
Ethical Considerations
In order to ensure an ethically sound study, an ethic’s approval was sought and received from the Institutional review board (Ref-2018/872-10/UB/SG/IRB/FHS), Faculty of Health Sciences University of Buea. Furthermore an authorization to carry out the study was sought and received from the Faculty of Health Sciences University of Buea. An administrative approval was gotten from the Regional Delegate of Public Health for the South West Region. An authorization was also obtained from the; Regional Hospital –Buea, Regional Hospital Limbe and District Hospital Kumba.
Consent was sought from each patient before the study commenced and confidentiality was maintained in the study by the non-use of patient’s names but Identification codes. Furthermore, with respect to the principle of beneficence; the patients were informed about the benefits such as deriving comfort from spiritual care. Participants’ information were saved in a private place not accessible by any one. Non-maleficence was ensured by administering spiritual intervention while ensuring sensitivity to participants’ cultural differences, beliefs, values and religious differences.
Internal Validity
Bias was reduced by doing an experimental study , while ensuring that the intervention and control were conducted in the same hospital , with similar patients with similar clinical characteristics ( Ambulatory HIV/AIDS patients receiving treatment at the Buea and Limbe Regional Hospital respectively. Next by the use of the simple random sampling method, the event of a phenomenon occurring by chance was reduced. Internal validity was further ensured by using standardized instruments of measurement of the variables. The use of measurable objectives for the study ensured the validity as well.
Results
Flowchart of Participants in the Intervention
Figure 1 depicts the flow of participants in the study. We approached 230 HIV patients fulfilling the inclusion criteria and asked them to enroll for the study. Base on the probability proportion to size technique, we approached 134 participants from the Limbe Regional Hospital (LRH) and 96 participants from the Buea Regional Hospital (BRH) as shown in Table 2.
Of the 134 participants approached in the LRH, 8 (5.9%) declined to participate and of the 96 participants approached in the BRH, 2 (2.1%) participants also declined. The remaining participants who consented were randomly allocated to a control group and intervention group in a ratio of 1:1(in LRH, the intervention: control ratio was 63:63 and in the BRH, the intervention: control ratio was 47:47). Among the participants in the control and intervention groups, 10 (9.1%) were lost to follow-up. Hence, of the 230 enrolled or approached participants, 200 completed the study, thus the completion rate was 87.0%.
Socio-Demographic Characteristics Of Participants
Table 3 shows the socio-demographic characteristics of the participants in the control and intervention groups. The two groups were similar (p>0.05) in terms of socio-demographic characteristics such as age, gender, education, occupation, religion, income and marital status at baseline. The mean age of the participants was 29.6 (SD ± 3.65) years. Majority 154 (77.0%) of the participants were females. Ninety-two (46%) participants were holders of a first school leaving certificate. Majority of the participants were single and had an average monthly income of less than 100,000FCFA. Seventeen (8.5%) participants were Muslims by faith.
Baseline Characteristics On Adherence To Haart Among Hiv Patients
The proportion of participants adhering to HAART was 122 (61.0%) [95%CI: 54 – 68] (Figure 3).
The proportion of participants adhering to HAART was not significantly (p=0.528) different in the intervention and control groups. The proportion of participants adhering to HAART in the intervention group was 70 (70.0%) while that in the control group was 74 (74.0%). This difference did not reach statistical significance (Table 3).
Impact of Spiritual Health Intervention on Adherence to Haart Among Hiv Patients
Table 5 shows the changes in the adherence of HIV patients to HART after the spiritual health intervention in the control and intervention groups. The proportion of participants adhering to HAART increased significantly from baseline to post-intervention in the intervention group but not in the control group. The proportion of participants adhering to HAART increased significantly (p=0.030) from 70 (70.0%) at baseline to 83 (83.0%) at post-intervention in the intervention group. In the control group, the proportion of participants adhering to HAART increased from 74 (74.0%) at baseline to 75 (75.0%) post-intervention but this increase did not reach statistical significance (Figure 4).
Binary logistic regression model showed that the spiritual health intervention (AOR=3.11, 95%CI: 1.52 – 7.54), being at least 38 years old (AOR=2.15, 95% CI: 1.02 – 4.54), being a female (AOR=2.15, 95% CI: 1.6 – 5.17), being female (AOR=2.03, 95% CI: 1.6 – 5.17), being a married (AOR=1.80, 95%CI: 1.21 – 8.36) and being a Christian (AOR=2.50, 95%CI: 1.61 – 5.92) were significantly associated with adherence to ART in HIV patients on ART (Table 5).
Discussion
The Impact of Spiritual Health Intervention on Adherence OF HIV/AIDS Patients to HAART
Importance of adherence
Adherence may be defined as the extent to which a patient takes a medication in the way intended by a health care provider and it is expressed quantitatively as the percentage of doses that have been taken by the patients [21]. Adherence to treatment is a very important aspect of health protective behavior. Poor adherence to treatment is considered a critical barrier to treatment success and remains one of the major challenges facing the healthcare professions in Nigeria and beyond [22]. [23] Noted that good adherence to medication taking behavior forestalls the psychological, physical, social and economic consequences of HIV/AIDS. Hence it is necessary to carry out studies on adherence in order to achieve optimal health care for masses. The phenomenon of adherence is related to people’s knowledge and belief about illness, motivation to manage it, confidence in their ability to engage in illness-management behaviors and expectations regarding the outcome of treatment and consequences of poor adherence [24].
The Impact of Spiritual Intervention to Adherence to HAART
The results on the impact of spiritual health intervention on adherence to HAART reveals that, the proportion of participants adhering to ART increased significantly from baseline to post-intervention in the intervention group but not in the control group. The proportion of participants adhering to HAART increased significantly (p=0.030) from 70 (70.0%) at baseline to 83 (83.0%) at post-intervention in the intervention group. In the control group, the proportion of participants adhering to HAART increased from 74 (74.0%) at baseline to 75 (75.0%) post-intervention but this increase did not reach statistical significance (Figure 9).
Implication of Spiritual Intervention to Treatment and Control of HIV/AIDs
This result suggests that HIV/AIDS patients receiving spiritual health care adjuvant to HAART are far more likely to adhere to treatment than those who receive only HAART as treatment. This result is consistent to that conducted by [25], in which 18 perinatal infected youth that measured religious beliefs and practices of these youths, found that participants who had excellent adherence had significantly higher religious beliefs scores and greater religious practice scores than those who had poor adherence. A contrary study by [24] revealed that high religiosity was negatively associated with ART adherence (Published by European Centre for Research Training and Development UK).
Studies conducted in Uganda have also reported mixed findings. [26] in a study that measured religiosity in terms of frequency of attendance at religious services found that high religious belief was associated with high levels of adherence to anti-retroviral therapy. But in a more recent in-depth interviews conducted with 39 very religious people living with HIV (16 had and 23 had never discontinued antiretroviral therapy) to assess the role of religion in their treatment decisions and in coping with HIV, [26] found that participants who had discontinued HAART gave reasons such as: teachings and prophecies from religious leaders and supporting Biblical scriptures All of which led them to feel that God, their faith and testimonies by their already healed peers who had stopped HAART would help them According to [25] participants who had never discontinued HAART gave reasons such as continuous adherence counseling from multiple sources, improvement in physical health as a result of HAART, belief that God heals in different ways and that non-adherence is equal to putting God to a test. They found that high religiosity was reported to help participants cope with HIV through engagement in personal and or community protective behaviors, taking care of other illness and reducing worries.
There is also, evidence that women living with HIV face different barriers to adherence.
Conclusion
Our Results on participants’ adherence revealed that, the proportion of participants adhering to HAART increased significantly from baseline to post-intervention in the intervention group but not in the control group. The proportion of participants adhering to HAART increased significantly (p=0.030) from 70 (70.0%) at baseline to 83 (83.0%) at post-intervention in the intervention group. Whereas the control had non statistically increase in adherence (Figure 9).This result provides evidence that administration of spiritual care as complementary therapy to ART will significantly increase HIVAIDS patients’ adherence to HAART and therefore increase viral suppression and general clinical outcomes.
Recommendations
We recommend that the state and ministry of public health should modify health policies to promote the provision of chaplaincy services and a prayer chapel in every hospital, so as to make available room for spiritual Health care provision.
HIV/AIDS patients taking treatment should be educated on the place of spiritual intervention in promoting hope and adherence and those who agree to be ministered to be enrolled in a spiritual intervention program.
Medical nursing and public health education should have spiritual care incorporated by the ministry of Higher education and public health, so as to adequately provide spiritual care as an integral part of holistic care.
Acknowledgements
We wish to acknowledge the Patients of Limbe and Buea Regional Hospitals for participating in the research.
Conflict of Interest
There is no conflict of interest in connection to this topic.
- Mueller PS, Plevak DJ, Rummans TA (2001) Religious involvement, spirituality, and medicine: implications for clinical practice. Mayo Clin Proc. 76: 1225–35.
- Cotton S, Puchalski CM, Sherman SN, Mrus JM, Peterman AH, Feinberg J, et al. (2006) Spirituality and religion in patients with HIV/AIDS. J Gen Intern Med. 21: S5–13.
- Dalmida SG, Koenig HG, Holstad MM, Wirani MM (2013) The psychological well-being of people living with HIV/AIDS and the role of religious coping and social support. Int J Psychiatry Med Garner RC (2000) Safe sects? Dynamic religion and AIDS in South Africa. J Mod Afr Stud. 38: 41–69
- Hamilton JB, Moore AD, Johnson KA, Koenig HG (2013) Reading the Bible for guidance, comfort, and strength during stressful life events. Nurs Res. 62: 178–84
- Kremer H, Ironson G (2009) Everything changed: spiritual transformation in people with HIV. Int J Psychiatry Med. 39: 243–62
- WHO (2007) Faith-based organizations play a major role in HIV/AIDS care and treatment in sub-Saharan Africa.
- NHS Education for Scotland-Mersey Care (2009) Spiritual Care Matters: An Introductory Resource for all NHS Scotland Staff.
- Sovran S (2013) Understanding culture and HIV/AIDS in sub-Saharan Africa. SAHARA J. 10: 32–41.
- Mkandawire-Valhmu L, Kako PM, Kibicho JW (2012) Perceptions of the character of God as narrated by East African women living with HIV. J Christ Nurs. 29: 164–72
- Rankin SH, Lindgren T, Rankin WW, Ng'Oma J (2005) Donkey work: women, religion, and HIV/AIDS in Malawi. Health Care Women Int. 26: 4–16.
- Steglitz J, Ng R, Mosha JS, Kershaw T (2012) Divinity and distress: the impact of religion and spirituality on the mental health of HIV-positive adults in Tanzania. AIDS Behav. 16: 2392–8.
- Szaflarski M (2013) Spirituality and religion among HIV-infected individuals. Curr HIV/AIDS Rep. 10: 324–32
- Tarakeshwar N, Vanderwerker LC, Paulk E, Pearce MJ, Kasl SV, Prigerson HG (2006) Religious coping is associated with the quality of life of patients with advanced cancer. J Palliat Med. 9: 646–57.
- Aldridge D (1991) Spirituality, healing and medicine. Br J Gen Pract. 41: 425–7.
- Coleman CL, Eller LS, Nokes KM, Bunch E, Reynolds NR, et al. (2006) Prayer as a complementary health strategy for managing HIV-related symptoms among ethnically diverse patients. Holist Nurs Pract. 20: 65–72
- Kulis S, Hodge DR, Ayers SL, Brown EF, Marsiglia FF (2012) Spirituality and religion: intertwined protective factors for substance use among urban American Indian youth. Am J Drug Alcohol Abuse. 38: 444–9
- Tarakeshwar N, Khan N, Sikkema KJ (2006) A relationship-based framework of spirituality for individuals with HIV. AIDS Behav. 10: 59–70
- Kremer H, Ironson G (2009) Everything changed: spiritual transformation in people with HIV. Int J Psychiatry Med. 39: 243–62.
- Ironson G, Solomon GF, Balbin EG, O'Cleirigh C, George A, Kumar M, et al. (2002) The Ironson-woods Spirituality/Religiousness Index is associated with long survival, health behaviors, less distress, and low cortisol in people with HIV/AIDS. Ann Behav Med. 24: 34–48.
- Odumosu O, Mahal A, Canning D, Okonkwo P (2006) The impact HIV/AIDS on Nigerians house-holds. In: Adeya O, Kanki PJ, Odutolu O, Idoko J. A. AIDS in Nigeria: A nation on the threshold. Cambridge MA (USA): Harvard University Press; 193-212.
- Kirkland EC (2001) Norms affecting HIV: Self disclosure in men and women. Journal of Consulting and Clinical Psychology, 23: 94–120.
- Renhard PM (2007) Good medication taking behavior and consequences of HIV/AIDS on man. Bulletin of AIDS, 7: 2000-6.
- World Health Organization (2003) Stigma, HIV/AIDS and prevention of mother-to-child Transmission in Nigeria. Evolution and Program Planning, 25: 347-56.
- Tumwine C, Neema S, Wagner G (2012) Reasons Why High Religiosity Can Co-exist with and Precipitate Discontinuation of Anti-Retroviral Therapy Among Different HIV Clinets in Uganada.
FIGURE 1
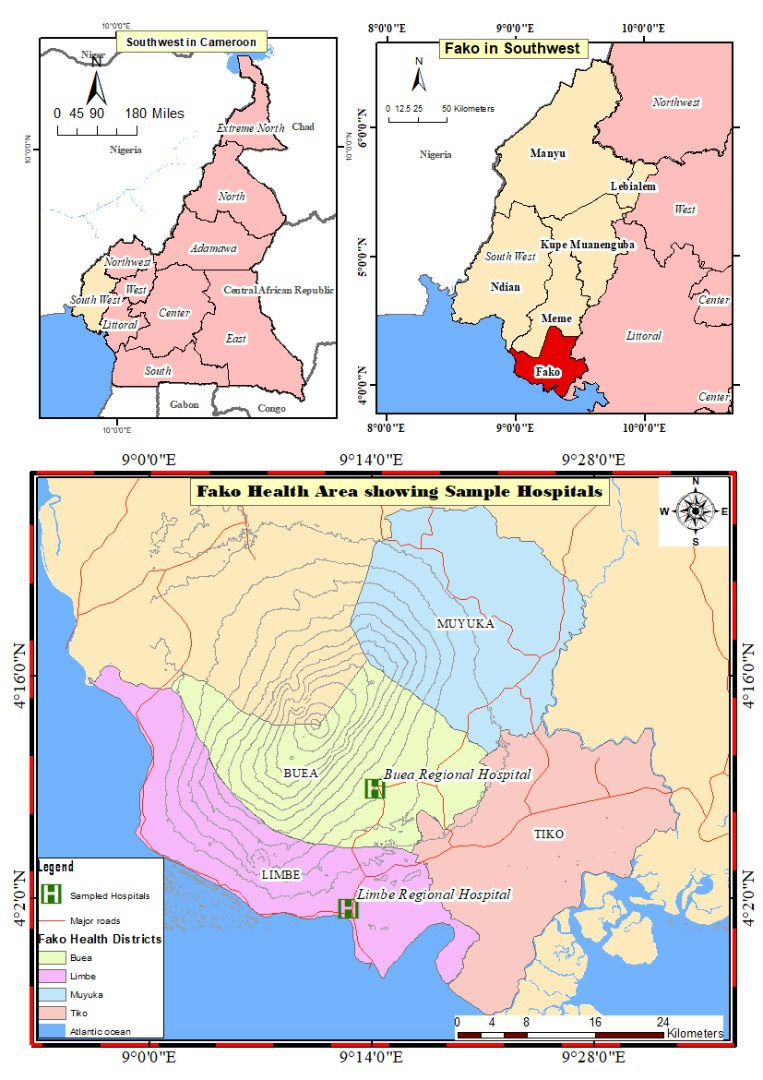
Figure 1: The Map of Study Area (Buea and Limbe) - Fako –Division South West Region
Where σ is the assumed standard deviation of each group (assumed to be equal for both groups)
Zcrit Value is the standard normal deviate for the desired significance level (1.96, corresponding to a significant value of 0.05)
Zpwr value is the standard normal deviate for the desired statistical power (0.34 or 1.28, are typically used corresponding to a power of 80% 0r 90% respectively)
And D is the minimum expected difference between the two means.
FIGURE 2
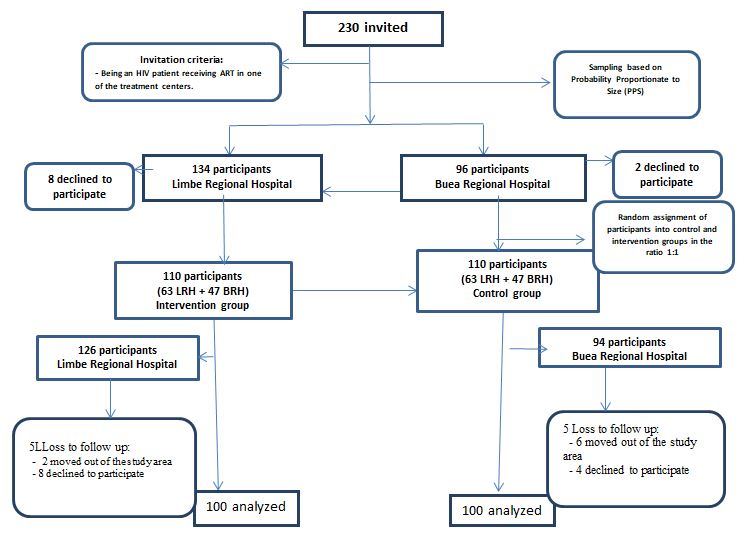
Figure 2: Flowchart for the Recruitment of HIV Patients
FIGURE 3
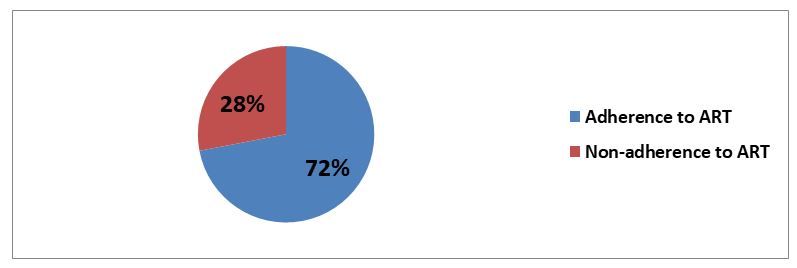
Figure 3: Proportion of participants adhering to HAART
FIGURE 4
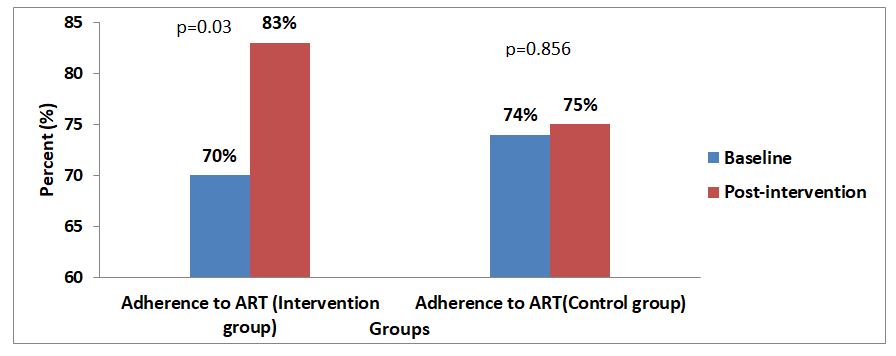
Figure 4: Impact of spiritual health on adherence to HAART among HIV patients in the control and intervention groups
Tables at a glance
Figures at a glance