Prevalence and Determinants of Adherence to Highly Active Antiretroviral Therapy (HAART) amongst a Cohort of HIV Positive Women Accessing Treatment in a Tertiary Health Facility in Southern Nigeria
Received Date: October 22, 2013 Accepted Date: December 21, 2013 Published Date: December 23, 2013
doi: 10.17303/jaid.2013.2.102
Citation: Oku AO, et al. (2013) Prevalence and Determinants of Adherence to Highly Active Antiretroviral Therapy (HAART) amongst a Cohort of HIV Positive Women Accessing Treatment in a Tertiary Health Facility in Southern Nigeria. J HIV AIDS Infect Dis 1: 1-8.
Abstract
Background: Optimal adherence to HAART amongst women living with HIV/AIDS (WLHIV) accounts for more than half of all new infections worldwide. This is particularly crucial for the success of HIV/AIDS treatment programs. In Nigeria, adherence amongst women has remained largely unexplored. This study aims to determine the prevalence and determinants of adherence to HAART amongst HIV positive non-pregnant women receiving treatment in a tertiary health facility in Cross River State, Nigeria.
Method: A cross-sectional study was conducted amongst non-pregnant HIV positive women on HAART attending the Special treatment clinic of the University of Calabar Teaching Hospital between December 2012-Feburary 2013. A consecutive sample of 282 eligible WLHIV was enrolled into the study. A semi-structured interviewer-administered questionnaire was used to elicit information on self-reported adherence from the respondents. Adherence was defined as the consistent use of at least 95% of prescribed doses the week preceding the study. Summarization of data was done using frequencies/ proportions while exploration of categorical variables was performed using the chi square test. Independent predictors of adherence to HAART were determined by binary logistic regression and significance level was set at p<0.05.
Results: The mean age of WLHIV was 33.6 ± 8.5 years. The overall self-reported adherence rate in this study was 59.6%. Being busy, forgetting to take medications, felt depressed, and inconvenient timing were the main reasons cited by respondents for skipping doses. The independent risk factors for adherence to HAART included: nonpayment for ART services [OR 2.30; 95% CI: 1.02-5.10] Increased transport costs [OR 2.0; CI: 1.16-2.72], improved perceived health status [OR 2.45; CI:1.90-5.03], and fewer number of children [OR 2.22; 95% CI: 1.21-4.09] and were the positive determinants of adherence to HAART. Conversely, increased pill load significantly decreased the likelihood of adherence to HAART. [OR 0.62; 95% CI:0.41-0.94.]
Conclusion: With about two-fifths of the study population reporting inconsistencies in adhering to HAART, the adoption of appropriate adherence enhancing strategies directed at ensuring an uninterrupted access to free ART services and reducing pill load is strongly recommended.
Keywords: Adherence; Women; HIV/AIDS; HAART; Nigeria
Abbreviations: AIDS: Acquired Immune Deficiency Syndrome; ART: Antiretroviral Therapy; HAART: Highly Active Antiretroviral Drugs; PEPFAR: President’s Emergency Plan for AIDS Relief; HIV-Human Immunodeficiency Virus; PMTCT-Prevention of Maternal to Child Transmission; PLHIV-People Living with HIV/ AIDS; UCTH-University of Calabar Teaching Hospital; USAID: United States Agency for International Development.
Introduction
In 2010, an estimated 33.3 million persons are infected with the Human Immunodeficiency Virus (HIV) globally; of these, 68% live in sub Saharan Africa where more than 60% of People Living with HIV/AIDS (PLHIV) are women, disproportionately affected by the HIV-1 epidemic for both biological and socio-cultural reasons [1-3]. Nigeria currently has one of the highest HIV burden worldwide, with 3.1 million PLHIV and about 215,000 annual AIDS deaths [4,5]. Females constituted 58% (about 1.72 million) of PLHIV and each year 55% of AIDS death occurs among women. This has been attributed to gender equality issues and societal factors that put women at risk of developing HIV/AIDS [6].
The health condition of PLHIV has improved significantly with the introduction and widespread use of Anti-Retroviral that offers the possibility of dramatically reducing HIV/AIDS-related morbidity and mortality and has subsequently led to the scaling up of treatment/preventive programs especially in developing countries. In Nigeria, as part of the response to the raging HIV/AIDS epidemic, the government in partnership with international collaborators in 2002, established the National Ant Retroviral Therapy (ART) Program which further improved access to HIV care and treatment [7].The total number of PLHIV on ART steadily increased from 50,581 at the early stages of ART initiation in Nigeria in 2005 to 302,973 in 2009 [5]. So far, these efforts still remain suboptimal as only one-third of individuals requiring treatment in Nigeria have access to ART [5]. With increased access to treatment, and programs launched to provide free Highly Active Antiretroviral Therapy (HAART), successful long-term treatment of HIV requires sustainable high rates of adherence to the HAART regimen [8-10]. Adherence rates of at least 95% are considered appropriate to maximise the benefits of HAART [11-14], in improving virological, clinical and immunological outcomes [14-16]. Incomplete medication adherence has been strongly correlated with treatment failure, disease progression and development of drug resistance [17,18].
Furthermore, although women are more likely to seek healthcare and initiate HAART earlier than men [3,19] they may be more likely to show incomplete adherence and discontinue HAART during therapy [20]. Adherence to HAART amongst women may be compromised by child-care responsibilities and dependency ratios [21,22] economic pressures and lack of partner support [22,23]. Inconsistent adherence to HAART increases women’s risk of virologic failure and subsequent clinical progression. This study was therefore conducted to document adherence patterns and factors associated with adherence amongst women who have been disproportionately affected by the HIV/AIDS epidemic especially in a resource constrained settings like ours at the University of Calabar Teaching Hospital, Calabar Nigeria. There is paucity of information regarding adherence patterns amongst women in Nigeria This study was therefore necessary to fill the knowledge gap and develop appropriate adherence enhancing strategies.
Materials and Methods
The study was conducted at the Special treatment clinic of the University of Calabar Teaching Hospital (UCTH), Calabar Nigeria (formerly called the President’s Emergency Plan For AIDS Relief (PEPFAR) clinic). In June 2005, the Hospital was chosen as a centre by the United States Agency for International Development (USAID for the implementation of PEPFAR. It is a major centre responsible for the provision of care and support services for PLHIV in Cross River and other neighbouring states.
Study Population
The study population comprised of 282 non-pregnant HIV positive female patients who had commenced HAART at the UCTH from December 2012 - February 2013. All HIV positive consenting women who were eligible to participate wereconsecutively recruited over the study period till the attainment of required sample size.The exclusion criteria included; male patients, ART-naïve patients, terminally ill female patients, pregnant women and non-consenting patients. The inclusion criteria adopted for the study included; consenting female patients diagnosed and confirmed to be HIV positive, at least 18 years of age and had been on HAART for 3 months.
Study design
A cross-sectional analytical study was conducted among WLHIV on HAART
Data collection instrument
An interviewer-administered semi-structured questionnaire was designed and used to collect pertinent information on socio-demographic profile, clinical and treatment variables including treatment experiences, reasons for nonadherence, and support received. Patient’s self-report was used to determine adherence to HAART in the week preceding the interview.A self-report tool for screening adherence and barriers (The Brief Medication Questionnaire) was used to collect adherence data [24]. The degree of adherence was calculated based on the formula:
% Adherence over last 7 days =

For the purpose of this study a score of ≥ 95% represented good adherence while < 95% was rated as having poor/ suboptimal adherence.
Data analysis
SPSS for Windows version 19.0 was used for data analysis. Descriptive and inferential statistical tests were employed. Descriptive statistics (frequencies, proportions, means and standard deviation) were first used to summarize variables while inferential statistics bivariate (chi-square) and multivariate (logistic regression) analysis was used to determine significant correlates and predictors of adherence. The level of significance was set at p < 0.05. Logistic regression analysis was used to identify the independent risk factors of adherence.Variables found to be significant at 10% after performing bi-variate analysis, were entered into a logistic model and predictors were determined at 5% significance
Ethical clearance and consent
The study procedures and data collection instruments were reviewed and approved by The Health Research Ethical Committee of the University of Calabar Teaching Hospital. Permissions were obtained from the Head, Family Medicine department where the clinic is domiciled and the Chief Nursing Officer before commencement of the study. Written informed consents were obtained from all women for the use of their data for the study.
Results
Two hundred and eighty-two eligible female respondents attending the Special treatment clinic UCTH and receiving treatment were studied. Overall mean age of respondents was 33.6±8.5 years. The largest proportion of HIV positive women 137(48.6%) were in the age group 25-34years. The majority of those interviewed were currently married, 138 (48.9%) and more than a third 39.7 % had attained either secondary or Tertiary education. Most, 214 (75.9%) were currently employed but more than three- quarters, 217 (77.0%) earned less than The family characteristics of respondents are as presented in Table 2. More than half 150 (53.2%) had at least 3 children and 214 (75.9%) with at most 5 people in their households. Furthermore, majority, 240 (85.1%), of the respondents were not living alone, 261 (92.6%) had disclosed their HIV statusand 198 (70.2%) received support from family and friends. However, less than a fifth, 48 (17.0%) were members of a HIV support group and only 52 (18.4%) had spouses who were also HIV positive. The Medical profile of respondents interviewed (Table 3) revealed that more, 147 (52.1%) had been on HAART for over 24 months. The median duration on HAART was 24 months (inter-quartile range 24-44.8 months). Over two-fifths of the study population, 129 (45.7%) had experienced side effects while on HAART and majority, 189 (67.0%) reported non use of traditional herbal remedy alongside HAART. In addition, more than three-fifths of the WLHIV 195 (69.1%) were on 2 pills daily and most, 265 (94.0%) reported experiencing an improved health status since their placement on HAART. Also, most of the patients, 204 (72.3%) reportedly spent less than N1,000 ($ 6.25)on transportation to the health facility and less than a tenth 26 (9.2%) paid for services at the treatment site. Optimal adherence to HAART (≤95%) was achieved by more than half 168 (59.6%) of the respondents interviewed. Being busy (39.7%) was the commonest reason given for nonadherence. This was followed by simply forgetting medications (33.7%), depression (19.1%), inconvenient timing for medications schedule (12.1%) and fear of being discovered (11.7%) (Figure 1). Bivariate analysis revealed the following factors as significantly associated with adhering to HAART (Table 4 and 5): having fewer children (≤ 5), obtaining free ART services, perceiving one’s health status improved, not encountering side effects and paid more than N1,000 on transportation to the health facility (p<0.05) . The predictors of adherence to HAART amongst HIV positive women accessing treatment in the Special treatment clinic UCTH (Table 6) were: obtaining free ART services, perceived improved health status, reduced pill load, and having fewer children. However, WLHIV who spent more on transportation to health facility were more likely to adhere to their prescribed doses compared with those who spent less. This cross-sectional study aimed to contribute towards addressing gaps in knowledge regarding the prevalence and determinants of adherence to HAART amongst a cohort of HIV positive women receiving treatment in a Tertiary health facility in Cross River state, Nigeria. Adherence to effective ARV therapy has been strongly correlated with HIV suppression reduced rates of resistance increase in survival and improved quality of life [16,26]. Adherence to HAART was reported in 59.6% of the population studied. This finding was consistent with other studies done in Nigeria and an African setting [25, 27-29], but slightly higher than earlier reports 30-34 although, these studies included both sexes, females constituted a majority of the study population. This has serious implications for the success of the HIV treatment programs in Nigeria where slightly over 40% of the population most vulnerable to the HIV/AIDS epidemic are unable to attain optimal adherence rates. Missing or skipping doses among study participants was associated with being busy and simply forgetting medications.These two reasons, have been consistently mentioned in other studies [25, 27, 29, 32, 35,36] as the main risk factors for poor adherence. This may be attributed to the numerous roles women play in caring for the family. Women in most African countries may also be saddled with numerous responsibilities like caring for aged parents and relatives, thereby leaving them with little or no time to care for themselves or remember their medications. Having fewer children was found to be associated with better adherence in this study. This finding was in agreement with a similar study done in Ethopia which demonstrated as a significant predictor not having dependants. The odds of not having dependants was 1.95 higher than those who had dependants [37]. The reason may be that women who had many children may likely forget their pills because of their busy schedules or due to stress of caring for their children or members of their family. Also another common reason for poor adherence was forgetting. These reasons may further buttress this point. Limiting pill number to two daily and dosing schedule to once or twice daily has been found to yield a better adherence [16].Respondents taking more than two pills daily had a reduced likelihood of adhering to treatment compared to those on at least two pills per day. This finding was also reported by simliar studies [38,39] were pill burden reportedly had a strong impact on adherence. Similarly, the attainment of 100% adherence rate was observed in patients taking fewer pills as demonstrated by Cauldbeck et al in India. This could be attributable to the fact that women probably because of their busy schedules may not be able to incorporate a complex drug schedule into their day to day activity or may simply forget their medications [40]. Furthermore, obtaining free treatment at ART clinics was a significant predictor of adherence to treatment. Women adherers compared to those paying for services. This was in keeping with studies done in the south western Nigeria [41], and in Kenya [42]. Although drugs are being given free of charge in most health facilities offering ART services in Nigeria, patients are still required to pay some user fees at health facilities. e.g.opening of folders, and certain laboratory investigations Also there are some indirect costs these patients bear e.g. transportation costs. In addition perception of one’s health status as improved was a motivator for adherence as seen in this study. WLHIV who perceived their health status as improved following commencement on HAART were more adherent compared to those who perceived their health as not improved This finding was in agreement with previous report by Malcom and colleagues [43], but at variance with a study done in southern Nigeria which reported that good health was a risk factor for non-adherence where patients tend to abandon treatment once their health status improved [25]. Social support has been demonstrated by Ambebir and colleagues in Ethiopia as a significant predictor of adherence [35]. Surprisingly, perceived social support and disclosure of one’s HIV status were not associated with adherence in this study. This finding is in contrast to findings from other studies conducted in Ethopia [35,44,45] where greater social support predicted not only better adherence, but also a more consistent adherence. Another recent report amongst pregnant HIV positive women by Ekama et al. [46] in Lagos (south western Nigeria) demonstrated that disclosure of one’s HIV status was associated with good adherence and ultimately resulted in better support. This was however not the case with our study. Similarly, membership of a HIV support group did not have any impact on adherence amongst the study population. This was contrary to findings observed in a study done in South-western Nigeria were attendance of support group meetings improved adherence [41]. This could be attributable to the fact the support groups were probably focusing more on income generating activities without emphasizing the treatment goal for every HIV client placed on HAART. This study also revealed that less than a fifth of WLHIV were members of a support group. This may be linked with their busy schedules or issues related to stigmatization where women were afraid of being found out if they attended meetings. Finally, a higher cost of transportation to the Health facility was associated with optimal adherence to HAART. This was quite odd and the reason for this is not clear. The fact that they had to pay more for transportation to the health facility may have motivated them take their medications more seriously considering the effect this had on their finances compared to those who paid little or nothing to the health facility. Certain limitations were observed in this study. The crosssectional nature of the study did not allow for inferences to be drawn as to causal relationship among variables. The use of patient’s self-report to assess medication adherence was a limitation in this study since patients had to recall their medication adherence in the previous week which methodologically could be associated with recall bias. To help reduce recall bias, the period of recall was limited to 7 days prior to the study. Patients also tended to either over- or underestimate their adherence to HAART. This drawback was further worsened by the inability to corroborate patient self-reported adherence with viral loads and CD4 responses owing to financial and logistic constraint of frequent laboratory monitoring. The medication adherence rate recorded in this study was low among HIV positive women in UCTH Calabar, Nigeria. This has serious implications for treatment failure and subsequently drug resistance. The predictors of adherence in the present study included: having fewer children, non-payment of ART services, reduced pill load, perceived health status as improved and increased transport cost to health facility. The authors therefore recommend the provision of free services at every ART clinic which should include treatment of opportunistic infections and required important investigations. This will aid in tackling the challenges of poor adherence. The use of treatment or adherence reminders or supporters may be very useful especially for women who are saddled with the additional responsibilities of home and family and tend to forget their medications in the process. In addition, family planning must be stressed and given out to HIV positive women whose families have to be planned to avoid having too many children. Lastly, ARV manufacturing pharmaceutical companies should ensure that all recommended ARVs consist of a total of two pills or less daily. The authors would like to thank the staff of the Special Treatment clinic in the department of Family Medicine, University of Calabar Teaching Hospital for the support and assistance during the collection of data.Discussion
Factors associated with Adherence to HAART
Limitations
Conclusion
Acknowledgements
- World Health Organization (WHO) (2009) UNAIDS Towards universal access-Scaling up priority HIV/AIDS interventions in the health sector (progress report 2009), Geneve, Switzerland.
- Dembélé M, Saleri N, Carvalho AC, Saouadogo T, Hien AD, et al. [2010] Incidence of tuberculosis after HAART initiation in a cohort of HIV-positive patients in Burkina Faso. Int J Tuberc Lung Dis 14:318-323.
- Muula AS, Ngulube TJ, Siziya S, Makupe CM, Umar E, et al. (2007) Gender distribution of adult patients on highly active antiretroviral therapy (HAART) in Southern Africa: a systematic review. BMC Public Health 7:63.
- UNAIDS Global AIDS Epidemic Update (2011). Geneva, Switzerland.
- Federal Ministry of Health (FMOH) (2010) National HIV sero- prevalence Senntinnel Survey. Abuja: Federal ministry of health.
- National Agency for the Control of AIDS (NACA) (2011) Fact sheet Women, girls and HIV in Nigeria.
- Odutolu O, Ahonsi B, Gboun M, Jolayemi , Adeyi O, et al. (2006) Response to HIV/AIDS in Nigeria: Olusoji Adeyi (1st edn) A Nation on the Threshold. Massachusetts Harvard University Press, USA.
- Moatti JP, Spire B (2003) Economic and socio-behavioural issues related to highly active antiretroviral therapies for HIV infection: the contribution of social science research. Med Sci 19: 878-884.
- Rao D, Kekwaletswe TC, Hosek S, Martinez J, Rodriguez F (2007) Stigma and social barriers to medication adherence with urban youth living with HIV.AIDS Care 19:28-33.
- Tapper ML, Flexner C, Eron JJ, Molina JM (2004) Simplifying antiretroviral therapy. AIDS Read 14: 355-360, 367-371.
- McPherson-Baker S, Jones D, Durán RE, Klimas N, Schneiderman N (2005) Development and implementation of a medication adherence training instrument for persons living with HIV: the MATI. Behav Modif 29: 286-317.
- Amico KR, Toro-Alfonso J, Fisher JD (2005) An empirical test of the information, motivation and behavioral skills model of antiretroviral therapy adherence. AIDS Care 17: 661-673.
- Remien RH, Bastos FI, Jnr VT, Raxach JC, Pinto RM, et al. (2007) Adherence to antiretroviral therapy in a context of universal access, in Rio de Janeiro, Brazil. AIDS Care 19:740-748.
- Weiser S, Wolfe W, Bangsberg D, Thior I, Gilbert P (2003) Barriers to antiretroviral adherence for patients living with HIV infection and AIDS in Botswana. J Acquir Immune Defic Syndr 34:281-288.
- Weiss L, French T, Finkelstein R, Waters M, Mukherjee R (2003) HIV-related knowledge and adherence to HAART. AIDS Care 15:673-679.
- Paterson DL, Swindells S, Mohr J, Brester M, Vergis EN (2000) Adherence to protease inhibitor therapy and outcomes in patients with HIV infection.Ann Intern Med.133:21-30.
- Nilsson Schönnesson L, Diamond PM, Ross MW, Williams M, Bratt G (2006) Baseline predictors of three types of antiretroviral therapy (ART) adherence: A 2-year follow-up. AIDS Care 18:246-253.
- Poppa A, Davidson O, Deutsch J, Godfrey D, Fisher M, et al. (2004) British HIV Association (BHIVA)/British Association for Sexual Health and HIV (BASHH) guidelines on provision of adherence support to individuals receiving antiretroviral therapy (2003). HIV Med 5:46-60.
- Cornell M, Myer L, Kaplan R, Bekker LG, Wood R (2009) The impact of gender and income on survival and retention in a South African antiretroviral therapy programme. Trop Med Int Health 14:722-731.
- Kempf MC, Pisu M, Dumcheva A, Westfall AO, Kilby JM (2009) Gender differences in discontinuation of antiretroviral treatment regimens. J Acquir Immune Defic Syndr 52: 336-341.
- Merenstein D, Schneider MF, Cox C, Schwartz R, Weber K, et al. (2009) Association of child care burden and household composition with adherence to highly active antiretroviral therapy in the Women's Interagency HIV Study. AIDS Patient Care STDS 23: 289-296.
- Vyavaharkar M, Moneyham L, Tavakoli A, Phillips KD, Murdaugh C, et al. (2007) Social support, coping, and medication adherence among HIV-positive women with depression living in rural areas of the southeastern United States. AIDS Patient Care STDS 21: 667-680.
- Murray LK, Semrau K, McCurley E, Thea DM, Scott N, et al. (2009) Barriers to acceptance and adherence of antiretroviral therapy in urban Zambian women: a qualitative study. AIDS Care 21:78-86.
- Svarstad BL, Chewning BA, Sleath BL, Claesson C (1998) The brief medication questionnaire: A tool for screening patient adherence and barriers to adherence. Patient Educ Couns 37:113–124
- Olowookere SA, Fatiregun AA, Akinyemi JO, Bamgboye AE, Osagbemi GK (2008) Prevalence and determinants of nonadherence to highly active antiretroviral therapy among people living with HIV/AIDS in Ibadan, Nigeria J Infect Dev Ctries 2:369-372.
- Hogg R, Heath K, Bangsberg D, Yip B, Press N, et al.(2002) Intermittent use of triple-combination therapy is predictive of mortality at baseline and after 1 year of follow-up. AIDS Care 16:51-58.
- Oku AO, Owoaje ET, Ige OK, Oyo-Ita A (2013) Prevalence and determinants of adherence to HAART amongst PLHIV in a tertiary health facility in south-south Nigeria. BMC Infect Dis 13:401.
- Shaahu VN, Lawoyin TO, Sangowawa AO (2008) Adherence to highly active antiretroviral therapy (HAAT) at a Federal Medical Centre. Afr J Med Sci37: 29-36.
- Agu KA, Okojie O, Oqua D, King RC, Omonaiye O, et al. (2011) Medication Adherence and Risk factors for Non-adherence among Patients taking Highly Active Antiretroviral Therapy. West African Journal of Pharmacy 22:19-26.
- Iliyasu Z, Kabir M, Abubakar IS, Babashani M, Zubair ZA (2005) Compliance to antiretroviral therapy among AIDS patients in Aminu Kano Teaching Hospital, Kano, Nigeria. Niger J Med 14:290-294.
- Nwauche C, Erhabor O, Ejele O, Akani C (2006) Adherence to Antiretroviral therapy among HIV-infected subjects in a resource limited setting in the Niger Delta of Nigeria. Afr J Health Sci 13:13 -17.
- Talam NC, Gatongi P, Rotich J, Kimaiyo S (2008) Factors affecting antiretroviral drug adherence among HIV/AIDS adult patients attending HIV/AIDS clinic at Moi Teaching and Referral Hospital, Eldoret, Kenya. East Afr J Public Health 5:74-78.
- El-Khatib Z, Ekstrom AM, Coovadia A, Abrams EJ, Petzold M, et al. (2011) Adherence and virologic suppression during the first 24 weeks on antiretroviral therapy among women in Johannesburg, South Africa - a prospective cohort study. BMC Public Health 11:88.
- Musiime S, Muhairwe F, Rutagengwa A, Mutimura E, Anastos K,( 2011) Adherence to highly active antiretroviral treatment in HIV-infected Rwandan women. PLoS One 6:1-6.
- Amberbir A, Woldemichael K, Getachew S, Girma B, Deribe K (2008) Predictors of adherence to antiretroviral therapy among HIV-infected persons: a prospective study in Southwest Ethiopia. BMC Public Health 8:1-10.
- Wakibi SN, Ng'ang'a ZW, Mbugua GG (2011) Factors associated with nonadherence to highly active antiretroviral therapy in Nairobi, Kenya. AIDS Res Ther 43:1-8.
- Endrias M, Alemayebu W, Gail D (2008) Adherence to HAART in PLWHA at Yirgalem Hospital South Ethopia. Ethopian Journal of health Development 22:174-179.
- Falang KD, Akubaka N, Jimam NS (2012) Patient Factors impacting Antiretroviral drug adherence in a Nigerian tertiary Hospital. Journal of Pharmacology and Pharmacotherapeutics 3:138-142.
- Sow PG, Toure K, Coume M, Dia AT, Traore I (2012) Predictors of ART adherence among HIV infected individuals in Dakar, Senegal. Journal of Medicine and Medical Science 3:212-216.
- Chesney M (2003) Adherence to HAART regimens. AIDS Patient Care STDS 17:169-177.
- Afolabi MO, Ijadunola KT, Fatusi AO, Olasode OA (2009) Determinants of adherence to antiretroviral drugs among people living with HIV/AIDS in the Ife-Ijesa zone of Osun state, Nigeria. Afr J Prm Health Care Fam Med1:6.
- Sarna A, Luchters S, Geibel S, Munyao P, Kaai S et al.( 2005) Promoting adherence to antiretroviral therapy through a directly administered antiretroviral therapy (DAART) strategy in Mombasa, Kenya. Population Council.
- Malcolm SE, Ng JJ, Rosen RK, Stone VE (2003) An examination of HIV/AIDS patients who have excellent adherence to HAART. AIDS Care 15: 251261.
- Chesney M (1997) New antiretroviral therapies: Adherence challenges and strategies. Presented at the Adherence in HIV Therapy: Implication for Nursing practice, San Francisco, USA.
- Gordillo V, del Amo J, Soriano V, González-Lahoz J (1999) Sociodemographic and psychological variables influencing adherence to antiretroviral therapy. AIDS 13:1763-1769
- Ekama SO, Herbertson EC, Addeh EJ, Gab-Okafor CV, Onwujekwe DI, et al. (2012) Pattern and determinants of antiretroviral drug adherence among Nigerian pregnant women. J Pregnancy 2012:1-6.
FIGURE 1
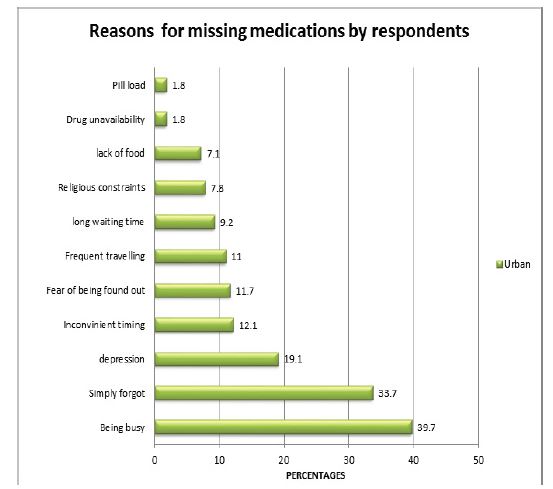
Figure 1: Reasons for missing medications by respondents
Tables at a glance
Figures at a glance