Towards Sustainable TB Control: Political Economy of Domestic Financing in Osun State, Nigeria
Received Date: November 25, 2025 Accepted Date: December 06, 2025 Published Date: December 10, 2025
doi:10.17303/jaid.2025.12.202
Citation: Timothy Akinmurele, Niyi Taiwo, Akin Oyebade, Adeniyi Adebayo (2025) Towards Sustainable HIV Care Financing: A Stakeholder Analysis of Health Insurance Integration in Nigeria. J HIV AIDS Infect Dis 12: 1-15
Abstract
Background: Tuberculosis (TB) is a deadly disease of major public health concern in Nigeria. However, TB control is grossly underfunded with an estimated financing gap of over 70%. To address this, the Domestic Mobilisation of Resources (DRM) is required for the equitable and sustainable financing of TB interventions. This paper reports the outcome of a DRM project that utilised a political economy framework to facilitate increased TB financing in Osun State, Nigeria.
Methods: The authors reviewed government documents, fiscal budgets, and annual budget performance reports to generate fiscal data for analysis. They also reviewed relevant literature to situate, compare and explain intervention outcomes. A 6-element political economy framework, consisting of leadership politics, bureaucratic politics, budget politics, interest group politics, external actor politics and beneficiary politics, was adopted on the project to drive reforms in TB financing.
Key Results: The project enhanced interministerial collaboration between Health, Finance, Budget, and Economic Planning ministries, improved budget transparency and reduced perceived opacity in health financing. This resulted in an 82% cumulative increase in the annual health budget from N9.85 billion in 2020 to N17.98 billion in 2023. The TB control budget also increased cumulatively by over 800% (N5 million in 2021 to N50 million in 2023). The number of health facilities accredited to provide TB services on the Osun State Health Insurance Scheme increased from 31 to over 170 within the first years of the project.
Conclusions: The study outcomes can inform strategies and policies in similar settings to mobilize domestic resources to control infectious and non-communicable diseases.
Keywords: Tuberculosis (Tb); Health Financing; Domestic Resource Mobilisation (Drm); Political Economy; Political Economy Framework; Social Health Insurance
Introduction
Domestic resource mobilisation (DRM) is currently on the front burner in global discourse around sustainable health financing in low and middle-income countries (LMICs) [5] DRM is crucial for mobilising funds to address financing gaps for the SDGs and other social interventions [1]. The success of DRM interventions is crucial; thus, identifying and understanding the political contexts, historical legacies, and the intricate relationships between various actors is important [2, 3]. There is a dire need to increase equitable and sustainable financing for TB interventions in Nigeria through DRM [4, 5]. The National TB Strategic Plan (2021 – 2025) emphasises the promotion of DRM to bridge the financing gap for TB control in Nigeria through increasing public sector spending, expanding the coverage of the social health insurance schemes and leveraging private sector resources (FMOH, 2021).
Tuberculosis (TB) remains a global epidemic of major public health concern requiring substantial resources for control and elimination. The number of TB cases and deaths remains alarmingly high, with Nigeria and 7 other countries accounting for over 68% of global TB cases. Nigeria has an estimated TB burden of 467,000 and 125,000 TB deaths, and it faces significant financial constraints in tackling the disease [6]. The United Nations High-Level Meeting (UNHLM) on ending TB in 2018 set an ambitious target of increasing the global annual TB investment to 13 billion USD by 2022. However, only 5.3 and 5.4 billion USD were released to fight TB globally in 2020 and 2021 respectively [7].
In Nigeria, TB control is largely funded by international donors with poor support from the Government, resulting in a wide funding gap (Figure 1). In 2021, only 30% of the 375 million USD TB control budget was funded, and over 80% of the funds came from international donors [6]. This funding gap exposes TB patients and their households to catastrophic expenditures and restricts access, undermining National and State TB programs and TB control efforts [6].
Osun State, with a population of over five million residents [8], faces challenges in TB control and securing adequate funding for TB control. A review of the health spending and budgeting pattern of the State (2013 – 2017) showed suboptimal performance compared to global health financing benchmarks (Table 1) [9].
There is a dire need to increase equitable and sustainable financing for TB interventions in Nigeria through DRM [4, 5]. The National TB Strategic Plan (2021 – 2025) emphasizes the promotion of DRM to bridge the financing gap for TB control in Nigeria through increasing public sector spending, expanding the coverage of the social health insurance schemes and leveraging private sector resources (FMOH, 2021). Planning and implementing DRM interventions is an inherently political process that may require the application of the political economy framework.
This study examines the impact of applying a political economy framework to mobilise domestic resources for TB control from government and non-government sources in Osun State, Southwest Nigeria. The 6-element framework, adopted from [10], consists of leadership politics, bureaucratic politics, budget politics, interest group politics, external actor politics and beneficiary politics. The framework was used to analyse the power, position, interest, and influence of various stakeholders including politicians, bureaucrats, leaders, interest groups, budget decision-makers, external actors and beneficiaries on the mobilization of resources for TB control in the State [10-14]. This approach has been successfully applied in several countries, including Malaysia, Mexico, South Africa and Turkey, to introduce reforms into their healthcare financing systems [13, 15]. This paper thus reflects the outcomes and impact of a DRM project that applied a political economy framework to generate sustainable financing for TB control in Nigeria.
With funding from the DRM component of a USAID Tuberculosis Local Organization Network (TB-LON) Project, the authors implemented this project to facilitate increased funding for TB control and elimination via domestic resources in Osun State between 2020 and 2023 [10]. The USAID TB LON Project is focused on complementing and accelerating the ongoing activities being implemented by the GoN and its partners to reduce the TB burden in Nigeria.
Literature Review
Tuberculosis (TB) remains a global epidemic and a major public health concern, requiring substantial resources for effective control and elimination. According to the 2022 Global TB Report, the number of TB cases and deaths remains alarmingly high, particularly in the eight high TB burden countries, including Nigeria, China, India, Pakistan, the Philippines, Bangladesh, Indonesia and the Democratic Republic of Congo (DRC), which account for over 68% of global TB cases. Globally, about 10.6 million people were estimated to have fallen ill with TB in 2021, but only 6.4 million TB cases were diagnosed [6].
Nigeria, one of eight countries with the highest TB burden globally, faces significant constraints in tackling the disease. The 2021 estimated TB burden in Nigeria was 467,000, but only 204,725 new TB cases were reported, representing a significant gap (43.8%) between estimated and reported cases. Also in 2021, about 125,000 people died from TB (one person every 4 minutes) with an estimated case-fatality ratio of 28% [6] Multidrug-resistant/Rifampicin Resistant (MDR/RR) TB remains a huge problem in Nigeria, with about 80% of estimated cases going undetected and untreated [6].
In 2018, during the first-ever United Nations High-Level Meeting (UNHLM) on ending TB, several Heads of State, including the Nigerian President, made powerful political declarations and committed to ambitious targets to eliminate TB [7]. The UN HLM set a target of increasing the global annual investment in TB to 13 billion US Dollars (USD) by 2022; however, only 5.3 and 5.4 billion USD were released to fight TB globally in 2020 and 2021, respectively (see Figure 1).
DRM is getting increasingly popular as a means of bridging critical funding gaps, influencing government spending and promoting national ownership to improve health and social outcomes [4, 5]. DRM aims to establish a sustainable framework for financing healthcare, and it entails the various means of generating, allocating, and utilizing financial resources for health interventions [5]. The National TB Strategic Plan (2015 – 2020) emphasizes the promotion of DRM as a sustainable financing mechanism for expanding TB control interventions in Nigeria. The current strategic plan for sustainable financing of TB prevention, care and treatment in Nigeria highlights these major sources: increasing public sector spending for health by increasing fiscal space; expanding the coverage of the social health insurance schemes; and leveraging private sector resources.
Achieving these sustainable DRM goals for effective TB control interventions is an inherently political process that requires the application of the political economy framework for the health financing reform approach proposed by [10]. Thus, understanding political economy and the application of political economy analysis is important for the successful management of health financing reforms. To successfully address the politics of health financing policy implementation, policymakers and development partners need to leverage political economy analysis to assess the power, position, interest and influence of various stakeholders including politicians, bureaucrats, leaders, interest groups, budget decision-makers, external actors and beneficiaries [14, 12].
Political economy analysis can help policymakers construct strategic responses and deploy appropriate policy sequencing approaches in implementing healthcare financing reforms [10-13]. Several countries, including Malaysia, Mexico, South Africa and Turkey, have successfully applied this approach to the implementation of reforms in their healthcare financing systems [13, 15].
This paper explores the application of the political economy framework in implementing DRM intervention to generate sustainable financing for TB control in Osun State, Southwest Nigeria. The project was implemented between November 2020 and March 2023.
Methodology
Design and Data Sources
To have a comprehensive understanding of the factors influencing the DRM for TB control in Osun State, the authors employed a multifaceted research approach that entailed a review of relevant academic literature, government policies and budgets as well as the analysis of fiscal data. The research team reviewed pertinent academic literature, academic papers and reports related to TB control, healthcare financing, and political economy. This review informed the study background and the adopted theoretical framework, and it provided context for interpreting and explaining the project outcome and impact. The State fiscal budget, relevant policies, and annual budget performance reports were analysed to generate the fiscal data reported. This analysed data provided an understanding of historical and current funding patterns for TB control in the states and informed the political economy analysis, especially the influence of stakeholders on the allocation of government resources for TB control.
The political economy analysis provides critical context and understanding for navigating the complex political and economic landscape within which DRM for TB control could be achieved. It helps policymakers develop effective strategies to address existential political challenges in implementing health insurance schemes [10, 16, 17]. Thus, the outcomes of this study will provide policymakers, funders, and other stakeholders with valuable insights for designing and implementing effective DRM interventions for the sustainable financing of TB elimination programs in Nigeria and other LMICs.
Implementation Steps
A four-step strategic implementation process was developed for this intervention:
Application of Political Economy Framework
Working with the State TB and Leprosy Control Program and the Osun State Health Insurance Agency (OSHIA), the project team conducted a comprehensive stakeholder analysis to identify, understand and prioritise people and groups who can influence health financing in Osun State (Table 2). The outcome of the stakeholder analysis was applied to the adopted political economy framework [10] and the identified stakeholders were categorised into six groups: leadership politics, bureaucratic politics, budget politics, interest group politics, external actor politics and beneficiary politics [10]. The categories were used to analyse the political economy dimensions of DRM for TB control in the State (Table 3).
This process enabled the team to assess and determine the roles and positions of various stakeholders. It also provided an understanding of the power dynamics between the politicians, policymakers, other stakeholders, and the institutions they represent and their influence on the mobilisation of resources for TB control in Osun State. This informed the design of strategic interventions and the development of tailor-made infographic advocacy tools, policy briefs and funding proposals for various private sector stakeholders.
Advocacy Meetings with Politicians and High-Level Policy Makers
A high-level advocacy meeting was held with politicians, policymakers, and other stakeholders at the project inception for their buy-in and commitment. This advocacy meeting was conducted with customised advocacy tools and presentations. The project team and members of the TWG conducted follow-up advocacy visits as needed on the project to the following stakeholders Honourable Commissioners and Permanent Secretaries of the Ministries of Finance, Economic Planning and Budget; Chairman, State House of Assembly Committee on Health; Chairman and Executive Secretaries of the Primary Health Care Development Board, Osun State Health Insurance Agency and Osun State Agency for the Control of AIDS; State Accountant General; relevant Directors from the Ministries of Finance and Economic Planning and Budget. The follow-up visits were conducted to reinforce their commitment, address concerns, provide updates, gain feedback, strengthen the relationship, identify opportunities and maximise project impact and sustainability.
Set up Osun State TB DRM Technical Working Group (TB DRM TWG)
The political economy analysis informed the setting up of a 17-member TB DRM TWG (Table IV) that provided a unique platform for effective communication between the Ministry of Health (MoH) and the finance and budget Ministries, Departments and Agencies (MDAs) in the state. The TWG promoted effective communication, reduced the information gap and solidified the relationship between the Ministry of Health and the finance and budget MDAs in the state. It also ensured transparency and prioritisation of the Health and TB budget on the State annual appropriation laws; effective tracking of the state annual budgeting preparation process for increased budget allocations for TB control interventions; active tracking of Memos, requests and disbursement of budgeted funds for TB services; and tracking the expenditure of the released funds for TB control in Osun State. See Table 3 for the TWG membership and the category/dimension they were selected from. The project also built the capacity of the TWG members and other relevant staff from the MoH on public finance management, public sector accounting, memo writing, advocacy, developing investment cases for private sector engagement (proposal writing) and budgeting. The TWG engaged in continuous high-level advocacy for improved funding for health, particularly TB, through a series of problem-focused and action-oriented meetings with relevant policymakers and private sector operators.
Table IV summarises the application of the political economy framework in analysing key structural and institutional factors, as well as the strategic actions employed to engage each dimension. This approach highlights how power relations, stakeholder interests, and governance structures shape policy implementation and influence the sustainability of TB financing reforms.
5-Year Road Map for Integrating TB Services into State Health Insurance Scheme (SHIS) Benefit Package
Integrating TB services into the benefit package of the SHIS represents an important milestone toward sustainable TB financing and Universal Health Coverage (UHC), elimination of user fees for improved access to TB services, protection from catastrophic health expenditures, ensuring the provision of high-quality TB services and improved TB outcomes (Regan et al., 2021).
The integration roadmap developed involves a six-step integration process (Figure II). The steps entail: Conducting a pure risk cost estimate (Actuarial Study) for TB coverage and inclusion of TB services on the benefits package of OHIS; Systematic accreditation and empanelment of all accredited public and private health facilities providing TB Services as a service provider on OHIS; Facilitating drive towards accelerated enrolment of informal sector workers and TB patients in OHIS; Facilitation of intersectoral and interagency collaborations for TB awareness activities in the state; Leveraging on funds from government and donor agencies for community TB services; and Leveraging on funds from government and donor agencies for the management of drug-resistant TB cases.
An implementation framework was also developed to guide and streamline the implementation of the six-step integration process, as depicted in Figure III below. The framework identifies the relevant stakeholders and highlights their roles and responsibilities in providing high-quality TB services as part of the state health insurance benefit package. The stakeholders essential for the success of the integration efforts (as identified in the framework) include the OHIS, TB Service Providers (healthcare facilities), Osun State Ministry of Health, Osun State TB and Leprosy Control Program, Donor Agencies, Implementing Partners, and other relevant Ministries, Departments and Agencies (MDAs).
Key Results and Discussion
The capacity building, monthly meetings and sustained high-level advocacy activities ensured a clear understanding of the state government budget preparation and approval process and protocols by the MoH, reduced the information gap and addressed perceived opacity in health budgets by the budget and finance MDAs. Through this strengthened communication and improved budgeting activities, the MoH recorded an increase in annual health budget from N9, 849, 596, 550.00 in 2020 to N14, 753, 941, 570.00 in 2021, N14, 592, 662, 630.00 in 2022 and N17, 917, 530.00 in 2023. Specifically, TB control budget also increased from N5, 000, 000.00 in 2021 to N47, 784, 500.00 in 2022 and over N50, 000, 000.00 in 2023 (Fig. 4). The zero-release of funds for TB control over the past 15 years was reversed with the release of funds from the State Government to upgrade the GeneXpert Lab in the State Hospital to Biosafety Level-2 (BSL-2) capacity.
An advocacy visit conducted to the Executive Governor of the State in August 2021 resulted in the State's commitment to procure two additional GeneXpert machines for TB diagnosis in the State. The private sector engagement drive led to the successful mobilisation of additional resources for TB control from NGOs and community groups for the renovation and equipping of three TB laboratories at Boripe, Isokan and Iwo LGAs.
Several countries, including Mexico, Nicaragua, Turkey and Uganda, have successfully increased DRM via the application of political economy analysis at different stages of their health financing reforms (18; 4; 10). In Uganda, political and economic factors impacted domestic revenue generation and spending priorities positively, with the government focusing on expanding domestic revenue mobilization and becoming less dependent on foreign aid [4].
The project successfully conducted an actuarial study, which provided the pure risk cost estimate for TB coverage under the OHIS. The outcome of this actuarial analysis, a critical step in the integration process, revealed the financial implications and feasibility of integrating TB services into the benefit package of OHIS. The number of health facilities accredited to provide TB services and dually empanelled as service providers on OHIS (vital for successful integration) increased from 31 to over 170. Enrolment of informal sector workers and vulnerable populations (including TB patients) in the health insurance scheme is crucial for UHC. Over 2,000 TB patients (from zero in 2021) were enrolled, as part of the over 70, 000 vulnerable population, on OHIS.
Other countries have documented successful applications of political economy analysis in shaping policy trajectories to drive health financing reforms and the introduction of health insurance schemes (20; 17; 10). A review of the political economy of enrolment in community health insurance schemes in Ethiopia suggested that regions demonstrating high levels of state power and political will are more likely to achieve greater success [19, 20].
This project encountered some challenges, significantly the re-election bid loss by the incumbent Governor to the opposition party in 2022 led to changes in the political structure of the state and stalled the procurement of the two GeneXpert machines.
Limitations
We acknowledge some limitations of this study, including the non-generalizability of findings to other settings with different political, economic, and healthcare systems from Nigeria. Secondly, this study only establishes correlations between the interventions and outcome/results because causation in a complex social and political environment can be challenging. Finally, other factors beyond the control of the project and thus not accounted for may have influenced the project outcomes.
Enablers/Constraints
Targeted high-level advocacy meetings and follow-up visits, strong inter-ministerial communication between health and budget/finance MDAs and involvement of multi-sectoral stakeholders contributed to the increase in government funding for TB control. Strategic private sector engagement yielded additional resources for renovating and equipping TB Labs and multi-sectoral collaborations to develop a TB integration roadmap that initiated a process for integrating TB services into the benefit package of the state health insurance scheme in Osun state.
A major constraint encountered in the project was the dwindling state revenue and economic downturn within the State’s economy. This reduction in Government revenue, compounded by competing demand from other critical sectors, significantly exacerbated the difficulty in increasing budget allocation and expenditure for the health sector and TB control activities. The prolonged bureaucratic procedure and bottlenecks encountered from memo generation to approval and release of funds hindered the execution of several TB control programs, this explains the historically poor budget performance of the Ministry of Health. (Table 1). The worsening economic indices also adversely affected private sector organisations' capacity to support TB control programs. The existing high level of poverty - worsened by declining macro and micro-economic indices, rising inflationary trends and cost of living -made it difficult to enrol informal sector workers on OHIS (Barasa et al., 2021; Chuma et al., 2013; Lagomarsino et al., 2012).
Conclusion
The outcome of this DRM intervention in Nigeria highlights the critical role the political economy plays in forging a path towards improved DRM from government and non-government sources for the realization of ambitious funding targets set during the UNHLM on ending TB. The same approach can be applied to successfully mobilize resources for healthcare interventions or social development projects in other resource-constrained settings like Nigeria, which heavily depends on unsustainable foreign aid to fund these interventions.
- Bolch KB, Ceriani L, López-Calva LF (2022) The arithmetics and politics of domestic resource mobilization for poverty eradication. World Development. 149: 105691.
- Hujo K, Bangura Y (2020) The politics of domestic resource mobilization for social development: An introduction. The politics of domestic resource mobilization for social development. 1-37.
- Hujo K (2020) The Politics of Domestic Resource Mobilization for Social Development: Conclusions. The politics of domestic resource mobilization for social development. 405-22.
- Kjær AM, Ulriksen MS, Kangave J, Katusiimeh M (2017) A Political Economy Analysis of Domestic Resource Mobilization in Uganda.
- USAID (2023) Domestic Resource Mobilization (DRM). United States Agency for International Development. Retrieved 4th August 2023 from https://www.f pfinancingroadmap.org/learning-/specifictopics/domestic-resource-mobilization
- WHO (2022) Global Tuberculosis Report 2022 (Global TB Report, Issue). https://www.who.int/te ams/globaltuberculosis-programme/tb-repor-ts/global-tuberculosis-report-2022
- UN (2018) Political Declaration of UN General Assembly High Level Meeting on the Fight Against TB. WHO.
- Igwenagu E (2021, July 14, 2021) Nigerian Informer - Osun State Population 2022. Nigerian Informer. Retrieved 3rd November 2022 from https://nigerianinformer.com/os un-state-population/
- Adenekan A, Ekpenyong J, Carlson A, Sine J, Ilika F (2020) Health Financing Landscape: Osun State. Retrieved 16th August 2023, from http://www.healthpolicyplus.com/ ns/pubs/17404-17728_OsunHFL.pdf
- Sparkes SP, Bump JB, Özçelik EA, Kutzin J, Reich MR (2019) Political economy analysis for health financing reform. Health Systems & Reform. 5: 183-94.
- Breyer F, Schneider F (1992) Political economy of hospital financing. Health Economics Worldwide. 267-285.
- Campos PA, Reich MR (2019) Political analysis for health policy implementation. Health Systems & Reform. 5: 224-35.
- Croke K, Mohd Yusoff MB, Abdullah Z, Mohd Hanafiah AN, Mokhtaruddin K, et al. (2019) The political economy of health financing reform in Malaysia. Health Policy and Planning. 34: 732-9.
- Moreno Ternero JD, Roemer JE (2010) The political economy of health care finance.
- Gilson L (2019) Reflections from South Africa on the Value and Application of a Political Economy Lens for Health Financing Reform [Article]. Health Systems & Reform, 5: 236-43.
- Kelkar S, Kelkar S (2021) Health Insurance, National Health Protection Scheme, Public—Private Partnership. India’s Private Health Care Delivery: Critique and Remedies: 275-332.
- Novignon J, Lanko C, Arthur E (2021) Political economy and the pursuit of universal health coverage in Ghana: a case study of the National Health Insurance Scheme. Health Policy & Planning. 36: 14-21.
- Carrión G (2020) The Political Economy of Domestic Resource Mobilization in Nicaragua: Changing State-Citizen Relations and Social Development. Springer.
- Lavers T (2019) Towards Universal Health Coverage in Ethiopia's ‘developmental state’? The political drivers of health insurance. Social Science & Medicine. 228: 60-7.
- Lavers T (2020) The political economy of health insurance enrolment in Ethiopia: Party, state and the quest for universal health coverage.
- UN (2015) Addis Ababa Action Agenda of the third international conference on financing for development. United Nations Department of Economic and Social Affairs. 2: 37.
FIGURE 1
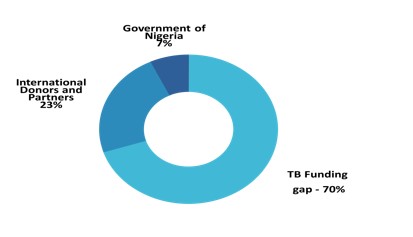
Figure 1: 2021 TB Funding Gap in Nigeria Showing TB Funding Gap of over 70%
FIGURE 2

Figure II: Six-Step TB Services Integration Process
FIGURE 3
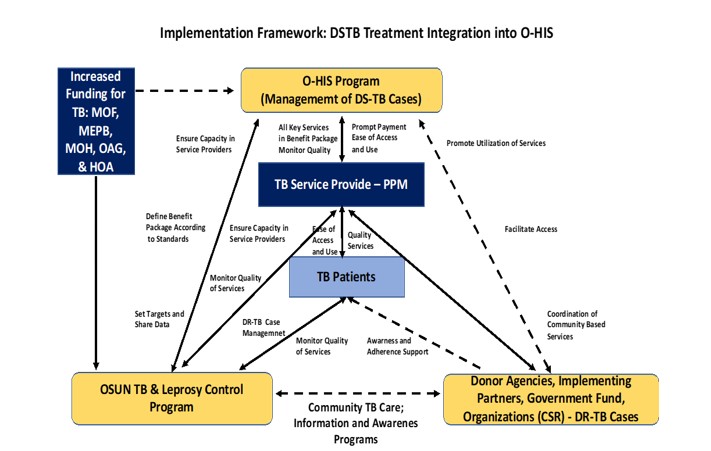
Figure III: Framework for Integrating TB Services into the OHIS for Sustainability
FIGURE 4
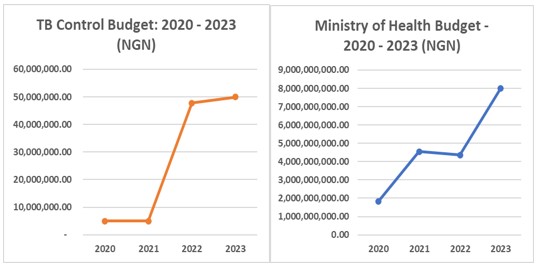
Figure IV: Ministry of Health and TB Budget Trend in Osun State 2020 - 2023
Tables at a glance
Figures at a glance