Ciprofloxacin Induced Torsades De Pointes – A Case Report
Received Date: December 28, 2022 Accepted Date: January 28, 2023 Published Date: January 31, 2023
doi: 10.17303/croa.2023.8.102
Citation: Neeladri Misra, Jeffrey Halley (2023) Ciprofloxacin Induced Torsades De Pointes – A Case Report. Case Reports: Open Access 8: 1-6
Abstract
Fluoroquinolones are a effective class of antibiotics used to treat a variety of bacterial infections. Their excellent bioavailability and broad spectrum antimicrobial coverage make them a excellent choice to use for treating bacterial infections. However an inappropriate and excess use of this class of drugs especially in the outpatient setting has resulted in increased adverse events of arrhythmias such as Torsades that can be life threatening and fatal . This has resulted in a increased awareness amongst physicians and an FDA warning on its labelling with guidelines on use of fluoroquinolones for special circumstances only.
We highlight one such case of Torsades De Pointes induced by Ciprofloxacin that was prescribed for a sinus infection for a 61 yr old Caucasian male with ischemic cardiomyopathy and was on antiarrhythmic dofetilide that presented to the hospital with complaint of repeated episodes of ICD firing.
Keywords: Torsades De pointes; Ciprofloxacin; Sotalol, dofetilide; Lidocaine; QTc; ICD; Amiodarone
Case Report
A 61 yr Caucasian male with past medical history of Coronary artery disease S/p CABG 10 years ago, Internal cardioverter-defibrillator placement for HFREF and Non sustained ventricular tachycardia , HFREF with EF 35%, Hypertension , Hyperlipidemia Chronic obstructive pulmonary disease, Diabetes mellitus And h/o Alcohol abuse, presented to the emergency room with complaints of his ICD firing .
The patient gave a history that he was woken from sleep after feeling his defibrillator go off once . He called paramedics and when they came in, the defibrillator went off a few more times . During the paramedic assessment a episode of ventricular tachycardia was recorded on EKG. The Patient was brought to our emergency room where the patient's ICD fired again.
An 12 lead EKG was immediately done in the emergency room and showed Torsades rhythm . His initial QTC was measured at 620ms
The patient was given Amiodarone 150 mg bolus and an Amiodarone Drip was started along with a Magnesium infusion. He was awake and hemodynamically stable. Cardiology was consulted and the patient was admitted to an cardiac telemetry floor . A CBC, CMP, Mg Level and chest x ray were ordered which were within normal limits.
On admission to the floor a detailed history and physical exam was done by the cardiology team. During the history it was found the Patient had been recently prescribed ciprofloxacin for symptoms of sinusitis by his Primary care physician. It was unclear why this drug was chosen as it was unusual for this drug to be given for sinusitis in the presence of safer alternatives and due to contraindication given patient also takes Dofetilide for control of his nonsustained ventricular tachycardia . Given this history findings the we concluded that patient likely had developed torsades de pointe due to drug interaction of ciprofloxacin with dofetilide.
An Electrophysiology consult was put in for further management of the patient. Their recommendations were to Hold both Dofetilide and amidodarone (due to QTc prolonging effect of both drugs) and start the patient on a lidocaine infusion at 2 milligrams/minute.
The patient was monitored very closely on a cardiac telemetry unit on the lidocaine infusion with serial EKG monitoring and electrolytes levels done BID. An repeat EKG showed his Qtc interval had decreased to 471msec.
Per recommendations from electrophysiology The patient was continued on the Lidocaine drip at 2mg/min for next 24 hrs. The following day patient remained Clinically asymptomatic with no telemetry events reported, and his Physical exam unremarkable.
His Day 3 EKG showed Qtc interval at 450 msec. Electrophysiology decided on stopping the lidocaine drip and starting the patient on Sotalol 160mg BID, with an EKG 2 hrs after each dose of sotalol for Qtc interval measurement. The Patient's potassium levels and magnesium levels were kept about 4 and 2 respectively through replacement protocol.
Patient during the rest of his hospitalization remained asymptomatic and developed no telemetry events after starting sotalol. His EKG on Day 3 showed Qtc interval of 462ms, 471ms. On Day 4 his Qtc interval got worse at 489ms so His sotalol dose was decreased to 120mg PO BID.
A 2D Echocardiogram showed Normal left ventricular chamber size with moderate to severe concentric left ventricular hypertrophy, moderate aortic stenosis., with ejection fraction of 30 - 35%.
After total of 5 days of hospitalization and frequent monitoring of electrolytes and EKG the Patient was discharged on sotalol 120 mg PO BID. Prior to Discharge extensive education and instructions given were to the patient that No Antibiotic was to be taken without first confirming with Electrophysiologist or Cardiologist. He was asked to Follow up with the cardiologist and Electrophysiologist to discuss further plan of management for recurrent Vtach episodes.
Dicussion
Our case highlights the importance of restricting the use of fluoroquinolones in patients and especially those with preexisting arrhythmia while checking for drug -drug interactions prior to prescribing .The FDA warnings have certainly changed the practice of fluoroquinolone use especially in the outpatient setting but more education and intervention are needed to prevent such adverse events of this drug class . The Empiric use of fluoroquinolones has been implicated in treatment of variety of disease process but case reports and research have well documented the adverse effects they have on the body [8].
Moxifloxacin and Levofloxacin carries the greatest risk of QT prolongation from all available quinolones in clinical practice and it should be used with caution in patients with predisposing factors for Torsades de pointes such as those taking antiarrhythmic therapy. [1] [5]. The Fluoroquinolones prolong the QT interval by blocking voltage-gated potassium channels, especially the rapid component of the delayed rectifier potassium current I(Kr), expressed by HERG (the human ether-a-go-go-related gene) [1]
Amongst fluoroquinolones Ciprofloxacin may be given to select patients because the agent is believed to be safer than other drugs in QTC prolongation in its class [2] however in patients taking class 3 antiarrhythmic agents known to predispose to Torsades the interaction cause serious arrhythmias and can be life-threatening. [3][4]
For URTI infections Amoxicillin/Clavulanate, Oral Cephalosporins and Doxycycline are safer and more effective treatment options and fluoroquinolones have very little role with restricted use for special circumstances. Even in such cases consultation with Infectious disease specialist when available and use of appropriate fluoroquinolones drug with least dosage regimen is preferred
Patients who have a predisposing factor that already increases the QtC interval such as in our case where the patient was on dofetilide the interaction with Ciprofloxacin resulted in torsades de pointes and would have been fatal if not for the patients had a existing defibrillator. Dofetilide is an very effective antiarrhythmic agent for maintenance of sinus rhythm and is used to convert patients in atrial flutter and fibrillation. It is also used in Nonstained Vtach patients to help prevent arrthymias [7] . The risk of dofetilide induced torsade de pointes (Tdp) is low when used with strict dosing criteria guided by renal function, QT interval and concomitant drug therapy. [6]
In cases of torsades Treatment of patients focus mainly of removal of offending drug that prolong the Qtc , and stabilization of the heart rhythm using antiarrthymic agents without Qtc effect that stabilize the cardiac membrane such as Lidocaine .
In conclusion fluoroquinolones antibiotics have a restricted role in use for treating bacterial infections and their use needs to be reserved for special circumstances where no other safer alternative is present . Preference to use safer antibiotics classes should always be considered especially in patients with preexisting cardiac arrhythmias.
Amongst drugs in the fluoroquinolones class, ciprofloxacin though considered relatively safer than other fluoroquinolones [2] in causing Qtc prolongation however if used in patients who are already on antiarrthymic drugs can lead to Qtc prolongation leading to Torsades [6] resulting in hospitalization and morbidity as highlighted in our case report .
- Briasoulis A, Agarwal V, Pierce WJ (2011) QT prolongation and torsade de pointes induced by fluoroquinolones: infrequent side effects from commonly used medications. Cardiology 120:103-10
- Frothingham R (2001) Rates of torsades de pointes associated with ciprofloxacin, ofloxacin, levofloxacin, gatifloxacin, and moxifloxacin. Pharmacotherapy 21: 1468-72
- Keivanidou A, Arnaoutoglou C, Krommydas A, Papanikolaou G, Tsiptses K et al. (2009) Ciprofloxacin induced acquired long QT syndrome in a patient under class III antiarrhythmic therapy. Cardiol 16:172-4
- Aktas MK, Shah AH, Akiyama T (2007) Dofetilide-induced long QT and torsades de pointes. Ann Noninvasive Electrocardiol 12: 197-202
- Liu X, Ma J, Huang L, Zhu W, Yuan P et al. (2017) Fluoroquinolones increase the risk of serious arrhythmias: A systematic review and meta-analysis. Medicine (Baltimore) 96: e8273
- Owens RC Jr, Ambrose PG (2002) Torsades de pointes associated with fluoroquinolones. Pharmacotherapy 22: 663-8
- Jaiswal A, Goldbarg S (2014) Dofetilide induced torsade de pointes: mechanism, risk factors and management strategies. Indian Heart 66: 640-8
- Yasynetskyi M, Banyra O, Nikitin O, Ventskivska I, Kozlov V et al. (2021) Mixed Sexually Transmitted Infections in Infertile Couples: Empirical Treatment and Influence on Semen Quality. Recent Adv Antiinfect Drug Discov 16: 227-36
FIGURE 1
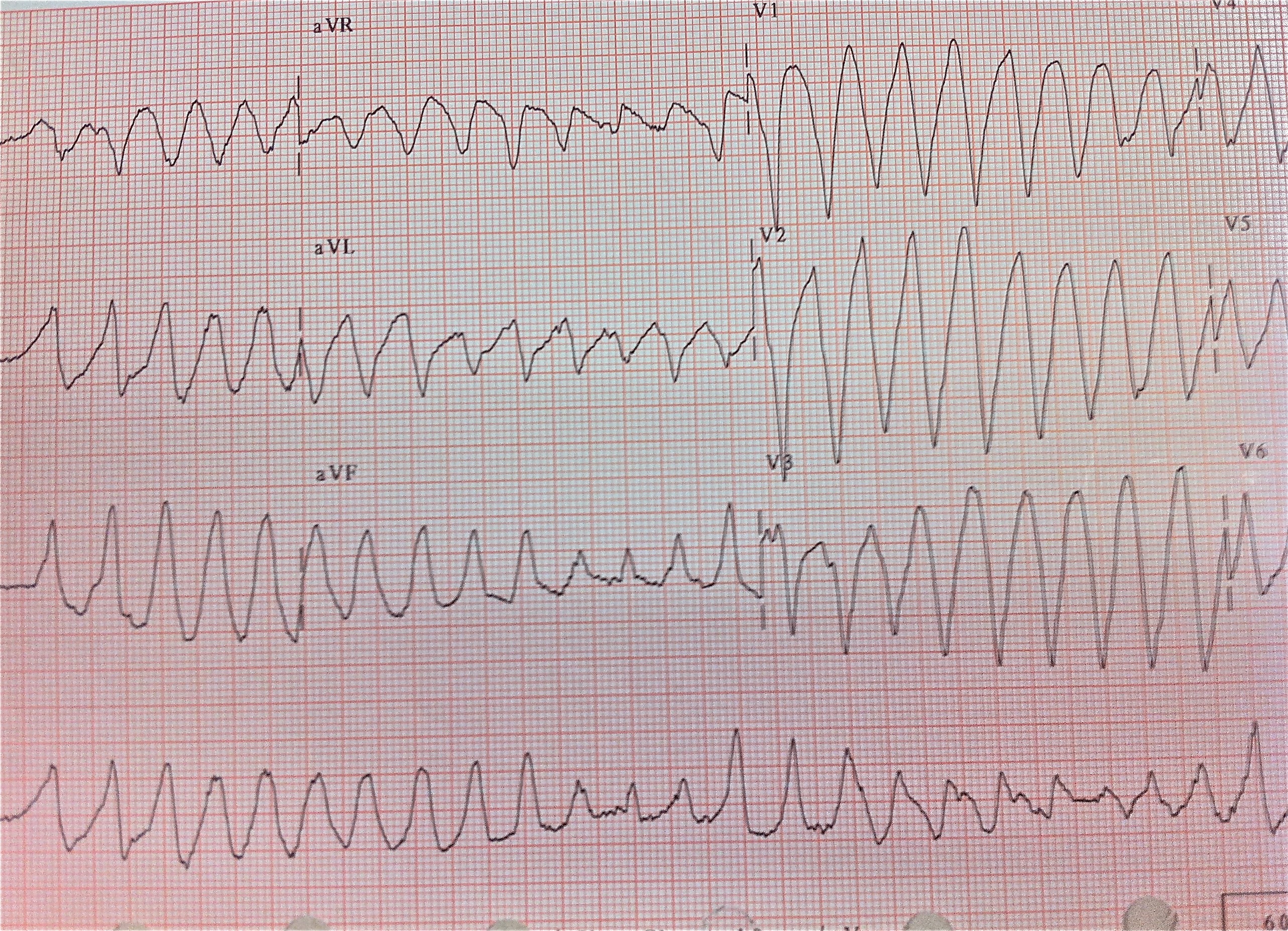
Figure 1: EKG at presentation showing Torsades de pointes
FIGURE 2
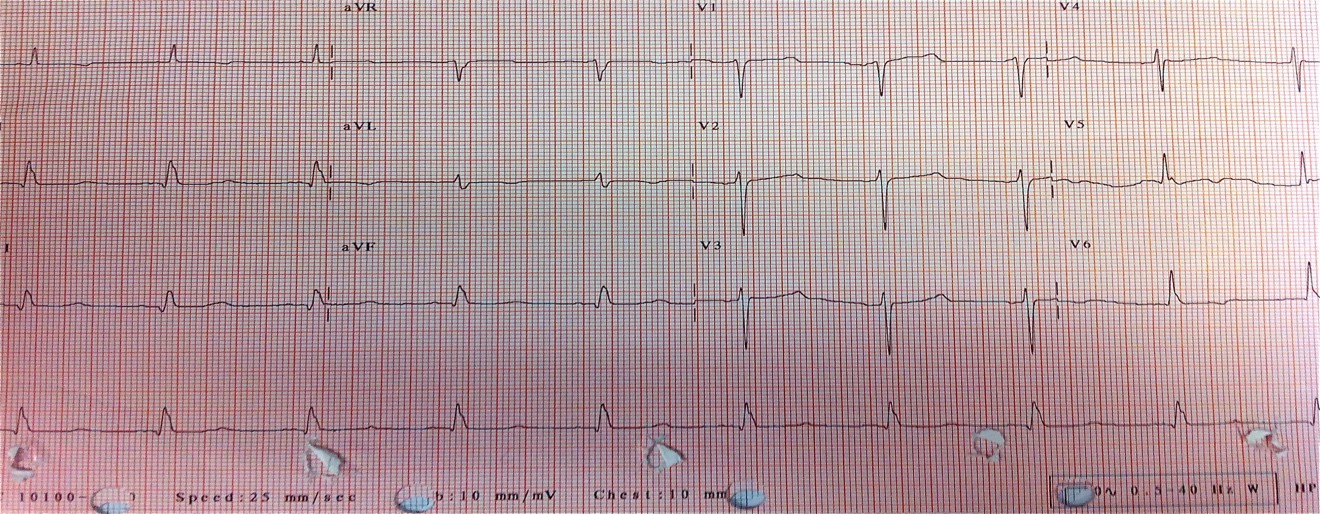
Figure 2: EKG on Day 4 after 48 hours of Sotalol, QTC measured at 470ms
Figures at a glance