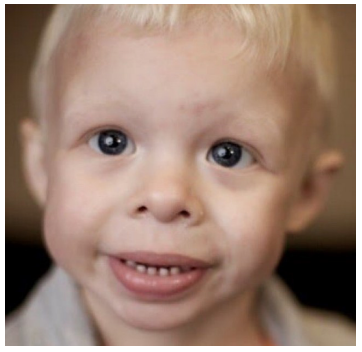
Figure 1: Characteristic facial features in Williams-Beuren syndrome (see text explanations). [13]
Affected organ or body system: Symptoms for following-up |
Early childhood |
Child hood |
Adult hood |
Frequency |
RECOMMENDATIONS |
Thorough physical examination |
Yes |
Yes |
Yes |
NA |
At each physician visit or at least once annually. Ensure that the growth delay is not drastic, take measures as necessary |
CAUTION by SEDATION or ANESTHESIA!!! |
Yes |
Yes |
Yes |
||
ViSÎOI1: |
|
|
|
|
Ophthalmological examination lifelong once annually for any vision problems and for strabismus for all ages |
Strabismus (esotropia) |
Yes |
|
|
50 |
|
Hyperopia (hypermetropia) |
|
Yes |
Yes |
50 |
|
Cataract |
|
|
Yes |
|
|
Otorhinolaryngology: |
|
|
|
|
Otorhinolaryngology examination and audiogram, lifelong once annually. |
Recurrent otitis media; chronic otitis media |
Yes |
Yes |
|
50 |
|
Progressive sensorineural hearing loss |
|
Yes |
Yes |
65 |
|
Hypersensitivity to sounds |
Yes |
Yes |
Yes |
90 |
|
Dental status: |
|
|
|
|
Regular dental examinations and professional dental cleaning every 6 months up to 12 years of age; |
Enamel hypoplasia |
Yes |
Yes |
Yes |
95 |
|
Microdontia, Diastema |
Yes |
|
|
|
|
Malocclusion |
|
Yes |
Yes |
85 |
|
|
|
|
|
|
Basic examination at each physician |
|
visit for elevated blood pressure (of |
||||
|
3 or 4 extremities), heartfrequency, |
||||
|
heart tones. |
||||
|
Once annually, lifelong: |
||||
|
electrocardiogram (ECG). |
||||
|
At least once annually for age 1 to 5 |
||||
Cardiovascular problems: |
years and once in every 2 years |
||||
|
thorough examination by a |
||||
|
cardiologist with blood pressure |
||||
|
measurement on 3 or 4 |
||||
|
extremities,echocardiography, |
||||
|
Doppler sonography (for severe |
||||
|
stenosis incl. CT, MRI, |
||||
|
catheterization), ECG. |
||||
Basic examination |
Yes |
Yes |
Yes |
80 |
|
Supravalvular aortic |
Yes |
Yes |
Yes |
75 |
|
stenosis |
|
|
|
|
|
Supravalvular pulmoniC |
Yes |
Yes |
Yes |
25 |
|
stenosis |
|
|
|
|
|
Peripheral pulmonic |
Yes |
|
|
50 |
|
stenosis (PPS) |
|
|
|
|
|
Stenoses of other arteries |
|
Yes |
Yes |
20 |
|
Ventricular septal defect |
Yes |
|
|
10 |
|
(VSD) |
|
|
|
|
|
Arterial hypertension |
|
Yes |
Yes |
50 |
|
Prolonged QT interval |
|
Yes |
Yes |
13 |
|
|
|
|
|
|
Screening at diagnosis - single |
|
ultrasonographic (US) examination |
||||
|
(Doppler) of the kidneys and |
||||
|
renalarteries; US evaluation for |
||||
|
nephrocalcinosis; for bladder |
||||
|
malformations, diverticula. In adults |
||||
|
- USexamination once every 10 |
||||
Genitourinary problems: |
years. |
||||
|
Annually lifelong: serum BUN |
||||
|
(serum urea) and urinalysis; serum |
||||
|
creatinine - as necessary.In case of |
||||
|
complications (persistent |
||||
|
hypercalcemia, hypercalciuria, |
||||
|
nephrocalcinosis) - |
||||
|
consultationwith nephrologist. |
||||
Malformations |
Yes |
Yes |
Yes |
5 |
|
Enuresis (diurnal, |
|
|
|
|
|
nocturnal) |
|
Yes |
|
50 |
|
Nephrocalcinosis |
|
Yes |
Yes |
<5 |
|
Bladder diverticulosis |
|
Yes |
Yes |
50 |
|
Gastrointestinal problems: |
|
|
|
|
Continuous prevention of constipation. Each situation of abdominal pain should be addressed critically and having in mind that abdominal pain may be due to mesenteric artery stenosis(!) but alsoreflux, hiatal hernia, peptic ulcer, cholelithiasis, diverticulitis, ischemic bowel disease (due to motilityproblems, rectal prolapse, hemorrhoids, bowel perforation), and quite common - psychogenic (out offear). |
Feeding difficulties |
Yes |
Yes |
— |
70 |
|
Constipation |
Yes |
Yes |
Yes |
50 |
|
Diverticula of the colon |
|
Yes |
Yes |
30 |
|
Prolapse of the rectum |
Yes |
Yes |
— |
10 |
|
Skin and soft tissues: |
|
|
|
|
At least once annually, lifelong: surgical examination for hernias; |
Soft and hyperelastic skin |
Yes |
Yes |
Yes |
90 |
|
Inguinal hernia |
Yes |
|
|
40 |
|
Umbilical hernia |
Yes |
|
|
50 |
|
Premature greying of hair |
|
|
Yes |
90 |
|
Musculoskeletal problems: |
|
|
|
|
At least once annually, lifelong: orthopedic examination for joint hypermobility, contractures, scoliosis, kyphosis, lordosis. |
Joint hypermobility |
Yes |
Yes |
|
90 |
|
Joint contractures |
Yes |
Yes |
Yes |
50 |
|
Radio-Ulnar Synostosis |
Yes |
Yes |
Yes |
20 |
|
Kyphosis |
|
|
Yes |
20 |
|
Scoliosis |
|
Yes |
Yes |
18 |
|
Lordosis |
|
Yes |
Yes |
40 |
|
Pathological gait |
|
Yes |
Yes |
60 |
|
Calcium homeostasis and vitamin D: |
|
|
|
|
Serum calcium levels: once every 4 months up to 2 years of age, once every 2 years thereafter (urinelevels only if necessary). Consultation on nutrition and dietary calcium intake; dietary calcium corrections are made only under physician supervision and never by parents alone! |
Hypercalcemia |
Yes |
|
Yes |
15—45 |
|
Hypercalciuria |
Yes |
Yes |
Yes |
30 |
|
Vitamin D hypervitaminosis |
|||||
Endocrine problems: |
|
|
|
|
Strict follow—up of TSH levels (+FT3, FT4) once annually up to 3 years of age; thereafter once in 12to 24 months lifelong (no TAT and MAT measurement necessary - the hypothyroidism is caused bygland hypo-/aplasia). |
Hypothyroidism |
Yes |
Yes |
Yes |
5—10 |
|
Early (but not precocious) puberty |
|
Yes |
Yes |
20 |
|
Diabetes mellitus |
|
|
Yes |
15 |
|
Obesity |
|
Yes |
Yes |
30 |
|
Neurological problems: |
|
|
|
|
Thorough neurological examination once annually for signs of muscle hypotension, hypertension,cerebe1lar symptoms. Head MRI if Chiari is suspected. |
Hyperactive tendon reflexes |
|
Yes |
Yes |
75 |
|
Chiari type I malformation (caudal retraction of the cerebellar tonsils through the foramen magnum) |
Yes |
Yes |
Yes |
10 |
|
Central muscular hypotension |
|
Yes |
- |
80 |
|
Peripheral muscular hypertension |
Yes |
Yes |
Yes |
50 |
|
Cognitive and developmental problems: |
|
|
|
|
Physical monitoring according to the age-adapted WBS nomograms for height, weight and head circumference at each visit by physician up to 5 years of age and once annually thereafter until adolescence. |
Motor and physical developmental delay |
Yes |
Yes |
- |
95 |
|
Intellectual impairment (normal intelligence in up to 5%) |
|
Yes |
Yes |
75 |
|
Visuospatial cognitive impairment |
|
Yes |
Yes |
95 |
|
Behavioral features: |
|
|
|
|
Evaluation by psychologist/psychiatrist, symptomatic therapy if necessary (fear, depression, hyperactivity). Training in social skills. |
Attention Deficit Hyperactivity Disorder (ADHD) |
|
Yes |
|
65 |
|
Anxiety disorder (specific phobias, generalized anxiety) |
|
Yes |
Yes |
70 |
|
Sleep disorders |
|
Yes |
Yes |
65 |
|
Table 2: Summary of WBS clinical features and recommendations for follow-up of patients with Williams-Beuren syr+drome at different ages, as recommended by the American Academy of Pediatrics [2,7,16].
Figure 1: Characteristic facial features in Williams-Beuren syndrome (see text explanations). [13]
Tables at a glance
Figures at a glance