Not so solitary! A case of a Solitary Fibrous Tumors of the Pleura
Received Date: July 02, 2025 Accepted Date: July 15, 2025 Published Date: July 19, 2025
doi: 10.17303/croa.2025.10.103
Citation: Jonathan Torrens Olán (2025) Not so solitary! A case of a Solitary Fibrous Tumors of the Pleura. Case Reports: Open Access 10: 1-6
Abstract
Primary neoplasms Of the pleura are rare and generally divided into two major categories: diffuse and localized tumors. The most frequently encountered pleural tumor is mesothelioma, which arises from mesothelial tissue. It is more commonly associated with asbestos and has poor prognosis. Conversely, localized pleural tumors are rare and immunohistochemical studies have demonstrated that these tumors have a mesenchymal rather than a mesothelial origin. For this reason, the term "localized mesothelioma" was abandoned, and these tumors are now called solitary fibrous tumors Of the pleura (SET P). SFTP generally display benign features yet malignant potential has Iken described in 10-20% of cases. Only about 5% of all malignant pleural tumors are comprised of SFTP SFTP are typically asymptomatic and discovered incidentally during chest X-ray examination showing a well-defined, lobular, solitary nodule or mass located in the periphery and typically adjacent to the pleural surface. This is important to have in the differential diagnosis, because when symptoms occur, they are usually secondary to the mass effect on adjacent Structures and typically include cough, chest pain and dyspnea, which are very corn. mon respiratory symptoms for many conditions. It is also associated with paraneoplastic syndromes such as hypertrophic pulmonary osteoarthropathy and refractory hypoglycernia. The most important and valuable positive markers in SFTP are CD34, CD99, BcL2 and STAT.6, In most cases complete surgical resection is the only necessary treatment, and recurrence is rare.
Keywords: Pleural Tumor; Pleural Disease; Solitary Fibrous Tumor
Case Report
A 74-year.old woman with a past medical history significant for essential hypertension, former smoker, and goiter presented to the urgency room with dyspnea on exertion of one month of evolution, 'Ihe patient has no known asbestos exposure. Physical examination was remarkable for decreased breath sounds on the left hemithorax, Chest Xray was initially evaluated and showed evidence of near complete opacification of the left lung, Given this finding, a chest CT scan was performed which revealed a 15.1 cm x II cm x 19.3 cm extrapulmonary and intrapulmonary mass in the left hemithorax with compression and subtotal collapse of the left lower lung, A PET CT scan was also performed and showed a 13 cm FDG avid mass in the left chest involving nearly all the left lower lung, and the posterior segment of the left upper lung. This is a tool which helps to categorizæ the tumor between malignant and benign, depending on the of its metabolic activity
A CT guided core biopsy of the lesion was done, and pathology was consistent with a solitary pleural fibrous tumor. Immunohistxhemistry was strongly positive for CD34, STAT6, and negative for pankeratin. The patient was then referred to a thoracic surgery specialist for evaluation. She was taken to the operating room and underwent a tumor embolization, to reduce blood loss and then a complete tumor resection was perfromed. The surgery was successful with an encouraging prognosis.
Discussion
Solitary fibrous tumor Of the pleura is a rare neoplasm, and it accounts for almost 5% of all pleural tumors. However. it can also present as an intrapulmonary mass. Although most are benign, around 12% are found to be malignant. It usually occurs in the sixth and seventh decades of life with no sex predomi- nance. Incidence is less than 3 per I patients and less than cases have been described in the literature [l -51. Histologi- cally it exhibits a proliferation of uniform elongated spindle cells alternating with areas of connective tissue arranged in a haphaz- ard distribution or 'pattern less pattern'. Immunohistochemistry plays an important role for the histopathologic diagnosis of this tumor. being the CD34, CD99, Bcl-2 and STAT-6 the most valu- able positive markers 16-81 (Figures and 4).
Conclusion
In patients with a solitary fibrous tumor of the pleu- ra, a complete surgical resection with negative margin remains the treatment of choice in all cases, as performed in our patient. At this moment is controversial the role for conventional Che. motherapy or radiotherapy as adjuvant therapy in these cases. Vascular adhesions to adjacent visceral or parietal pleura are fre- quent leading to bleeding, however, formal lobectomy is rarely required. Benign SFTP has a high cure rate, Around 8% of pa. tients develop local recurrence, which is usually amenable to cu. rative re-excision, with an overall long-term cure rate of 88% to 92%, Patient tolerated the procedure and remained stable with. out recurrence,
- Sun N, Wang J, Cheng Z Han W, Li G, et al. (2020) Solitary fl. brous tumor of the pleura in a 22-year.old woman: a case report. J Int Med Res 2020.
- Jeon, HW, Kwon SS, Kim YD (2014) Malignant solitary fibrous tumor of the pleura slowly growing over 17 years: case report. J Cardiothorac Surg 9: 113.
- Guinee DG, Allen TC Primary pleural neoplasia-en. tities other than diffuse malignant mesothelioma. Archives of Pathology & Laboratory Med 132: 1149-70.
- Abu Arab W (2012) Solitary fibrous tumours of the pleura. Eur J Cardiothroac Surg 41: 587-97.
- Hohenforst.Schmidt W, Grapatsas K, Dahm M (2017) Soli. tary fibrous tumor: A center's experience and an overview of the symptomatology, the diagnostic and therapeutic procedures of this rare tumor. Respir Med Case Rep 21:99-104.
- CieSlik-Wolski B, Pryt L, Szlachcifiska A, Walczak-Pasz G, Je- sionek-Kupnicka D, et al. (2015) Solitary fibrous tumor Of the pleura - analysis of 18 cases. Kardiochir Torakochirurgia POI 12: 208-15.
- Erica Rego, Brian A Solomon (2018) Giant solitary fibrous tu- mor Of the pleuraRego Solomon BA. Giant solitary fibrous tumor of the pleura. Appl Radiol 47:41-3.
- Jenkins LA, O-Yurvati AH (2008) Solitary Fibrous Pleural Tumor. J Am Osteopath Assoc 108: 307-9.
FIGURE 1
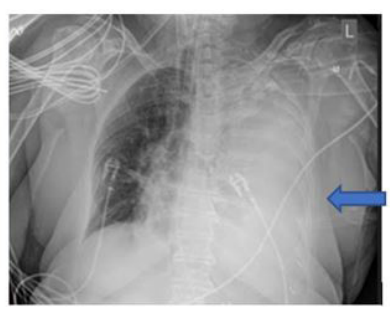
FIGURE 2
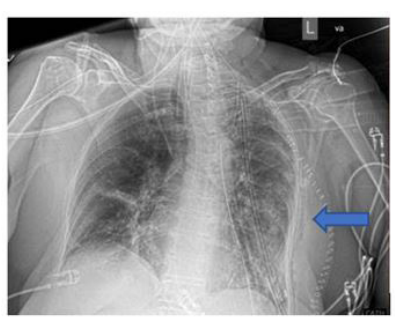
FIGURE 3

FIGURE 4

Figures at a glance