Case Report of Synchronous Lung Adenocarcinoma and Ectopic Intrathyroidal Thymoma with Lung Metastases
Received Date: March 05, 2024 Accepted Date: April 05, 2024 Published Date: April 08, 2024
doi: 10.17303/jcrto.2024.12.103
Citation: Bonan Hou, ShaoDing Yu (2024) A Rare Case Report of Synchronous Lung Adenocarcinoma and Ectopic Intrathyroidal Thymoma with Lung Metastases. J Cancer Res Therap Oncol 12: 1-8
Abstract
Ectopic intrathyroidal thymoma is rare, to our knowledge, and almost all reported cases have never distant metastasis. A 71- year-old woman presented to the respiratory clinic with a nine-month history of neck swelling and dysphagia and with a month of dyspnea and episodic headache. Radiology showed an about 112 × 42 mm mass in the left thyroid gland with multiple solid nodules and a mixed ground-glass opacity in the lung. The thyroid mass and intrapulmonary nodules were resection and submitted into frozen sections for the intraoperative consultant. After the diagnosis of malignant thyroid tumor with pulmonary metastasis was made, debulking surgery was performed. Pathologically, the thyroid mass was an ectopic intrathyroidal thymoma (type AB) with TTF1 aberrant expression; the solid lung nodules were a metastatic thymoma, and the mixed ground-glass opacity was a lung adenocarcinoma. We found that PD-L1 and PD-1 expressed in similar locations in this ectopic intrathyroidal thymoma. The result would indicate a relatively high probability that immunotherapy is a benefit for this patient. Here, we reported the first case report of synchronous lung adenocarcinoma and ectopic intrathyroidal thymoma with lung metastases.
Keywords: Ectopic Intrathyroidal Thymoma; Pathology; PDL1; Metastasis; Lung Adenocarcinoma
Introduction
The thymic tumors contain thymoma and thymic carcinoma. Ectopic thymic tumors mean that they do not occur in the anterior mediastinum where the normal thymus is located. Ectopic thymoma is rare and predominately occurs in the cervical region, including the thyroid gland [1], paratracheal region [2] and chest wall [3]. Additionally, almost all cases of ectopic thymoma fail to recur and metastasize according to the latest WHO classification of tumors. Here, we report a rare case of ectopic intrathyroidal thymoma with lung metastases.
Case Presentation
Clinical FeaturesA 71-year-old woman presented to the respiratory clinic with a nine-month history of neck swelling and dysphagia and with a month of dyspnea and episodic headache. Neck ultrasound found a thyroid giant mass, at least 112 × 42 mm in size, extended from the left lobe to the thorax (Figure 1A). According to the Thyroid Imaging Reporting and Data System (TI-RADS), the largest was classified as 4A. The following head and chest enhanced computed tomography (CT) examination showed an irregular mass within the left thyroid and multiple nodules in the lung. The mass in the left thyroid protruded into the superior mediastinum and pushed the trachea to the right (Figure 1B). Multiple pulmonary nodules were primarily located in the bilateral inferior lung lobes and the middle lobe of the right lung and had a soft-tissue density (Figure 1C) with an exceptional nodule present with mixed ground-glass opacity in the dorsal part of the right inferior lung lobe (Figure 1D). To identify the nature of the thyroid mass and the pulmonary nodules, the patient received a surgical biopsy. During the operation, we found that the left thyroid mass protruded into the thorax and ended up in the level of the left brachiocephalic vein with the formation of tumor embolus within the inferior thyroid vein. Subsequently, the left thyroid mass and a solid nodule in the right middle lung lobe were resected and submitted to an intraoperative pathology consultant. The diagnosis of thyroid malignant tumor with pulmonary metastasis was made (Figure 1E and F). Given that the patient had an advanced stage thyroid tumor (Stage IVB), debulking surgery was performed, including pulmonary wedge resection for the visible soft-tissue density nodules and the mixed ground-glass opacity nodule, and total thyroidectomy.
Pathologic FeaturesThe resection samples were pathologically examined by paraffin embedding and sectioning. Histopathologically, the tumor infiltrated into and dissected through the normal thyroid (Figure 2A) with the formation of some intravascular tumor emboli (Figure 2B). The tumor had two components, including the lymphocyte-scarce zone and the lymphocyte-rich zone. In the lymphocyte-scarce zone, ovalshaped tumor cells formed slit-like or pseudo-glandular structures (Figure 2C). In the lymphocyte-rich zone, small and round tumor cells admixed with more lymphocytes (Figure 2D). The metastatic lesion in the lung (Figure 2E) and the inferior thyroid vein tumor embolus (Figure 2F) were the same morphology as the thyroid tumor. Moreover, the mixed ground-glass opacity nodule showed that tumor cells primarily formed an acinar pattern to break the surrounding normal pulmonary tissue, consistent with primary lung adenocarcinoma with a predominant acinar pattern. Immunohistochemistrically, the tumor cells in the thyroid mass and intrapulmonary metastases were positive for CK19 (Figure 3A), CKH, CKL, PAX8 and TTF1 (Figure 3B), and PDL1 (Figure 3C) and CD20 stained scattered tumor cells; tumor infiltrating lymphocytes were positive for CD3 (Figure 3D), CD99, TDT (Figure 3E) and Ki67, scattered tumor infiltrating lymphocytes were positive for PD1 (Figure 3F). Finally, the diagnosis of synchronous lung adenocarcinoma and ectopic intrathyroidal thymoma (Type AB) with multiple lung metastases was made.
Discussion
Embryologically, the thymus is derived from the third pharyngeal pouches, and downward migrate to the anterior mediastinum. An ectopic thymus will occur when the migrated thymus has failed to reach the destination. This mass of the left thyroid protruded into the superior mediastinum, but the tumor was primarily located at the left thyroid. So, we believe that this case is a rare thymoma derived from the ectopic thymus of the thyroid gland. To our knowledge, this is the first case of ectopic intrathyroidal thymoma with lung metastasis.
The chest CT image showed that a part-solid nodule located in the dorsal part of the inferior lobe of the right lung was different from the other pure solid nodules in the lung. Histologically, the lung nodule is a primary lung adenocarcinoma, obviously different from the other intrapulmonary metastases. According to the National Comprehensive Cancer Network guideline, this patient with T1 stage primary lung adenocarcinoma should undergo mediastinal lymph node dissection or systematic lymph node sampling. However, given that the patient with advanced-stage thyroid tumor received a debulking surgery, the mediastinal lymph nodes sampling had not been done.
TTF1, thyroid transcription factor-1, is thought to be an originated marker in practical pathological diagnosis. The epithelial component of the mouse thymus is positive for TTF1 [4], but it is unclear whether TTF1 is expressed in the normal human thymus. Recently, there is some evidence that TTF1 is expressed in the epithelial component of type AB thymoma [5,6]. These studies result further supported the diagnosis of type AB thymoma from immunophenotype.
As the behavior of type AB thymoma is generally indolent, the tumor is regarded as a borderline tumor in the 2004 WHO classification. However, thymoma is re-classified as malignancy by the latest WHO due to its potential of distant metastases. This ectopic intrathyroidal thymoma should be considered stage IVB if the Modified Masaoka clinical staging is appropriate for the thyroid gland. There is evidence that the stage IVB thymoma located at the mediastinum has a poor prognosis [7]. Although the number of case histories of the ectopic intrathyroidal thymoma with distant metastasis is limited, we are sure that this patient will have a poor prognosis because of multiple lung metastases. With targeted therapy and immunotherapy development, there are more therapeutic schedules for patients with end-stage tumors besides chemo radiotherapy. Rajan et al. have described currently almost all targeted therapy which may be possible to use for advanced thymic tumors [8]. However, it is a pity that no one immunostain indicated targeted treatment available is positive in our marker pattern. Although Marchevsky et al. doubted if the PDL1/PD-1 pathway is an actionable therapeutic target in thymoma as PD-L1 and PD-1 expressed in different locations [9], there also is evidence that immunotherapy was a benefit for a part of patients with thymic tumors [10]. Fortunately, we found that PD-L1 and PD-1 expressed in the same locations in this ectopic intrathyroidal thymoma, as shown in Figure 3c and Figure 3f. The result would indicate a relatively high probability that immunotherapy is a benefit for this patient.
In conclusion, to our knowledge, we report the first case of ectopic intrathyroidal thymoma with multiple lung metastases and this case will change the long-held view that ectopic intrathyroidal thymoma has an indolent behavior. We also describe this case from clinical presentation to radiology to pathology and discuss the therapeutic schedules available. This case report will provide an important reference for the further study of ectopic intrathyroidal thymoma.
- Park HO, Kim SH, Moon SH, Yang JH, Kang DH, Lee JH (2017) Ectopic Cervical Thymoma: A Case Report and Review. The Korean journal of thoracic and cardiovascular surgery, 50: 312-5.
- Yajima T, Mogi A, Shimizu K, et al. (2018) Ectopic thymoma in the paratracheal region of the middle mediastinum: a rare case report and literature review. BMC research notes, 11: 256.
- Cao X, Lin R, Han B, Chen C (2019) A rare case of ectopic chest-wall thymoma: a case report. AME case reports, 3: 18.
- Farr AG, Dooley JL, Erickson M (2002) Organization of thymic medullary epithelial heterogeneity: implications for mechanisms of epithelial differentiation. Immunological reviews, 189: 20-7.
- Smith T, Mauri F, Naresh KN (2016) Thyroid transcription factor-1 immunostaining in World Health Organization type AB thymoma. Histopathology, 68: 618-9.
- Yan B, Seng SC, Petersson F (2011) Thymoma with nuclear expression of thyroid transcription factor-1: a potential diagnostic pitfall on core biopsy. Applied immunohistochemistry & molecular morphology: AIMM, 19: 76-81.
- Lewis JE, Wick MR, Scheithauer BW, Bernatz PE, Taylor WF. Thymoma (1987) A clinicopathologic review. Cancer, 60: 2727-43.
- Rajan A, Giaccone G (2010) Targeted therapy for advanced thymic tumors. Journal of thoracic oncology : official publication of the International Association for the Study of Lung Cancer, 5: S361-4.
- Marchevsky AM, Walts AE (2017) PD-L1, PD-1, CD4, and CD8 expression in neoplastic and nonneoplastic thymus. Human pathology, 60: 16-23.
- Rajan A, Heery CR, Thomas A, et al. (2019) Efficacy and tolerability of anti-programmed death-ligand 1 (PD-L1) antibody (Avelumab) treatment in advanced thymoma. Journal for immunotherapy of cancer, 7: 269.
FIGURE 1
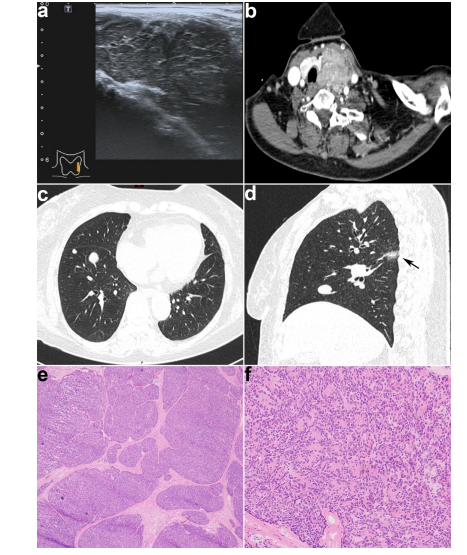
Figure 1A: Ultrasound showed that the left thyroid had a large hypoechoic solid nodule with a clear margin. (B) Enhanced-CT in the axial plane showed an irregular heterogeneous enhanced mass within the left thyroid pushing the trachea to the right. (C) Non-enhanced CT in the axial plane showed multiple solid nodules in the inferior lobe of the right lung. (D) Non-enhanced CT in the sagittal plane showed a mixed ground-glass opacity in the dorsal part of the inferior lobe of the right lung (arrow) and a solid nodule. (E) In the frozen section, the tumor showed a multinodular growth pattern characteristic of the "jigsaw puzzle" pattern. (F) At a higher magnification of (E), tumor cells formed a pseudo-glandular pattern
FIGURE 2
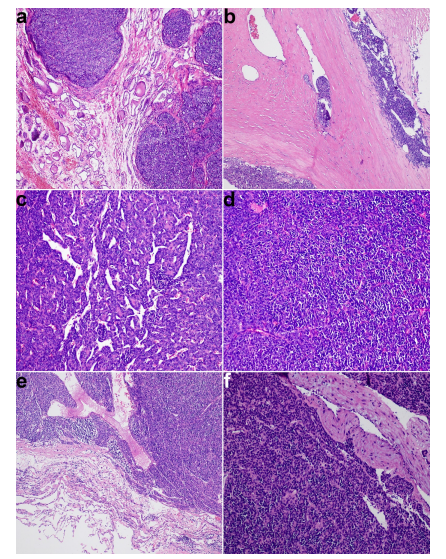
Figure 2: The postoperative pathological section showed that the tumor involved in the normal thyroid (A) and some intravascular tumor emboli were observed (B). (C) In the lymphocyte-scarce zone, oval-shaped tumor cells formed slit-like or pseudo-glandular structures. (D) In the lymphocyte-rich zone, small and round tumor cells admixed with more lymphocytes. (E) Intrapulmonary solid nodules were well-demarcated and the same histomorphology as the type AB thymoma. (F)Tumor embolus of the inferior thyroid vein was identified as type AB thymoma
FIGURE 3
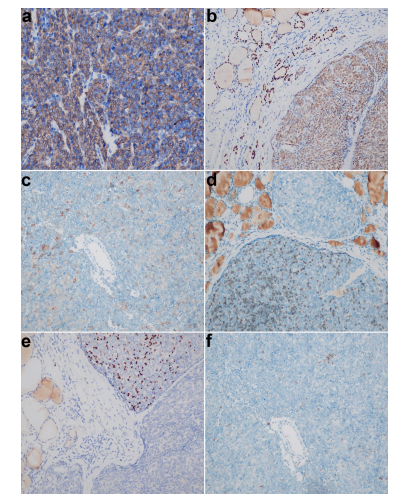
Figure 3: (A) Tumor cells in thyroid mass were diffusely positive for CK19. (B) Tumor cells in the thyroid mass and surrounding normal thyroid glands showed nuclear staining for TTF1. (C) Scattered tumor cells in the thyroid mass were positive for PDL1. Tumor infiltrating lymphocytes were positive for CD3 (D) and TDT (E). (F) Scattered tumor infiltrating lymphocytes were positive for PD1
Figures at a glance