A Case Report of Long-Term Survival in Small Cell Lung Cancer Following Multiline Therapy
Received Date: March 03, 2024 Accepted Date: April 03, 2024 Published Date: April 06, 2024
doi: 10.17303/jcrto.2024.12.102
Citation: Wan Guang zhi (2024) A Case Report of Long-Term Survival in Small Cell Lung Cancer Following Multiline Therapy. J Cancer Res Therap Oncol 12: 1-9
Abstract
Small cell lung cancer (SCLC) represents a highly malignant form of lung cancer, characterized by its notable mortality. Recent phase III clinical trials, specifically Impower133 and CASPIAN studies, have resulted in the approval of atezolizumab and durvalumab in combination with chemotherapy as the first-line therapeutic approach for extensive-stage SCLC. However, the observed improvement in median overall survival (OS) from these trials was modest, with an approximate increase of only 2 months. Furthermore, patients who experience disease progression following first-line therapy face limited treatment options and exhibit poor survival outcomes. We aimed to investigate the potential benefits of individualized treatment strategies in SCLC by presenting a case study highlighting long-term survival achieved through the application of multiple lines of therapy. Furthermore, a thorough review of existing literature is conducted to elucidate the role of personalized treatment approaches in maximizing survival outcomes for patients with SCLC.
Keywords: Small Cell Lung Cancer; lung Cancer; Chemotherapy; Computed Tomography
Case Presentation
A 56-year-old male patient presented with a persistent cough and underwent chest computed tomography (CT), which revealed the presence a pulmonary mass. Subsequent positron emission tomography (PET)-CT scan indicated that the left hilar space was occupied by lung cancer, accompanied by obstructive inflammation and mediastinal lymph node metastasis (Figure 1A). Pathologic analysis of specimens obtained through electronic bronchoscopy biopsy confirmed the presence of small cell carcinoma nests infiltrating the bronchial mucosa in the left upper lung, consistent with small cell carcinoma (Figure 1B). Immunohistochemical staining, including CD56 (++), thyroid transcription factor-1 (TTF-1, ++), SCLC, ++), further supported the diagnosis of SCLC for the observed lesion.
The patient then received six cycles of lopressor/- cisplatin + etoposide (EP) chemotherapy. Follow-up chest CT conducted on February 27th, 2013, exhibited a significant reduction in the size of the left hilar mass and mediastinal lymph nodes, indicating a partial response (PR) to the treatment (Figure 2). After 3 cycles of chemotherapy by March 21st, 2013, the patient received concurrent radiation therapy comprising 25 sessions to target the lung cancer and enlarged mediastinal lymph nodes, with a cumulative radiation dose of 50 Gy.. The chemotherapy regimen was completed by June 2013. Notably, the patient experienced grade IV myelosuppression during chemotherapy, necessitating supportive treatment to stimulate erythropoiesis, leukocyte production, and platelet production. As a prophylactic measure, brain irradiation was administered in September 2013.
On April 22nd, 2014, a follow-up PET-CT scan revealed a small mass in the left lung, which was determined to be a stable lesion following radiotherapy. However, a thoracoabdominal CT scan with contrast conducted on October 20th, 2014, identified the presence of a left adrenal tumor, indicating disease progression (PD) (Figure 3A). Consequently, the patient received a cycle of EP chemotherapy on October 22nd, 2014. Due to a myocardial infarction, radiotherapy was chosen as an alternative to chemotherapy for treating the left adrenal metastasis. Subsequent imaging on March 31st, 2015, demonstrated a significant reduction in the size of the left adrenal metastasis (Figure 3B).
During a chest CT scan performed on October 16th, 2017, new left supraclavicular lymph node metastasis was observed (Figure 3C). From October to November 2017, radiotherapy was administered to target the metastatic lymph node foci in the left supraclavicular region. Notably, a follow-up chest CT on March 13th, 2018, indicated a notable decrease in the size of the left supraclavicular lymph node (Figure 3D). A PET-CT scan on August 16th, 2017, revealed periaortic lymph node metastasis (Figure 3E), prompting the patient to receive radio-wave knife radiotherapy. Furthermore, abdominal magnetic resonance imaging (MRI) conducted on September 20th, 2018, unveiled the presence of multiple round-like shadows in the liver parenchyma, characterized by slightly prolonged T1 and T2 signals. The larger shadow, measuring 1.3×1.0 cm on limited diffusion weighted imaging (DWI), indicated the presence of multiple intrahepatic foci highly suggestive of metastasis (Figure 3F). In September and October 2018, the patient underwent hepatic artery perfusion chemoembolizations twice in the interventional unit, involving the administration of lopressor (20mg) and epirubicin hydrochloride (40mg).
A PET-CT scan conducted on December 18th, 2018, revealed increased size and metabolic activity in the right parietal, left parietal, and left parietal iliac vessel lymph nodes near the abdominal aorta (Figure 4A). The patient received four cycles of nivolumab immunotherapy between January and February 2019. Subsequent PET-CT imaging performed in June 2019 indicated a reduction in lesion size and decreased metabolic activity (Figure 4B).CT with contrast on December 11th, 2019 showed the enlarged lymph nodes around the hepatic hilum and anterior to the right renal vein and significantly enhancing soft tissue nodules under the right renal hilum, encompassing the right upper ureter, leading to dilated right hydronephrosis. These nodules were considered metastatic. Additional findings included stenosis of the superior branch vein of the right posterior lobe of the liver and uneven perfusion in the right lobe of the liver. The adrenal nodules, which were larger than before, were also considered to be metastases (Figure 5A, B). Subsequentially, oral anlotinib was initiated on January 17th, 2020. A follow-up abdominal CT on March 3rd, 2020 showed that the lesion under the right renal hilum decreased in size compared to previous scans, and the lymph nodes around the hilum showed no significant changes (Figures 5C, D).
Abdominal CT on May 28th, 2021 revealed that the left adrenal metastases increased compared to previous scans and were classified as PD (Figure 6A). Immunotherapy with durvalumab started in June 2021 every 3 weeks. The patient also underwent 6 cycles of EP chemotherapy every 4-5 weeks. After chemotherapy, the patient developed grade IV myelosuppression. However, this condition improved with leukocyte boosting therapy, and no significant gastrointestinal side effects were observed. After completing the 6 cycles of chemotherapy, the patient received immunotherapy with single- agent durvalumab. Stable disease was assessed by intermittent review during chemotherapy (Figure 6B).
Discussion
Small cell lung cancer is a group of highly aggressive neuroendocrine carcinomas that are poorly differentiated and account for about 15% of all lung cancers. Radiotherapy is the primary treatment majority for extensive-stage SCLC cases. According to the International Association for the Study of Lung Cancer, the 2-year overall survival (OS) rates of patients with stage I, II, III, and IV SCLC are approximately 73%, 54%, 23% and 8%, respectively [1]. A Spanish study [2] reported that approximately 20% of SCLC patients had brain metastases at diagnosis, and 96.7% of SCLC patients had metastatic lesions. The median OS was approximately 9.5 months, with 1- and 2-year survival rates of 38.9% and 14.8%, respectively. The combination of etoposide with platinum and topotecan has been the standard first- and second-line treatment for SCLC for over 3 decades. However, recent advancements have introduced immunotherapy, small molecule anti-angiogenic drugs, and new chemotherapeutic agents as first-line treatment options for SCLC.
Oligometastasis was first proposed by Hellman et al. in 1995. The metastasis of malignant tumors gradually evolves from local to systemic lesions, and oligometastasis represents a transitional stage with weak invasiveness, limited number of metastases and metastatic lesions, and specificity of metastatic organs. It does not have the tendency of systemic dissemination [3]. The majority of clinical studies define oligometastases as involving less than three metastatic organs and fewer than five metastatic foci. Oligometastases are further categorized into new oligometastatic disease and recurrent oligometastatic disease [5]. Concurrent oligometastasis is defined as a maximum interval of six months between the diagnosis of oligometastasis and the primary cancer, while heterochronous oligometastasis is defined as over an interval of six month between the diagnosis of oligometastasis and the primary cancer. Several previous studies have reported the benefit of local radiotherapy in progression-free survival (PFS) and OS with for patients with oligometastases. In the prospective phase II SABR-- COMET2 study, 99 patients with 1 to 5 oligometastases and unrestricted primary tumor types were enrolled. The study showed an improvement in PFS from 5.4 to 11.6 months and OS from 28 to 50 months. Local radiotherapy of the ymph nodes and adrenal glands was administered multiple times throughout the treatment for oligometastases, resulting in control of patient tumors and a survival benefit consistent with previous studies. Local radical treatment of patients with oligometastatic disease not only removes the lesions but also activates the body's anti-cancer immune response, producing more and stronger tumor-specific T lymphocytes [4-6].
Results of a meta-analysis [7] showed that the overall response rate of chemotherapy combined with immunotherapy in SCLC ranged from 33% to 68%, while the disease control rate was about 70% to 88%. Pembrolizumab, nivolumab, atezolizumab, and durvalumab have all been used as first-line treatment regimens, with studies indicating no significant differences [8]. The IFCT-1603, a phase II clinical trial, evaluated the efficacy of atezolizumab as second-line treatment of relapsed SCLC, demonstrated no survival benefit when compared to chemotherapy alone [9]. Rudin et al. [10] proposed the classification of SCLC in 2019 into four molecular subtypes based on gene mutations: achaete-scute homologue 1 (ASCL1), neurogenic differentiation factor 1 (NEUROD1), yes-associated protein 1 (YAP1) and POU class 2 homeobox 3 (POU2F3). The subtypes were labled SCLC-A, SCLC-N, SCLC-Y and SCLC-P, respectively, with SCLC-A being the most prevalent. Gay et al. found a type of SCLC that expressed the YAP1 protein, lacked ASCL1, NEUROD1 and POU2F3 gene mutations, and expressed multiple immune checkpoints, namely CD274 (PD-L1), PDCD1 (PD-1), and CTLA-4 along with their receptors. Therefore, this type of SCLC is referred to as SCLC-inflammatory (SCLC-I); SCLC-I tumors have high expression of CD8A and CD8B and a higher number of immune cell infiltrates surrounding the tumor. When Gay et al. [11] performed a subtype analysis of the population enrolled in IMpower133, they found that the SCLC-I population in the atezolizumab combination chemotherapy group had improved OS, suggesting that SCLC-I subtypes may have a greater chance of benefiting from treatment with immune checkpoint inhibitors (ICIs).
The CheckMate 331 study [12] suggested that second-line use of nivolumab did not improve OS in patients with relapsing SCLC. However, in the Chinese cohort, the median OS of patients in the nivolumab and chemotherapy groups was 11.5 and 7.0 months, respectively [hazard ratio (HR) = 0.70, 95% confidence interval (CI) 0.42-1.17, P = 0.03, and nivolumab reduced the risk of death by 30%. Further subgroup analysis of the Chinese cohort showed that both extensive- and limited-stage SCLC patients benefited from nivolumab treatment, whether it was used in the platinum-sensitive group, platinum-resistant group, or in different PD-L1 subgroups at baseline. In the global cohort, the objective response rates (ORRs) were 13.7% and 16.5% for nivolumab and chemotherapy, respectively, indicating that nivolumab was less efficient than chemotherapy. However, in the Chinese cohort, the efficiency of nivolumab was significantly better than that of chemotherapy, with ORRs of 20.6% and 4.7%, respectively. This disparity in data between the global and Chinese cohorts suggests that the efficacy of nivolumab may vary among different ethnic groups. Based on these findings, we gave patients second-line nivolumab monotherapy, resulting a prolonged PFS of 10 months and improvement in their quality of life. Once the immune system is activated and begins to attack tumor cells, this attack often lasts for a long time, and may even continue to take effect after discontinuing the medication. This is also an important reason why nivolumab can prolong the survival of patients. Once again, verify the persistence of immunotherapy.
SCLC is a highly vascularized tumor, and studies have demonstrated that the small molecule, multi-targeted anti-angiogenic drug anlotinib significantly improves PFS and OS in third- or above-line SCLC patients. This establishes anlotinib as the standard of care for post-line SCLC treatment. Anlotinib exerts a synergistic effect on tumors by modulating the tumor immune microenvironment and angiogenesis. The combination of anlotinib with sintilimab, used as third-line treatment, resulted in 15 months of PFS. This was much longer than the effect of anlotinib alone as third line treatment. This may be related to the fact that anlotinib inhibits tumor angiogenesis, reduces hypoxia and acidification within the tumor, improves the tumor microenvironment, thereby reducing the production of immunosuppressive factors and increasing immune cell infiltration and activity within the tumor.
Compared with PD-1 inhibitors, PD-L1 inhibitors bind to PD-L1 on both tumor cells and antigen-presenting cells. This leads to a stronger overall immune and restoration of T-cell-mediated anti-tumor immunity. PD-L1 inhibitors block the binding of PD-L1 on tumor cells to B7-1 on T cells, which helps in the full activation of T cells. In addition, inhibiting the binding of B7-1 molecules on dendritic cells to their highly expressed PD-L1 makes it difficult to bind CD28 to initiate immune activation. This reduces the self-inhibition of dendritic cells and further enhances the anti-tumor immune response. It is worth mentioning that PDL1 inhibitors do not interfere with the normal function of PD-L2. PD-L1 monoclonal antibodies block the binding of PD-L1 and PD-1, thereby preserving the function of PD-L2 in macrophages. This helps in avoiding side effects such as interstitial lung disease[13]. Given the long-term benefits of ICIs and the fact that the PD-1 and PD-L1 mechanisms are not exactly the same, PD-L1 inhibitors are associated with significantly fewer adverse effects. In this case, the patient was given durvalumab immune re-challenge, which led to another successful long period of PFS.
SCLC is highly aggressive, with a poor prognosis and short survival period. Therefore, accurately defining the pathological type and determining the tumor stage are crucial for effective management of SCLC. Chemotherapy combined with immunotherapy is the treatment option for ES-SCLC. However, for patients with relapsed progressive disease, there is a need for further evidence-based studies to establish maintenance treatment regimens following standard therapy. We anticipate the results of ongoing clinical studies involving novel immunotherapeutic agents and multi-drug combinations.
- 1.Nicholson AG, Chansky K, Crowley J, Beyruti R, Kubota K, Turrisi A, et al. (2016) The International Association for the Study of Lung Cancer Lung Cancer Staging Project: Proposals for the Revision of the Clinical and Pathologic Staging of Small Cell Lung Cancer in the Forthcoming Eighth Edition of the TNM Classification for Lung Cancer. J Thorac Oncol, 11: 300-11.
- Franco F, Carcereny E, Guirado M, Ortega AL, Lopez-- Castro R, Rodriguez-Abreu D, et al. (2021) Epidemiology, treatment, and survival in small cell lung cancer in Spain: Data from the Thoracic Tumor Registry. Plos One, 16: e251761.
- Weichselbaum RR, Hellman S (2011) Oligometastases revisited. Nat Rev Clin Oncol, 8: 378-82.
- Lhuillier C, Rudqvist NP, Elemento O, Formenti SC, Demaria S (2019) Radiation therapy and anti-tumor immunity: exposing immunogenic mutations to the immune system. Genome Med, 11: 40
- Liu C, Hu Q, Xu B, Hu X, Su H, Li Q, et al. (2019) Peripheral memory and naive T cells in non-small cell lung cancer patients with lung metastases undergoing stereotactic body radiotherapy: predictors of early tumor response. Cancer Cell Int, 19: 121.
- Liu C, Hu Q, Hu K, Su H, Shi F, Kong L, et al. (2019) Increased CD8+CD28+ T cells independently predict better early response to stereotactic ablative radiotherapy in patients with lung metastases from non-small cell lung cancer. J Transl Med, 17: 120.
- Ma X, Wang S, Zhang Y, Wei H, Yu J (2021) Efficacy and safety of immune checkpoint inhibitors (ICIs) in extensive-stage small cell lung cancer (SCLC). J Cancer Res Clin Oncol, 147: 593-606.
- Chen J, Wang J, Xu H (2021) Comparison of atezolizumab, durvalumab, pembrolizumab, and nivolumab as first-line treatment in patients with extensive-stage small cell lung cancer: A systematic review and network meta-analysis. Medicine (Baltimore), 100: e25180.
- Pujol JL, Greillier L, Audigier-Valette C, Moro-Sibilot D, Uwer L, Hureaux J, et al. (2019) A Randomized Non-Comparative Phase II Study of Anti-Programmed Cell Death-Ligand 1 Atezolizumab or Chemotherapy as Second-Line Therapy in Patients With Small Cell Lung Cancer: Results From the IFCT-1603 Trial. J Thorac Oncol, 14: 903-13.
- Rudin CM, Poirier JT, Byers LA, Dive C, Dowlati A, George J, et al. (2019) Molecular subtypes of small cell lung cancer: a synthesis of human and mouse model data. Nat Rev Cancer, 19: 289-97.
- Gay CM, Stewart CA, Park EM, Diao L, Groves SM, Heeke S, et al. (2021) Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell, 39: 346-60.
- Spigel DR, Vicente D, Ciuleanu TE, Gettinger S, Peters S, Horn L, et al. (2021) Second-line nivolumab in relapsed small-cell lung cancer: CheckMate 331(☆). Ann Oncol, 32: 631-41.
- Mayoux M, Roller A, Pulko V, Sammicheli S, Chen S, Sum E, et al. (2020) Dendritic cells dictate responses to PDL1 blockade cancer immunotherapy. Sci Transl Med, 12.
FIGURE 1
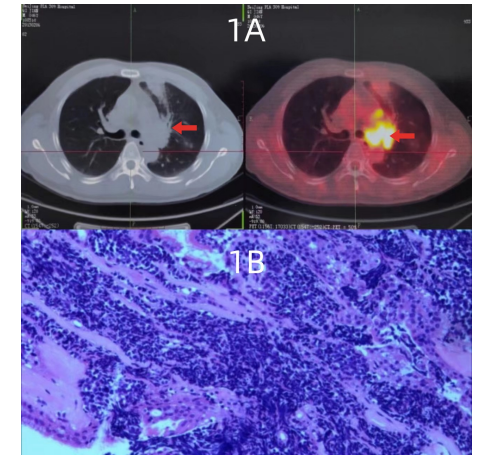
Figure 1: Baseline physical examination results of the patient at initial presentation. (A) PET-CT at initial examination indicated a hypermetabolic region, marked by a red arrow , which was considered malignant. (B) Pathological examination, HE staining of the puncture biopsy section showed malignant.
FIGURE 2
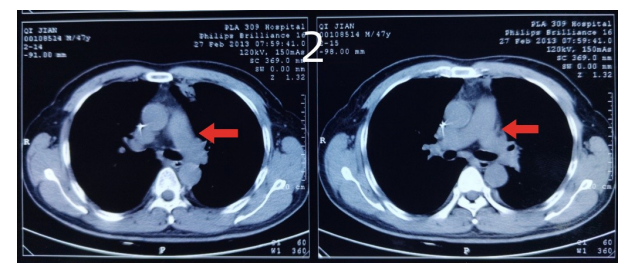
Figure 2: Treatment effect after one cycle of chemotherapy. The red arrows highlighted a significant reduction in the left hilar mass and mediastinal lymph nodes compared to the findings observed on PET-CT on February 6th, 2013 (partial response).
FIGURE 3
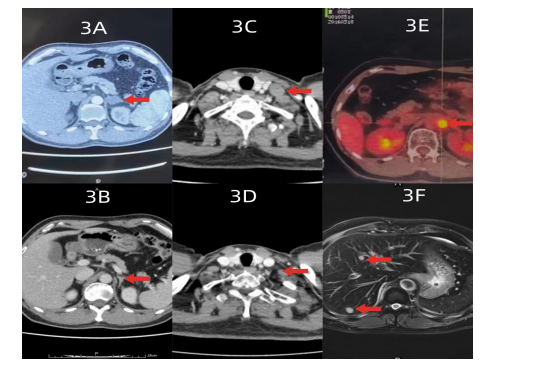
Figure 3: The patient benefited from local treatment. (A) The patient's upper abdominal enhancement CT on October 20th, 2014 revealed a new mass in the left adrenal gland, indicated by the arrow, which was considered to be a tumor recurrence. (B) After local radiotherapy, the left adrenal mass significantly reduced in size compared to before radiotherapy. (C) A repeat chest CT on October 16th, 2017 revealed an enlargement of a new metastatic lymph node on the left supraclavicular side. (D) The left supraclavicular lymph node was significantly smaller than before. (E) Increased metabolism of the periaortic lymph node, which was considered malignant. (F) Long T2 signal indicated by the arrow, suggested multiple metastases in the liver.
FIGURE 4

Figure 4: The patient benefited from the immunotherapy. (A) PET-CT showed that the right parietal, left parietal, and left parietal iliac vessels lymph nodes of the abdominal aorta were larger than before, and the metabolism was increased as indicated by the arrows. (B) The metabolism of the left parietal abdominal aortic lymph nodes was lower than before after PD1 treatment, as indicated by the arrow
FIGURE 5
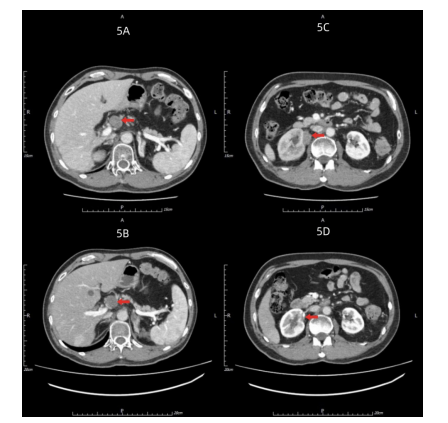
Figure 5: Targeted anti-vascular treatment benefited the patient. (A, B) Abdominal CT showed enlarged lymph nodes around the hepatoportal and in front of the right renal vein; soft tissue nodules under the right renal portal with significant enhancement. These nodules encircled the right upper ureter, resulting in dilated right hydronephrosis, which newly occurred. (C, D) The right subglottic lesion indicated by arrows was smaller than before, and the periportal lymph nodes were stable
FIGURE 6
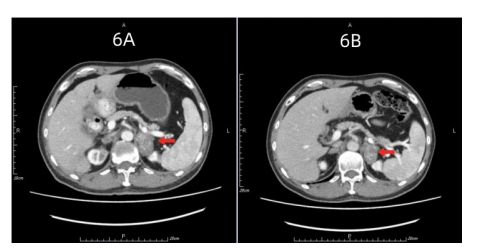
Figure 6: Immune rechallenge stage. (A) The metastases in both adrenal glands were larger than before, with the right side being particularly obvious, as indicated by the arrow. The mass also showed uneven enhancement. (B) The left adrenal mass was stable after immunotherapy.
Figures at a glance