Rare Presentation of Adenoid Cystic Carcinoma in the Lung
Received Date: October 13, 2023 Accepted Date: November 13, 2023 Published Date: November 16, 2023
doi: 10.17303/jcrto.2023.11.204
Citation: Srutdi Kamalam Natarajan, Arthi M, Priyathersini Nagarajan (2023) Rare Presentation of Adenoid Cystic Carcinoma in the Lung. J Cancer Res Therap Oncol 11: 1-8
Abstract
Adenoid cystic carcinoma is a malignant neoplasm often arising from the salivary glands and is quite unlikely to present as a primary lung tumor. Hence, when a presentation seems out of the ordinary, one should be able to identify the possibility of this diagnosis. Herein we have a case of a 50-year-old female with a primary adenoid cystic carcinoma of the lung
Radiological evaluation showed no evidence of any primary in the salivary glands or breasts. She underwent a right lower lobectomy, and the specimen obtained was sent for histopathological examination. Based on her history and presentation, she was suspected to have an adenocarcinoma of the lung. However, histopathological examination showed a characteristic adenoid cystic carcinoma with a sieve-like or cribriform pattern along with an infiltrative nature, and immunohistochemistry helped finalize the diagnosis. This particular case was selected because it is highly unusual, and it is crucial to realize that presentations of this nature can also occur.
Keywords: Lung Tumor; Adenoid Cystic Carcinoma; Immunohistochemistry; Histopathology
Introduction
Lung cancer is one of the most commonly diagnosed cancers in the world, contributing to about 11.6% of the total cases [1]. In India, lung cancer accounts for about 5.9% of all cancers and 8.1% of all cancer-related deaths. Among all lung cancers, salivary gland tumors arising primarily from the lung are largely unusual. Nonetheless, a pulmonary presentation still accounts for about 0.04 to 0.2% of all lung cancers [2] and has low malignant potential. Since it is considered a low-grade malignancy, it tends to be slow-- growing and has a protracted clinical course. Owing to its rarity, diagnostic and therapeutic challenges often arise given that the signs and symptoms resemble other common conditions. There are no specific risk factors implicated in the pathogenesis of the condition which makes it difficult to identify groups at risk. The initial clinical picture is vague and does not contribute to the confirmation of the diagnosis. The location of the tumors is often central, as they arise from the central bronchi, and rarely peripheral [3]. Radiological imaging modalities help in the localization of the tumor. The use of PET/CT helps distinguish primary adenoid cystic carcinoma of the lung from a secondary tumor that has spread from another site, which is crucial for accurate diagnosis. The diagnosis is also chiefly based on histopathological studies, with significant emphasis on immunohistochemistry. Surgery remains the mainstay of management, with poor evidence of efficacy in terms of the role of chemoradiation and its impact on survival.
Case
A 50-year-old female known to have been hypertensive for five years presented with complaints of hemoptysis for one month and a non-productive cough over a period of five years. She has no other known comorbidities and no significant family or personal history. PET/CT revealed an FDG-avid multilobulated soft tissue density lesion in the anterior basal segment of the lower lobe of the right lung with no infiltration into the pleura or mediastinum (Figure 1). The ability to differentiate primary tumors from secondary metastasis using 18F-FDG PET/CT is useful in guiding clinical decision-making along with the evaluation of clinicopathological features. Based on her history and presentation, she was suspected to have an adenocarcinoma of the lung. She underwent a right lower lobectomy, and the specimen obtained was sent for histopathological examination. When examined grossly, the specimen showed a well-defined, solid, firm globular mass measuring about 8x6x3 cm infiltrating into the adjacent lung parenchyma. The dissection of the mass displayed a gray-white appearance with no areas of hemorrhage or necrosis (Figure 2). Microscopy showed moderately differentiated cells with a characteristic sieve-like or cribriform pattern with inner ductal and outer myoepithelial cells (Figures 3, 4, and 5). Immunohistochemistry was done, and tumor markers CD117 showed membrane positivity (Figure 6) and a Ki67 proliferation index of less than 5% (Figure 7). Diagnosis of primary adenoid cystic carcinoma of the lung was made. The tumor was staged as T2N0M0. The patient tolerated the surgery well, and postoperative follow-up was done annually, was uneventful, and showed no evidence of recurrence or metastasis (Figures 8 and 9).
Discussion
Adenoid cystic carcinoma frequently develops from the salivary glands and, through a perineural invasion, spreads to lymph nodes and may metastasize to the lung. It rarely grows from other sites like the breast, female reproductive tract, the prostate in males, skin, and lungs. Pulmonary ACC is a slow-growing neoplasm with an indolent clinical course, and despite arising from the lung as a primary tumor, morphologically it is similar to tumors developing from the salivary glands. Most cases exhibit peripheral nerve invasion and often extend into the submucosa.
These tumors usually occur during adulthood, but some forms of the condition are reported among children. The majority of cases occur in the fifth decade of life, with a slight male preponderance. In this case, the subject was a 50-year-old female with no comorbidities.
Patients initially present with non-specific symptoms, most commonly cough, shortness of breath, wheezing, or hemoptysis [4], which results in a delayed diagnosis, as seen in this case where the patient had a non-productive cough for a period of five years. The location of the tumor and distal obstruction are some factors that determine the clinical presentation.
Furthermore, because of its atypical clinical manifestations, early ACCL is hard to differentiate from common respiratory diseases like asthma and chronic obstructive pulmonary disease. Smoking or any other risk factor is not specifically implicated in the pathogenesis of this tumor which makes identifying groups at risk difficult [5].
Radiological examinations do not reveal any characteristic features but help with the identification and localization of the growth. FDG PET/CT provides the advantage of distinguishing a primary growth from a secondary metastatic tumor from elsewhere in the body, commonly from the salivary gland or breasts [6]. Histopathology and immunohistochemistry play a major role in the confirmation of a diagnosis. Commonly identified histopathological forms of the tumor include cribriform, tubular, and solid patterns of which a solid pattern has the worst prognosis and higher risk of metastasis. In this case, microscopy revealed a cribriform pattern. Surgical resection is the most effective intervention [7] in cases of such primary lung tumors. The type of surgery done depends on the stage of the disease. In cases of primary lung tumors with good resectability and no metastasis, surgical management, either a pneumonectomy or lobectomy with or without chemotherapy, is indicated. Surgery may not be beneficial in cases of advanced disease. The role of radiotherapy is not well defined, however, can be reserved for those with unresectable tumors or who cannot tolerate surgery. However, radiation therapy has no known effect on the overall survival rates. Research on other treatment modalities is expanding significantly with advancements in the field of molecular pathology, primarily concentrating on molecular targets.
Adenoid cystic carcinoma of the lung is considered a low-grade malignancy, and hence, long-term survival is assured. However, recurrence after 10 or more years is not uncommon, and close follow-up is required.
Conclusion
Despite the rarity of the tumor,it is crucial to recognize primary adenoid cystic carcinoma of the lung to prevent misdiagnosis. It may be mistaken as a benign condition based on microscopy and hence immuno-histochemistry is crucial in establishing the correct diagnosis. Even though recurrence is possible, long-term survival is usually guaranteed. The prognosis depends on factors like age, tumor size, tumor staging, prevailing histological pattern and surgical margin status.
- F Bray, J Ferlay, I Soerjomataram, RL Siegel, LA Torre, A Jemal (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin 68: 394-424
- Hu MM, Hu Y, He JB, Li BL (2015) Primary adenoid cystic carcinoma of the lung: Clinicopathological features, treatment and results. Oncol Lett 9: 1475-81.
- Multiple primary lung cancer comprised of adenocarcinoma and adenoid cystic carcinoma (2022) A case report. Translational Cancer Research 11: 591-6.
- Moran CA, Suster S, Koss MN (1994) Primary adenoid cystic carcinoma of the lung. A clinicopathologic and immunohistochemical study of 16 cases. Cancer 73: 1390-7.
- Sun X, Gu W, Yuan H, Wang S, Yang Y et al. (2022) Clinical use of 18F-FDG PET/CT in the differential diagnosis of patients with primary and secondary adenoid cystic carcinoma of the lung: a retrospective cohort study. Translational Lung Cancer Research 11: 1643-56.
- Iqbal MS, Aslam S (2016) Primary Adenoid Cystic Carcinoma of Lung - An Overview. Clin Oncol 1: 1158.
- Kitada M, Ozawa K, Sato K, Hayashi S, Tokusashi Y et al. (2010) Adenoid cystic carcinoma of the peripheral lung: acase report. World J Surg Oncol 8: 74.
FIGURE 1
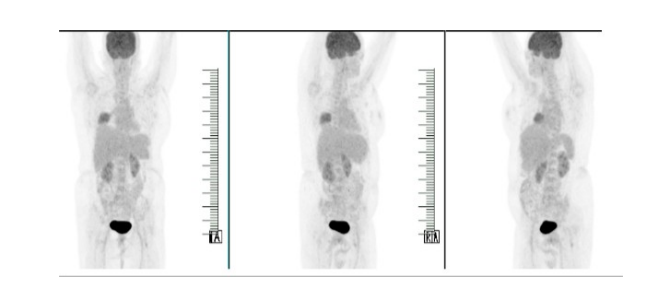
Figure 1: PET-CT done in 2019 at the time of presentation
FIGURE 2
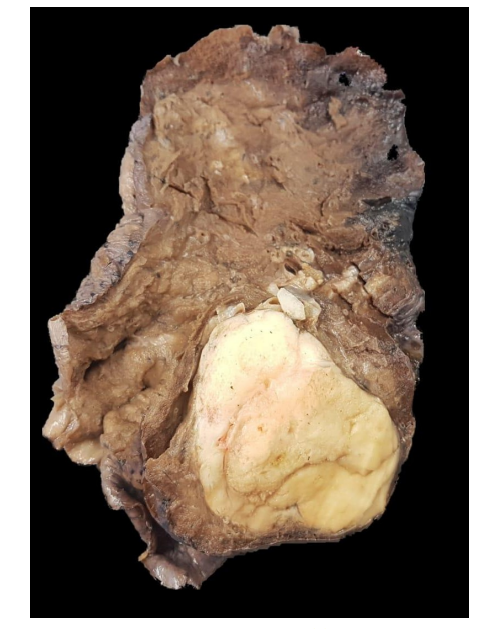
Figure 2: Gross specimen post lobectomy
FIGURE 3
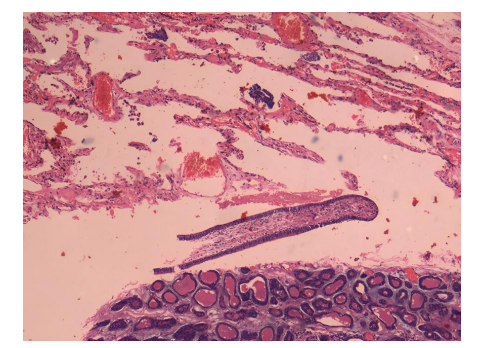
Figure 3: Low power view showing lung parenchyma with the attached tumor
FIGURE 4
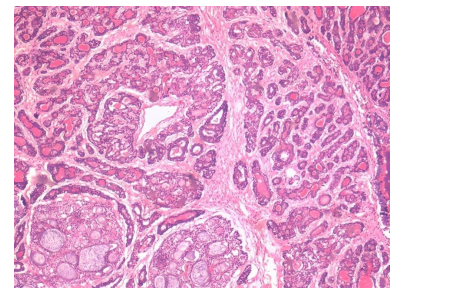
Figure 4: 200 x Tumor cells showing cribriform pattern composed of inner ductal and outer myoepithelial cells
FIGURE 5
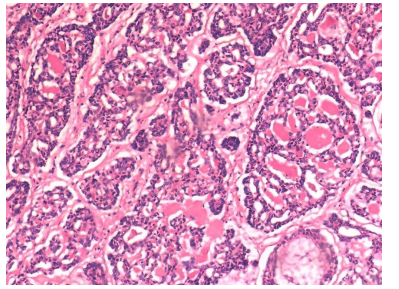
Figure 5: 400 x showing higher power view of tumor cells confirming the adenoid cystic tumor
FIGURE 6
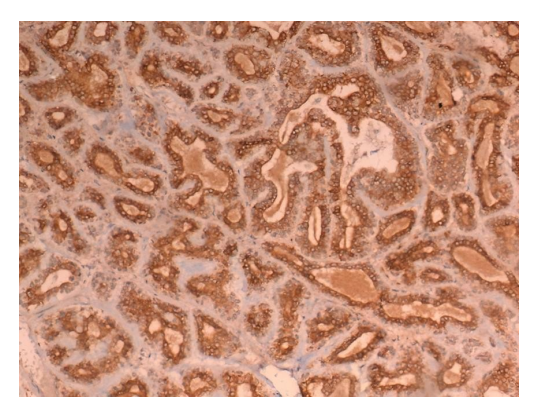
Figure 6: IHC for CD117 confirms the diagnosis of adenoid cystic carcinoma
FIGURE 7
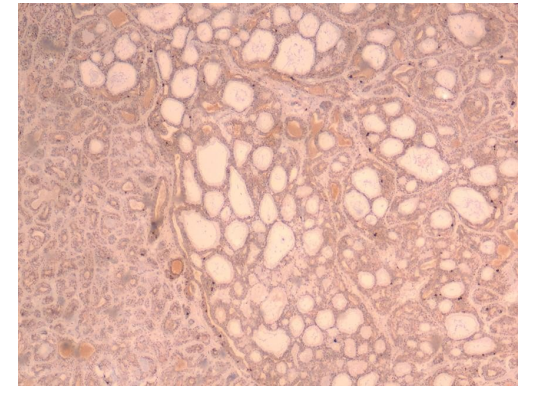
Figure 7: IHC for Ki67 proliferation index less than 2%
FIGURE 8
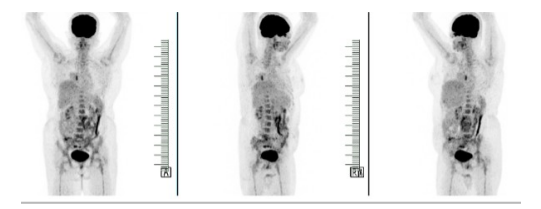
Figure 8: PET-CT done in 2020 during annual follow-up: Focal non FDG avid air space opacity noted in the right perihilar region,FDG avid foci are seen in the right lower lobe lobectomy stump
FIGURE 9
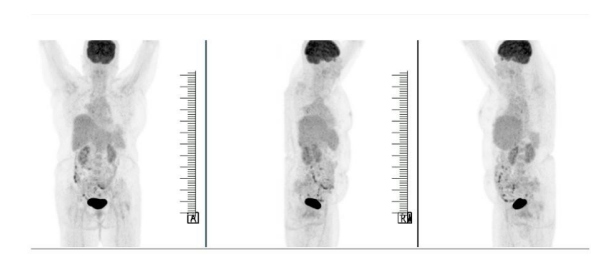
Figure 9: PET-CT done in 2021: No recurrence/metastasis
Figures at a glance