Single-use-Duodenoscopes: A Failure Concept in Times of Need
Received Date: December 08, 2023 Accepted Date: January 08, 2024 Published Date: January 10, 2024
doi: 10.17303/jcrto.2024.12.101
Citation: Carl C. Schimanski, Zeynep Babacan, Christian Friedrich (2024) Single-use-Duodenoscopes: A Failure Concept in Times of Need. J Cancer Res Therap Oncol 12: 1-8
Abstract
Background: Singe-use endoscopes have been used for cholangioscopy for over a decade. Two different single-use-duodenoscope were launched within the recent 3 years. We established a single-use-duodenoscopy system in June 2022 as a failure concept and for treatment of patients harboring multi-resistant organisms at a tertiary care center in Darmstadt, Hessia, Germany. Due to a technical malfunction we relied on the pre-established failure concept over a period of 13 days in 2023.
Methods: patients who had received an ERCP by single-use-duodenoscopes between February 22nd and March 6th 2023 due to a malfunction of the hospital endoscope washer disinfector (ETD) system were identified and analyzed. We report on patient characteristics, ASGE grades, indication, interventional success and adverse events of ERCPs.
Results: 18 emergency or urgent ERCPs by the use of single-use-duodenoscopes had been performed within 13 days. ASGE grades were 1 (16.6%), 2 (26.6%), 3 (43.8%) and 4 (27.8%), respectively. Success rates for diagnostic and therapeutic interventions were: stent removal 100% (10/10), cannulation and positive cholangiogram 89% (16/18), stone extraction (> 10 mm) by lithotripter basket 100% (7/7), baby-in-mother cholangioscopy (83%; 5/6), electrohydraulic lithotripsy 100% (3/3), bile duct biopsy 100% (2/2). No related adverse events were observed.
Summary: Single-use-duodenoscopy seems feasible as a failure concept even in ASGE grade 3 and 4 procedures.
Keywords: Duodenoscopes; Cholangioscopy; Endoscope; Electrohydraulic Lithotripsy
Introduction
Reusable endoscopes are a standard-of-care in medicine. Modern endoscope washer disinfector (ETD) systems provide a solid processing of endoscopes after diagnostic or interventional procedures [1]. In spite of careful desinfection of duodenoscopes, the contamination rate of reprocessed duodenoscopes is 15.25% according to a current meta-analysis by Larsen S et al [2]. A series of publications revealed the risk of transmitting multi-resistant bacteria into the bile duct system resulting in severe and difficult to treat infections [3,4]. The overall mortality linked to ERCP is about 0.3% [5]. Mortality rates linked to contaminated duodenoscopes are rarely published, therefore underreported and most likely underestimated [3]. The risk of multi-resistant infections has led to new recommendations concerning the architecture and processing of duodenoscopes [6]. Therefore, single-use-duodenoscopes are recommended in the case of MRE, MRSA and VRE colonization or infection of the bile duct system. Furthermore, patients with suspected or proven prion disease should be treated with single-use-endoscopes, as decontamination is difficult, expensive and challenging to the endoscopic material [7].
ERCP is an important diagnostic and interventional technique, not only in tertiary care centers. Being the only tertiary care center in southern Hessia and the coordinating hospital of the region, we had decided to invest in a failure concept in 2022 in order to secure ERCP in patients harboring multi-resistant organisms and in the case of technical malfunction of endoscopes, processors or the hospital endoscope washer disinfector (ETD) system. Due to a longer lasting malfunction of the ETD system between February 22nd and March 6th 2023 we unexpectedly relied on performing ERCPs with single-use-duodenoscopes. We retrospectively identified all patients who had received an ERCP by single-use-duodenoscopes and report on patient characteristics, indication, interventional success, ASGE grades and adverse events in order to describe our novel experience of single-use-duodenoscopes as failure concept.
Methods
Study Design and Inclusion Criteria
This research was a retrospective, monocentric study involving the tertiary care center Municipal Hospital Darmstadt, Hessia, Germany. We analyzed all consecutive patients who underwent diagnostic or interventional ERCP with the single-use “Ambu aScope Duodeno” duodenoscope and Ambu aBox Duodeno processor between February 22nd and March 6th 2023 due to a defect of the hospital ETD system, specifically a leakage of the ETD water supply line with consecutive germ colonization. The electronic chart review was performed in order to collect captured variables. The study received institutional ethic board approval (nr. 2023-3418-evBO).
Procedures
According to our standard procedures written informed consent was obtained from all patients prior to the procedure. For prophylaxis of post ERCP pancreatitis, patients received 100 mg diclofenac suppository 30 minutes before ERCP. The endoscopic procedures were performed by two senior endoscopists (ERCP lifetime experience > N=2000 procedures). A single-use sterile duodenoscope (Ambu aScope Duodeno, Ambu aBox Duodeno, Ambu A/S, 2750 Ballerup, Denmark) was used for diagnostic and interventional ERCP, respectively. Stent removal was conducted by a 15 mm asymmetric polypectomy snare (MTW Endoskopie W. Haag, 46487 Wesel, Germany). Duct intubation and papillotomy were performed with a sphincterotome SU (Endoflex GmbH,46562 Voerde, Germany). For intubation and guided intervention, a 0.025-inch 260 cm Jagwire Straight tip high performance guidewire (Boston Scientific, Marlborough, MA 01752, USA) was used. Bile duct stones were removed with a 30 mm lithotripter basket (Fujifilm Medwork GmbH, 91315 Hochstadt, Germany). If indicated, a single-use cholangioscope (SpyScope DS II, Spyglass DS Direct visualization system, Boston Scientific, Marlborough, MA 01752, USA, respectively) was used. Bile duct biopsies were taken with SpyBiteMax forceps (Boston Scientific, Marlborough, MA 01752, USA). Electrohydraulic lithotripsy was performed with a biliary electrohydraulic lithotripter probe and the Autolith Touch generator (Boston Scientific, Marlborough, MA 01752, USA, respectively). If indicated, patients received a 50/70 or 90 mm straight PTFE stent preplaced on a introducer system (MTW Endoskopie W. Haag, 46487 Wesel, Germany).
Definitions and Outcomes
The primary outcome was technical success, defined as successful diagnostic cholangiogram (a) papillotomy (b), stone removal (c) stenting (d) cholangioscopy. The secondary outcome was the analysis of recorded adverse effects.
Results
Baseline Characteristics
Between February 22nd and march 6th 2023 a total of 18 ERCP were performed by use of single-use-duodenoscopes. Patient age ranged from 37 to 84 years, the average age was 69.3 years. 12 patients (66.6%) were females and 6 patients males. Indications for ERCP were bile duct stones (N=10; pre-verified by oral EUS), suspected extrahepatic cholangiocellular cancer (N=4), suspected DHC leakage (N=1), stenosis of the pancreatic duct (N=1), sclerosis of the papilla (N=1) and sludge of the common bile duct (N=1).
Clinical Outcomes
One ERC (double duct sign, 1/18, 5.5%) was diagnostic, while 17 out 18 (94.5%) had a therapeutic approach. ASGE grades were 1 (16.6%), 2 (26.6%), 3 (43.8%) and 4 (27.8%).
8 patients had already undergone a papillotomy prior to the current ERCP. Cannulation of the papilla Vaterii and the common bile duct was successful in 16 out of 18 cases (89%), papillotomy in 8 of 8 cases (100%) and stone removal by lithotripter basket in 7 of 7 cases (100%). Stent implantation was successfully performed in 12 of 13 (92.3%) of intended patients. Failure of intubation and stenting was due the rigidity of the single-use-duodenoscope tip according to the endoscopist, respectively.
6 patients had been scheduled for single-use cholangioscopy due to cholangiocellular carcinoma (N=2) or complex bile duct stones (N=4). Cholangioscopy was successfully performed in 5 out of those 6 patients. In 3 patients with choledocholithiasis, complex bile ducts stones were resolved by electrohydraulic lithotripsy prior to stent implantation. In one patient with a complex bile duct stones cholangioscope intubation of the common bile duct failed due to the rigidity of the endoscope tip according to the endoscopist. In two patients with a suspected extrahepatic cholangiocellular carcinoma intracanalicular biopsies were gathered by cholangioscopic biopsy, prior to successful stenting of the common bile duct bridging the tumor mass.
Adverse Events
No procedure derived adverse events were documented.
Discussion
This monocentric, retrospective study demonstrated the effective and safe use of a novel single-use-duodenoscope for ERCP.
Reusable endoscopes are used in endoscopy units worldwide. Although decontamination and processing after their use is standardized, the specific architecture of duodenoscopes bears the risk of transmitting germs from one patient to another [3,4]. As the bile duct system is sterile, contamination implicates the risk of biliary infections, such as cholangitis or sepsis, which can be particularly difficult to treat and dangerous in the case of multi-resistant organisms or prion disease. Therefore, the use of single-use-duodenoscopes can be economically and ecologically justified in these specific situations.
The municipal hospital of Darmstadt (Klinikum Darmstadt GmbH, Darmstadt, Germany) is the only tertiary care center of southern Hessia, caring for a population of 1.5 million citizens. In summer 2022 we had established a failure concept for ERCP by introducing the Ambu aScope Duodeno single-use endoscope and the respective Ambu aBox Duodeno processor allowing us to bridge malfunction of the endoscope washer disinfector or to treat patients harboring the risk of transmitting multi-resistant organisms. European market access of the Ambu aBox and aScope Duodeno was October 2021 and the system had already been pretested by our institution in December 2021.
Due to a malfunction of the hospital endoscope washer disinfector (ETD) system we were dependent on single-use-endoscopes over a period of 13 days. During this period, we performed 18 ERCPs by use of single-use-duodenoscopes.
The success rates were as follows: stent removal (10/10; 100%), bile duct cannulation and positive cholangiogramm (16/18; 89%), papillotomy (8/8; 100%), stone removal via lithotripter basket (7/7; 100%) and stenting (12/13; 92.3%). Our overall completion rate was 89% and was thus in line with data generated by two trials [8,9] applicating the Ambu aScope Duodeno (84% and 98%, respectively). In addition our overall completion rate was matching the data generated in 3 prospective trials performed with the single-use-duodenoscope Exalt Model D (96.7%, 88.5% and 95%, respectively) (Boston Scientific Corporation, Marlborough, MA, USA) [10-13]. Noteworthy, the amount of ASGE grade 3 and 4 ERCPs was high among our patients as compared to above cited studies due to nature of indication.
Bang J et al. reported on a similar product (Exalt Model D, Boston Scientific Corporation, Marlborough, MA, USA) used in a prospective, randomized trial comparing single-use versus reusable duodenoscopes in ERCP. 98 patients with low-complexity procedures underwent ERCP within this trial 10). The median number of attempts for successful cannulation was surprisingly significantly lower for the single-use cohort, however the ease of passage in to the stomach, image quality and image stability were significantly worse in the single-use cohort. No significant difference for cannulation success was found between single-use and reusable endoscopes (95.8% vs. 100%), also being in line with our own experience with the Ambu aScope Duodeno in patients with a complex ERCP (89%; >70% ASGE 3 and 4).
Napoleon B et al. reported on a single-use-duodenoscope tested in a prospective multi-center trial in France. 64 patients underwent ERCP (58.3% ASGE 2, 35% ASGE 3); 95% of procedures were completed using the single-use-duodenoscope [14]. In another single-center trial with a higher complexity (ASGE 3 and 4 in 51.9%) procedures completion using the Exalt Model D was only 90.4% (13). Adverse events occurred in 0-5% of trials, paralleling our own data [13,14].
In addition, we performed a smaller series of single-use mother-in-baby cholangioscopies with adequate technical success rates (5/6; 83%). The parallel use of both single use endoscopes (duodenoscope and cholangioscope) resulted in successful electrohydraulic lithotripsy and intracanalicular biopsies, respectively. Therefore, it also seems feasible in selected patients. Only one international, multicenter, retrospective trial did analyze the combination of both single-use endoscope in a total of 66 patients, so far, reporting a technical success rate of 98.5% and a high user satisfaction score somewhat paralleling our experience [15].
Noteworthy, the endoscopic procedures were performed by senior endoscopists, with an ERCP lifetime experience ≥ 2000 procedures. Therefore, the reported success rates could be distorting not matching the reality in other, smaller endoscopy units. The unusual haptic feel, as well as the light weight of 700g and the specific procedural perception of the Ambu aScope Duodeno endoscope can initially be irritating and bothersome, potentially impacting on success rates. This personal experience is line with data published by the manufacturer himself, demonstrating a significant correlation of product usage and satisfaction indicating a learning curve when the endoscopy setup is being changed from reusable to single-use [16]. Increasing the weight of the Ambu aScope Duodeno endoscope mimicking the weight of a reusable duodenoscope might increase the endoscopist comfort.
A prospective, comparative study of the most prevalent reusable- and single-use-duodenoscopes concerning technical success parameters would be feasible and desirable.
In summary, we were able to demonstrate, that single-use-duodenoscopes may function as a failure concept for larger endoscopy units. However, due to economic (market price: 850 € per aScope Duodeno) and ecological reasons, the use of single-use endoscopes should be limited to selected emergency patients within a failure concept or patients harboring a risk of transmitting multi-resistant organisms.
Conclusion
Single-use-duodenoscopes demonstrate solid technical and clinical success rates. They help reducing the risk of biliary infections, which can be particularly difficult to treat and dangerous in the case of multi-resistant organisms or prion disease. In addition, they represent a solid failure concept.
Declaration of Interest Statement
None
- Leiss O, Beilenhoff U, Bader L, Jung M, Exner M (2002) Reprocessing of flexible endoscopes and endoscopic accessories - an international comparison of guidelines. Z Gastroenterol 40: 531-42.
- Larsen S, Russell RV, Ockert LK, Spanos S, Travis HS, Ehlers LH, Maerkedahl A (2020) Rate and impact of duodenoscope contamination: A systematic review and meta-analysis. E Clinical Medicine 25: 100451.
- Rubin ZA, Kim S, Thaker AM, Muthusamy VR (2018) Safely reprocessing duodenoscopes: current evidence and future directions. Lancet Gastroenterol Hepatol. 3: 499-508.
- Rupp C, Bode K, Weiss KH, Rudolph G, Bergemann J et al. (2016) Microbiological Assessment of Bile and Corresponding Antibiotic Treatment: A Strobe-Compliant Observational Study of 1401 Endoscopic Retrograde Cholangiographies. Medicine (Baltimore) 95: e2390.
- ASGE Standards of Practice Committee; Anderson MA, Fisher L, Jain R, Evans JA, Appalaneni V (2012) Complications of ERCP. Gastrointest Endosc 75: 467-73.
- Beilenhoff U, Biering H, Blum R, Brljak J, Cimbro M et al. (2017) Prevention of multidrug-resistant infections from contaminated duodenoscopes: Position Statement of the European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Gastroenterology Nurses and Associates (ESGENA). Endoscopy 49: 1098-106.
- Kampf G, Jung M, Suchomel M, Saliou P, Griffiths H, Vos MC (2020) Prion disease and recommended procedures for flexible endoscope reprocessing - a review of policies worldwide and proposal for a simplified approach. J Hosp Infect 104: 92-110.
- Bhenswala P, Andalib I, Gress F (2021) Preliminary clinical evaluation of a novel single use duodenoscope: a single center experience. Am J Gastroenterol 116: S481.
- Ambu. Ambu announces interim 60-patient clinical trial results for aScope Duodeno 1.5 showing 98.3% procedure success rate
- Bang JY, Hawes R, Varadarajulu S (2021) Equivalent performance of single-use and reusable duodenoscopes in a randomised trial. Gut 70: 838-44
- Muthusamy VR, Bruno MJ, Kozarek RA, Petersen BT, Pleskow DK et al. Clinical Evaluation of a Single-use-Duodenoscope for Endoscopic Retrograde Cholangiopancreatography. Clin Gastroenterol.
- Slivka A, Ross AS, Sejpal DV, Petersen BT, Bruno MJ et al. (2021) EXALT Single-use-Duodenoscope Study Group. Single-use-duodenoscope for ERCP performed by endoscopists with a range of experience in procedures of variable complexity. Gastrointest Endosc. 94: 1046-55.
- Persyn D, Malenstein HV, Vanderschueren E, Schuermans A, Dreesen M et al. (2022) Performance and applicability of a first generation single-use-duodenoscope: a single-center cohort study. Ann Gastroenterol 35: 368-75.
- Napoléon B, Gonzalez JM, Grandval P, Lisotti A, Laquière AE et al. (2022) Evaluation of the performances of a single-use-duodenoscope: Prospective multi-center national study. Dig Endosc 34: 215-21.
- Fugazza A, Colombo M, Kahaleh M, Muthusamy VR, Benjamin B et al. (2023) The outcomes and safety of patients undergoing endoscopic retrograde cholangiopancreatography combining a single-use cholangioscope and a single-use-duodenoscope: A multicenter retrospective international study. Hepatobiliary Pancreat Dis Int 11: S1499-3872(23)00047-4.
- Martos-Pereira I. User evaluation on AMBU aScope Duodeno – an analysis based on 505 user evaluations of Ambu aScope Duodeno used for ERCP procedures.
FIGURE 1
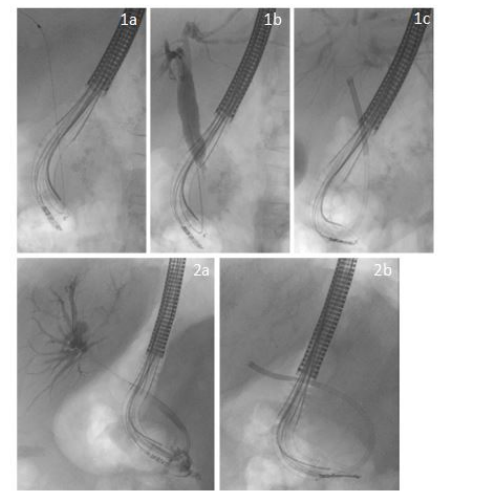
Figure 1: 1a-c representing the case of a patient with a distal cholangiocellular carcinoma depicting wire cannulation (a) positive cholangiogram (b) cholangioscopy (c) 2a-b representing a case of a patient with Klatskin III cancer depicting the positive cholangigramm (2a) and cholangioscopy (2b)
Tables at a glance
Figures at a glance