The Application of Three-Dimensional (3D) modelling in Pelvis and Hip Surgery
Received Date: April 24, 2024 Accepted Date: May 24, 2024 Published Date: May 27, 2024
doi: 10.17303/jcrto.2024.12.205
Citation: Tauhid Sajjad, Chaoyong Wang, Zeeshan Farhaj, Muhammad Shahbaz, Islam MD Shariful et al. (2024) The Application of Three-Dimensional (3D) modelling in Pelvis and Hip Surgery. J Cancer Res Therap Oncol 12: 1-14
Abstract
Purpose: The emerging Three-dimensional (3D) modelling improves intraoperative visualization, management, and analysis of available imaging data, the 3D form of available image, provides the surgeon with a better comprehension of the geometry, size, and exact relationship between target and normal tissue. The role of 3D modelling in orthopedic pelvic and hip surgical planning is brought to focus.
Methods: The Medline database was searched using the keywords 3D printing, three dimensional printing, 3 dimensional printing and the results were screened for pelvis and hip surgery related full text articles. The duplicates and non-related articles were removed.
Results: The articles were used to build a review with focus on Acetabulum, Pelvis, Hip and sacrum. We found that the role of 3D printing is non-negligible. The advances made with the help of 3D printing are wonderful and promising. The use of 3D saw its application in many fields. But the orthopedic surgery to our observance has benefitted the most till now.
Conclusion: With the advances in the technology it is needed to make the 3D modelling easier, quicker, accurate, cost effective and reliable to help implement its deeper use in orthopedics. The authors believe that the 3D printing is an enormous help for the orthopedic surgeons which will only lead to positive outcomes
Keywords: 3D Modelling; Pelvis; Hip; Acetabulum; Orthopedic Surgery; Review
Introduction
The very process of producing the three-dimensional (3D) objects by the use of constructive geometry from available images and rendering them to solids is called 3D modelling. The sources of the images can either be magnetic resonance imaging, functional magnetic resonance imaging, magnetic source imaging, computed tomography, positron emission tomography, single photon emission tomography, ultrasound and surface light scanning [1]. The most common modality of imaging in orthopedics is X-ray. Other modalities such Computed tomography (CT) scanning, Magnetic resonance imaging (MRI) are also commonly used. Any surgical procedure will tend to have good surgical results if preoperative planning is done. The use of imaging modalities helps determining the approach to deal with target tissue. Therefore, it is of utmost importance that imaging is used in orthopedics procedures. This use helps in diagnosis and planning the procedure and execute the plan successfully. The 3D printing/ modelling is a rapidly rising imaging modality. The surgeons have started using this in almost all fields of orthopedic surgeries. The 3D reconstructed images help in obtaining graspable knowledge of patient’s pathological, traumatized, and normal bone and soft tissue. This greatly enhances the surgeon’s knowledge about the target tissue and surrounding tissue which help in preprocedural planning and procedural execution for best operative outcomes. This also helps in patient specific 3D printed instrumentation and precise surgical results. Today, thanks to 3D modelling, patient specific customized casts, prosthesis, and orthoses are being manufactured, these are not only limited to orthopedics [2-6]. The computer aided and robotics surgery have been used to improve the accuracy of component positioning in hip arthroplasty but have had limited uptake because of high costs, increased operating times, and other logistic issues. There are reports about the image guided arthroplasty [7,8], yet the data shows that conventional surgery is still the choice [9]. Further recently, patient-specific instrumentation has been developed to guide the positioning of components during surgery. This technique uses imaging techniques such as CT and MRI to plan surgery in a virtual 3D environment. The surgeon can then plan prosthesis orientation and position in relation to a chosen standard frame of locus and execute the plan using simple intraoperative patient specific guides.
Trauma fractures commonly present as intra-articular fractures (tibial plateau), usually caused by elevated-dynamism trauma. Different injury mechanisms lead to various types of fractures. They are complex intra-articular injuries with implications for articular congruity, cartilage integrity and extra-articular structures [10]. The goals of trauma fractures' treatment are anatomic reduction of the articular surface, restoration of axial alignment, recovery of joint stability, and rigid internal fixation. Conservative treatment is only restricted to undisplaced fractures, rarely suitable for these fractures. The anatomy of the tibial plateau is complex, and the nature of such fractures often associated with implications for articular congruity, cartilage integrity and extra-articular structures, which bring great difficulties to surgical treatment. Tibial plateau fractures are challenging to treat because of the difficulty of reducing and retaining multiple articular fragments as well as correct restoration of axial alignment [11]. In the practice, conventional surgeries of open reduction and internal fixation have proven to be reliable, but the outcome of these treatment is still far from perfection and satisfaction until now. The preoperative preparations play a fundamental part in the treatment of tibial plateau fractures, including the design of the surgical approach, the process steps for reduction, the placement of the implants, and the need for bone grafts. Surgeons often need to conduct preoperative preparations based on the results of auxiliary examinations (X-ray, CT, MRI). However, it is difficult to visualize the morphology of fracture site ideographically by limited insight on screen, let alone projecting specific preoperative surgical plans. The empirical operations unsurprisingly lead to errors in the choice of operative approach and internal fixation. As a consequence, these errors cost time and effort during operation, increase intraoperative blood loss, have remorseful impacts on the outcome, even complicated with infection, implant failure, knee stiffness, knee instability, posttraumatic osteoarthritis, etc.
The Medline database was searched using the keywords 3D printing, three dimensional printing, 3 dimensional printing (Figure 1).
Here we present the current work with the use of 3D modelling in orthopedic pelvic interventions with the use of 3D modelling, summarize the work done so far and describe the evidence regarding its use in clinical practice.
Discussion
AcetabulumZeng. C et al. [12] prospectively studied 10 patients with acetabular fractures. The fractures were anterior column in 3 cases, T shaped in 1 case, 1 case with a transverse and posterior wall fracture and 5 cases of both column fractures. The authors made virtual simulation of reduction and to judge the length of screws. Then the manipulated images were used to print a real size model of the patient’s acetabulum to pre-bend the plates for simulated fixation which resulted in preplanned outcome of the fixation. Most of what they simulated overlapped with the surgical results, except in some cases the screws used in simulation used were longer than the one used in actual surgery. This marks a point for improvement where actual calculations are needed for excellent results. On the other hand, 7 patients had a displacement of fracture reduction of less than 1mm while the other 3 cases had a displacement f 1-2mm. It is a negligible displacement with room for improvement as translation from images to 3D printed model and simulated application are prone to errors, hypothetically.
Cao L et al. [13] compared the use of a novel positioner for the accurate sitting of the acetabular component. The positioner was used to determine the rotation center of the hip. Post-operative radiologic assessment of the rotation of the hip the inclination angle and the anteversion angle of the cups in both groups showed no difference. The scatter of the vertical and horizontal dislocation deviated from the targeted zone by 5mm. the difference was significant between both groups. If the center of rotation is not fixed the longevity and the clinical outcome might be affected. And malposition of the rotation center of the hip may result in pseudosubluxation. All the cases in novel positioner group 32/32 and 24/40 cases in conventional group fell within the target zone. The postoperative functional and radiological improvements in patients showed that the use of the positioner helps to restore the center of rotation more precisely and provide better results yet in short term. A longer follow up is needed to establish the effectiveness.
Chen X et al. [14] performed an experimental study for fixation of plates and screws of acetabular fracture. They used 14 adult cadaver pelvises to obtain computed tomographic scans in order to prepare 3D models. The fractures were produced in software according to Judet-Latournel fracture lines. The software was then used to prepare guiding template which was then printed. Then the template was used for prebending the plates. The plates were placed with screws using ilioinguinal approach and Kocher-Langenbeck approach. The cadavers were then further scanned after fixation. There was no penetration reported. There was no significant difference between the entry or exit points. The guiding template and bending module helped in accurate placement of the plates and screws for the treatment of the acetabular fractures and opens a horizon for future individualized surgical outcome.
Li BF et al [15] analyzed 50 cases of acetabular fractures. The digital anatomical 3D models were used, for simulated fracture reduction. The 3D printed pelvic model were then printed for definite diagnosis and to understand the type of the fracture for surgical planning. The operative findings were consistent with the 3D models. This aided the authors in shortening the operative time, reduction in bleeding. The Matta score revealed that the anatomical reduction was possible in 41 cases and satisfactory reduction in 9 cases. Further, Harris functional criteria placed 32 patients in excellent, 12 in good and 6 in acceptable outcome category. This meant that the translation of the spatial relation and anatomic structure was accurate and its assistance in surgical planning and outcome is noteworthy.
Liu X et al [16] also studied the use of 3D modelling and computer simulation in preoperative planning of the acetabular fractures. This was a retrospective analysis. There were 53 patients with pelvic fractures in their analysis. There were 34 patients in conventional treatment group, and 19 patients in 3D features assisted group. as with previous studies, the intraoperative blood loss, transfusions, reduced fluoroscopy time and operative time, were significant as compared to the conventional group. When assessed with Mattas scores, the 3D group had excellent or good outcome in 94.7% of the patients as compared to 82.4% in conventional treatment group. Similarly, the hip function was excellent or good in 3D group standing at 89.5% at final follow-up and 85.3% in conventional group.
Upex P. et al [17] worked on a both column fracture of right acetabulum in a 39 years old male. The 3D model of horizontally reversed left healthy hip was used to pre-contour the plates for fixation. The sterilized plates were then used for satisfactory reduction and fixation on the fracture, although the plates were pre-contoured based on the healthy hip assuming that both hips are identical, still the outcomes were acceptable as no further contouring was needed to fix the plates. Rest of the post-operative course was uneventful. They estimated that the pre-contouring saved approximately 30 minutes of operative time. The authors emphasize on the use of this technology to save time, money and to further implement this technology to reduce monopolized effect of industry because of huge difference in cost.
Mai JG et al [18] reported the use of complex acetabular fracture with the use of 3D model. They used acetabular wing-plate customized for each patient with the help of 3D model. As per Letournel-Judet classification, there were anterior and posterior hemitransverse fractures and 6 both column fractures, without posterior wall fracture or contralateral pelvic fracture. The acetabular wing-plate was printed with titanium. And they treated all the fractures from lateral rectus approach. The anterior column and quadrilateral surface fractures were fixed with 3D printed titanium wing-plate. The posterior column fractures were reduced and fixed by antegrade lag screws under vision. The outcomes were excellent to good for anterior and posterior columns. There was one case (75 years old female) had a loose screw in the pubic bone at 1-month follow-up, but no intervention was done as patient did not complain of any discomfort. By the Matta score the reduction was excellent in 3 cases, good in 4 and fair in 1 case. The bone union was noticed in all cases. According to the modified Merle D′Aubigné and Postel scoring system, 5 cases were excellent, 2 cases were good, 1 case was fair. The follow-up time is short in this series and long term follow-up is required to further strengthen their observation.
Cai Z. et al [19] studied the use of computed tomography in accurately measuring the acetabular anteversion in children with developmental dysplasia of the hip. There were 186 children with developmental dysplasia of the hip. All the patients were unilaterally affected. None of the children had any neuromuscular disorder or other congenital malformations. The outcomes of the measurements were consistent within the 3D computed tomography and the 3D printed model, but were not consistent with the 2D computed tomography. Their results show that the 3D computed tomography is more accurate than the 2D, as the results of 3D were basically consistent with the actual degree of the acetabular anteversion. The study is limited to children with developmental dysplasia of the hip, the authors did not analyze acetabular abduction angle and anteversion angle of the femoral neck to evaluate the pathology changes of the hip joints which require further studies.
Wan L. et al [20] presented a comparative study of 96 patients divided in two groups as 3D and conventional to compare the feasibility and value of reduction. Both groups had equal number of patients. There was no statistical difference in general data and acetabular fractures in both groups. The 3D group was significantly better than the conventional group by the means of shorter operation time, less bleeding and the number of intraoperative fluoroscopies. The rate of complication was higher in conventional group. There was no significant difference in reduction quality of the both groups. The results show that 3D help can assist the surgeons for better outcomes, yet the reduction quality might be same.
Zhou X. et al [21] studied the significance of the 3D arterial model in the management of the delayed reconstruction of acetabular fractures. The skeletal and arterial models were accurate. The reduction and fixation were smooth and the superior gluteal artery injury was avoided with the help of printed model. The superior gluteal artery was ligated in 1 case, as there was no possible way in preoperative planning, while in all other cases the superior gluteal artery was preserved. The implants were pre-contoured. This made the fixation easier. The implants were fixed successfully in 6/8 patients without further adjustments in contour. While in 2/8, in case 1 a fragment was unreliably fixed by the plates and unexpectedly a screw was needed to enhance the fixation, and in the other case the, the four-hole plate was not fixed easily as the space limited the options so the plate was shortened. The outcomes were anatomical reductions in 4/8, and imperfect reductions in 4/8. The authors did not mention the use of scores to judge their reduction or functions postoperatively.
Wan L. et al [22] studied the curative effect and prognosis of 3D printed titanium alloy trabecular cup and pad for acetabular defect of hip joint revision. There were 42 patients, 22 in observation and 20 in control group. The preoperative Harris score was not statistically significant among groups. The Harris score was significant postoperatively in observation group. the pain VAS score was not significant before operation among groups. The pain VAS score was significantly lower in observation group postoperatively. Similarly, the quality of life SF-36 score was significantly in observation group. the follow-up time is short, only for 1 year after operation. A long-term follow-up is required to further ascertain the effects of 3D printed titanium alloy trabecular cup and pad as compared to conventional.
Liu ZJ et al [23] successfully used 3D modelling in reduction and fixation of the complex acetabular fracture. The simulated operation was performed to plan for the surgery day. The preoperative simulation resulted in anatomical reduction and decreased operative time and blood loss. The simulated operation is free of soft tissue so the length and number of plates might be different in actual occurrence which is a matter to study carefully.
Deng A et al. [24] reported a patient with acetabular fracture which as operated laparoscopic assisted operation with the guide of 3D printed model. The authors also report shortened postoperative recovery time due to optimal surgical outcomes which promoted the rehabilitation process successfully.
Fukushima K. et al [25] reported the use of 3D model for the periacetabular osteotomy in young adults with developmental hip dysplasia. Due to its steep learning curve, the authors thought that a preoperative simulation on a model with help to improve the outcomes and decrease the learning curve to effectively perform periacetabular osteotomy. They performed a surgery with the help of 3D model which on simulation enlightened that if a conventional osteotomy is performed there will be anterior impingement. So, a modified osteotomy was performed which had better outcomes. The authors have only one case to support the outcomes. A longer study with more cases is required to establish the outcomes.
Duncan JM et al [26] reported the use of 3D printed model in the treatment of a both column acetabular fracture. The help of 3D printed model guided for exact operative plan and authors feel that it helped them avoid dual or extensive approach in the treatment of this case. The tactile help lead them to anatomical reduction. They also implied on further exploration in the field of 3D modelling as this helps in greater outcomes.
Kavalerskiy GM et al [27] reported 17 cases of revision surgery with complex acetabular defects. With the help of 3D models, severe acetabular defects (Paprosky IIC, IIIA, IIIB) revision surgeries were performed successfully. They noted the size of the planned and used components were same in 64.3% of cases. While in other cases the difference was not more than 2mm. while in all cases the type of planned and used augments were same. This shows another successful use of the 3D modelling method in complex surgeries.
Maini L. et al [28] performed a randomized case control study of 21 patients with acetabular fracture. Patients in case group were operated with help of 3D model while those in control underwent conventional approach. They report less blood loss, operative time and better anatomical reduction in case group. The reduction of case group was statistically significant as evaluated by the computed tomography. The pre-contoured plates fitted well intraoperatively. The pre-contouring is useful but the results were insignificant, this might have arisen from the small sample and varied fracture pattern in cases. So a further study with same fracture types will be helpful in pre-contouring assessment.
Shon HC et al [29] also reported the beneficial use of 3D modelling in both column acetabular fracture with limited exposure through an incision 3cm above the pubic symphysis. If needed another incision for lateral window was made along iliac crest for fractures extending to ileac crest or posterior column fractures. The resultant reduction was excellent in 4/5 and good in 1/5 according to Matta criteria. The functional outcome was good in all patients by modified Merle d’Aubigne score. The limit in the study was the modelling, as the author could only print one connected form. Therefore, a displaced fracture a gap between fragments was seen as connective entity. This connection needed to be cutout and separation. This could lead to severe misunderstandings.
Heunis JC et al [30] report an unfortunate case of 21-year-old male, with metastatic osteosarcoma. The metastatic focus was in left posterior inferior rim of acetabulum. The patient underwent successful resection of the metastatic lesion. The operation was planned with a 3D model to delineate the osteotomy. He returned to his normal life routine afterwards. The case shows successful use of 3D modelling in a complete osteotomy. The patient, later passed away 3 years after hi initial diagnosis due to recurrent metastasis. Author imply that such resections can prolong the survival of a patient or a cure. Authors also point to upfront costs of the 3D modelling which are ~3000USD.
Brouwers L et al [31] studied the interpretation of the acetabular fracture according to Judet- Letournal classification between observers of different levels of the experience. They observers were asked to state their preferred approach in treating the observed fracture. When using 3D modelling model there was more agreement on surgical approach as compared to the virtual reality model. The time used to classify these fractures was not different among the observers. The Judet-Letournal classification is still difficult to interpret. Yet the authors found that the 3D modelling was superior to virtual reality in classifying the fracture. And the 3D modelling technology hold upper hand as compared to virtual reality model, as it can be used in the operative settings.
Pelvis
Pelvic FracturesZenj CJ et al [32] used the 3D modelling models for minimal invasive surgery for internal fixation with plate of pelvic fracture through a small incision. There were 50 patients who underwent pelvic fracture surgery for anteromedial internal fixation. The 3D model was used for simulation operation to identify optimal location for plate screw fixation, to template the plate according to the bone contour. The model also assisted in screw length measurement and screwing approach. The diaplases and internal fixation was undertaken from extraperitoneal space. The outcomes were from good to excellent in 96% of the patients.
Postoperative radiographs showed close similarity in the internal fixation on patient and 3D model. The 3D model helped them to a great extent, as no screw breached the hip joint cavity. The operative time was shorter too. This shows that a minimal invasive surgery was done with ease by 3D model simulation prior to operation.
Yang H et al [33] also evaluated unstable pelvic fracture internal fixation by the use of cannulated screws with the help of 3D printed insertion template. They had 10 patients in the study. Most of the patients were males 7/10. There were 6 patients with sacral fracture, 1 case with sacroiliac joint dislocation, 3 cases of iliac bone fracture. The 3D model was used for screw fixation and the operative outcomes were excellent in 8/10 cases and good in 2/10 cases. No complications were reported. The follow up showed good fracture healing. The simulation resulted in excellent functional outcome in 9/10 cases and good in 1 case. This shows that the 3D printed insertion template used by the Yang et al was able to guide them for precise and optimal screw fixation. This showed that the 3D printed model can be used for the treatment of the unstable pelvic fracture screw fixation.
Nie WB et al [34] used the 3D model simulation along with minimal invasive surgery for the pubic rami fracture. There were 30 patients in their series all of whom underwent minimally invasive surgery aided by the 3D model for the fixation of the anterior pubic ring. As of earlier two series the surgical outcomes were optimal. As of previous references, the Matta criteria showed excellent effectiveness in 22/30 cases and good in 8 cases. On the other hand, functional evaluation of criteria of Majeed showed excellent effectiveness in 21/30 and goo in 9/30. This outcome suggests that the 3D printed model along with minimally invasive surgery can better treat these fractures. The 3D model helps in plate modeling, which will definitely shorten the operative time. As like previous series the surgical accuracy improved and better results were achieved as per Matta and Majeed criteria.
Sanghavi PS and Jankharia BG. [35] presented a case of right acetabular fracture, they used the 3D model to actually hold the fractured model over seeing it in images which helped them to understand the fracture pattern, understand accurate classification of the fracture, and better understanding of the situation was made clear. Rather than fixation the decision was changed to total hip replacement. The outcome was time, cost and material savings. Which are beneficial for everyone.
Wu C et al [36] compared the use of 3D printing model assisted surgery with the conventional surgery and found that, the Majeed criteria was significantly higher in 3D assisted surgeries and the success rate of sacroiliac joint screw fixation was of category I in 3D assisted surgeries. There was decrease in operation time, blood loss and fluoroscopy time when assisted with 3D model. The patients who were operated with 3D model assistance had good waiting time for weight bearing exercise and function. They suggested that the 3D assistance is a good alternative for treatment of unstable fractures.
Hung CC et al [37] also compared the conventional versus 3D assisted contoured plate fixation in the treatment of anterior pelvic ring fracture. There were 30 patients, 16 of whom underwent 3D assisted surgery and 14 conventional surgeries. Not surprisingly, the group with 3D assistance had shorter internal fixation time, surgery time, and less blood loss.
However, the postoperative radiologic results were same in both groups. This shows that 3D assistance is reliable and effective as compared to conventional approach. With the help of 3D model, a safer surgery and personalized surgical plan can be carried out.
Pelvic tumor and 3D printing assisted surgeryLele D et al [38] reported a pelvic malignant tumor resection and then reconstruction with the help of 3D model, and a custom-made pelvic prosthesis fixation, total hip replacement, pelvic and hip joint reconstruction were carried out. This resulted in acceptable outcome for the surgery. Although the authors reported huge intraoperative blood loss of 4000 ml, given the field they were working, which is a big point of concern, could this have been avoided, the surgery would have been outstanding. Future steps are to be taken in preventing such intraoperative blood loss which will promote the use of such custom-made prosthesis fixation.
Liang H et al [39] reported a series of 35 patients who underwent resection of pelvic tumor and then reconstruction using 3D printed endoprostheses. A variety of prosthetic surgeries were performed in their series, which were reconstruction using iliac prosthesis, standard hemipelvic prosthesis, and screw-rod connected hemipelvic prosthesis. All the patients had an en bloc resection. There were 25 patients who were alive after a mean follow-up period of 20.5 months, 5 were still alive with the disease and remaining five deceased from metastasis.
While there were delayed wound healings (7/35) and hip dislocation (2/35). The surviving patients with iliac prosthesis had a mean musculoskeletal society score of 22.7, 19.8 in those with standard prosthesis and 17.7 in screw road connected prosthesis. Their series shows good short- -term functional results and long-term follow up is needed to establish a strong case.
Bagaria and Chaudhary [40] reported a multicenter study where 50 patients were enrolled who were operated by 5 surgeons. The surgeries included periarticular trauma in 24 cases, pelvic trauma in 11 cases, complex primary in 7 cases, and revision arthroplasty in 8 cases. The 3D printed models were used in of the surgeries to better understand the pathoanatomy, and operation simulation. The 3D models were sterilized for intraoperative guidance. A questionnaire was used to understand the opinion of surgeons post each operation. The end results showed that the preoperative rehearsal, intraoperative use of sterilized model, surgical navigation and preoperative implant selection, would probably reduce the surgical time, improve the surgical outcomes by increasing the accuracy of the fixation. They recommended it to be used by other surgeons for the obvious positive results.
Liu X. et al [41] were interested in knowing the difference between common 3D printed anatomic templates and modified printed anatomic templates for the reconstruction of pelvis after pelvic tumor resection. The study included 38 patients, 19 for each group. The group A patients were assigned for modified printed template assisted surgery. The study was based on the zone II and III tumor resection and postoperative implant complications and tumor recurrence. So, the authors came up with the idea of customized cutting block. The results showed that, compared to the common printed template surgery, the modified 3D printed template resulted in shorter operative time, less blood loss and simpler operation. The other important outcome was lower tumor recurrence and accuracy of tumor resection. But they also noted that the rate of customized implant loosening was higher in the modified 3D printed model assisted surgery group, which is a worrisome point, this needs to be addressed for better future outcomes.
Angelini A et al [42] studied a series of 13 patients prospectively for pelvic tumor. There were 7 cases of primary bone tumor, 3 metastatic, and 3 cases of total hip arthroplasty. En bloc resection was completed in all cases, with wide surgical margins. There were no reported deaths due to perioperative complications. There were 7 patients with no evidence of disease, a case was alive with disease, and one case with no evidence of disease after treatment of local recurrence or metastasis. Another patient is without evidence of disease after surgical treatment of lung metastasis, one patient died due to metastasis and one was alive with metastatic breast cancer on chemotherapy. The reported survival was 100% at 12 months and 80% at 24 months.
The complications were reported in 5 cases. With minor complications excluded the survival was 72% and included was 62%. The musculoskeletal tumor society functionality score was 80.3% between good and excellent. The use of 3D printed prosthesis is growing with time, even customized implants are growing. The better outcomes were complete restoration of the bone defect and acceptable functional results.
Although the complications rate was high, yet the outcomes are promising and future development may see a way to deal with complications.
Han Q et al [43] reported a case of right acetabular metastatic carcinoma. They designed a 3D printed titanium alloy hemi-pelvic prosthesis. The manufacturing was based on the morphology of the unaffected side. Another 3D printed osteotomy guide was printed to for guidance and application in improving the accuracy of osteotomy and to reduce operative time. The 3D printed hemi-pelvis was successfully implanted, there was no loosening in their planned 12 months follow up time. The life quality of the patient reportedly improved. The work emphasizes that the use of 3D printed models and guides can help in improving the surgical outcome and quality of life.
Wu XB et al [44] worked on old pelvic fractures which are one of the rare and challenging presentations. The anatomical accuracy of the 3D printed model was tested by the use of dried cadaveric pelvises. Which was within the specifications? They operated on 9 cases of old pelvic fractures. The fractures were classified as type C following the Tile classification. They were type C3 in four cases, type C2 with an acetabular fracture in 2 cases, C with an acetabular fracture in 2 cases and type C3 with a T-shaped fracture in 1 case. The 3D printed templates were used to plan the surgical correction such as osteotomy position, angle required to create wedge resection geometry, to select the best incision, instrumentation and placement of internal fixation apparatus. The outcomes were optimal. There were no patients with delayed incision healing, wound infection or nonunion. Although the results were excellent and good according to Majeed scores in 77.8 % (7/9) of cases, the poor outcomes were also high in 22.2% (2/9). There is a huge room for improvement, although restoring the original anatomy is a real challenge where a lot of dynamics/factors are affecting the outcomes. Yet the authors have shown another optimal example of the 3D printed models use in orthopedic surgeries.
Hip
Joseph Z et al. [45] reported a case of total hip arthroplasty revision in a 70-year-old female. They produced a full-scale model of the hip joint. The model allowed for preplanning of revision surgery. The trials were undertaken for acetabular components, to determine the cup size, position and screw placement and to assess the need for reaming. Eventually the patient underwent revision surgery. The 3D model gave the team confidence boost as the conventional methods do not allow for such confidence grooming. This such showed that the help of 3D modelling can be obtained to plan for complex revision surgeries.
Fang C et al. [46] presented a case of intertrochanteric fracture of an arthrodesed hip. Their approach was unique as such presentations are rare due to popularization of the total hip arthroplasty. The patient was 88 years old female with history of arthrodesis 16 year ago due to tuberculosis. The use of 3D modelling enabled pre-templating the implant for the procedure. The Kirschner wires were used to fix the template on the model which was optimal. The operation was done with standard Smith-Peterson approach. The operative time was 69 minutes from skin to skin. She was able to bear weight 2 days after surgery and was discharged 22 days after surgery. Due to rarity of such fractures, is challenging. The use of 3D modelling allowed Fang et al to completely plan for the surgery beforehand. The operation was minimally invasive. The implant selection and templating allowed for a long lever arm of fixation in both fragments which was important in the case of osteoporotic bone.
The outcomes were optimal, with quick recovery and returning to pre fracture activity level in 4 months’ time.
Tserovski S et al. [47] presented a case of 66 years old male with history of coxarthrosis. The preoperative imaging showed a large right sided pelvic defect and severe acetabular defect.
The 3D modelling allowed for recognition of all areas of bony deficiency. The preoperative surgical drill with position simulation was carried on the model. The 3D model helped in correct acetabular cup and augment were selected. Nevertheless, the negative features of the 3D modelling are, technically demanding process, advanced computer skills and additional training. The model completion is a lengthy process.
Zhu W et al. [48] used laser sintering technology to print 3D porous titanium into cylinders of different sizes. Platelets were coated on a cross-linked gelatin present within the porous network of 3D-printed titanium. The release of the TGF-β1 VEGF were analyzed for expression. the in vivo setup was made for skull defect in rabbits. The stimulation by low dose growth factor showed excellent regeneration quality. And the results were promising as compared to the control group. Theirs in vivo studies showed extensive bone regeneration after the implantation of 3d printed porous titanium containing platelet coated micro scaffold. They also observed vessel regeneration which is outstanding find. The authors recommended that this discovery to be used in osteonecrosis of the femoral head as there are no satisfactory treatments of large bone defects, which require structural support or the areas of no bioactivity such a femoral head necrosis. Their model stimulates extracellular matrix and accelerates bone regeneration. This could become a definite treatment in large defects.
Zhu Y et al. [49] combined the ceramic 3D modelling technology with the antibacterial nano- modification. The zirconia ceramic implant material was obtained with precise 3D structure and effective antibacterial properties. The authors also addressed other problems of zirconia ceramic implants were effectively minimized by optimizing the reaction conditions and selective area inversing compensation, which resulted in more strength and sintering induced irregular shrinkage reduction. They observed that the zirconium dioxide material, covered with a layer of zin oxide nanoparticles. The proposed modification with zinc oxide had no significant effect on the mechanical properties of the zirconium dioxide. The inflammation was less in zirconium dioxide-zinc oxide ceramics. The zirconium dioxide-zinc oxide also exhibited better antibacterial qualities than zirconium dioxide ceramics. The cytotoxicity was also less in the authors proposed material. Their animal models demonstrated that the implants were in good position without dislocation. Which shows the proposed material used by the authors can be used for 3D modelling. In addition to these tests the sections of surrounding muscles and bone tissue showed no significant abnormality and the bone growth was observed. Although they have provided with a new material for 3D modelling with optimal qualities, yet long term research is needed to explore the deficiencies of this compound.
SacrumIn order to improve the pelvic fixation outcomes, Hansen B et al. [50] came up with a training module for S2- alar-iliac-screw. In this module postgraduates from different years of training were trained. The results presented by the author are noteworthy. A 3D printed Sacral model was used for the training purpose. The left sided free-hand screw fixation was accurate to 17% before feedback and training, which improved to 80%. Also, for the right side free-hand screw placement was only accurate for 7%, and improved to 100% after training and feedback. Another accomplishment seen during the training was the reduction of fluoroscopy time. They demonstrated that with the use of a 3D model it was easy to train the postgraduates for the screw placement and the breaches were reduced.
Zhang YZ et al [51] developed an image 3D model on a computer workstation for simulation of screw fixation and the study was reverse engineered. The tailor-made navigation method was used for each of 6 patients ranging from type I to III, with one patient accompanied by the neurologic damage. The translational errors for the drilling were minimal. The lag screws were used successfully with the computer aided precision to fix the fracture while keeping the errors of translation minimal.
Kim D et al [52] reported a case of 3D printed titanium implant post hemisacretomy due to sacral osteosarcoma. This was done with preservation of contralateral nerves. The patient was able to walk 2 weeks after operation and had left sided foot drop. The sphincter function though was preserved. This was further successful as 1 year follow up showed good bony fusion. Yet the issue of strength of such 3D printed implant can be a matter of debate.
Conclusion
Here we see that the use of 3D modelling has its advantages in the pelvic region. It has seen its use in all orthopedic sections. The professionals and scientists are using this technology with more confidence, growing with each passing day. The number of publications is also growing in this field. It looks assuring that the future of 3D modelling is bright. The future holds more marvels of the 3D modelling, which will further strengthen its cause. The era is not far when it will be adopted by other fields to improve clinical outcomes.
- Udupa JK, Herman GT (2000) 3D imaging in medicine. 2nd ed. CRC Press UK.
- Wong TM, Jin J, Lau TW, Fang C, Yan CH, Yeung K, To M, Leung F (2017) The use of three-dimensional printing technology in orthopaedic surgery: a review. J Orthop Surg, 25: 2309499016684077.
- Gadia A, Shah K, Nene A (2018) Emergence of three- -dimensional printing technology and its utility in spine surgery. Asian Spine J, 12: 365-71.
- Garg B, Gupta M, Singh M, Kalyanasundaram D (2019) Outcome and safety analysis of 3D printed patient specific pedicle screw jigs for complex spinal deformities: a comparative study. Spine J, 19: 56-64.
- Vaish A, Vaish R (2018) 3D printing and its applications in Orthopedics. J Clin Orthop Trauma, 9: S74-5.
- Trauner KB (2018) The emerging role of 3D printing in arthroplasty and orthopedics. J Arthroplasty, 33: 2352-4.
- Resubal JR, Morgan DA (2009) Computer assisted vs conventional mechanical jig technique in hip resurfacing arthroplasty. J Arthroplasty, 24: 341-50.
- Beckmann J, Stengel D, Tingart M, Götz J, Grifka J, Lüring C (2009) Navigated cup implantation in hip arthroplasty: A meta-analysis. Acta Orthop, 80: 538-44.
- NJR.12th Annual Report. http://www.njrcentre.org.uk/njrcentre/Portals/0/Documents/England/Reports/12th%20annual%20report/NJR%20Online%20Annual%20Report%202015.pdf. Accessed March 7, 2019.
- Metcalfe D, Hickson CJ, McKee L, Griffin XL (2015) External versus internal fixation for bicondylar tibial plateau fractures: systematic review and meta-analysis. J Orthop Traumatol, 16: 275-85.
- Jansen H1, Frey SP, Doht S, Fehske K, Meffert RH (2013) Medium-term results after complex intra-articular fractures of the tibial plateau. J Orthop Sci, 18: 569-77.
- Zeng C, Xing W, Wu Z, Huang H, Huang W (2016) A combination of three-dimensional printing and computer-assisted virtual surgical procedure for preoperative planning of acetabular fracture reduction. Injury, 47:22237.
- Cao L, Wang Y, Zou S, Cheng H (2019) A novel positioner for accurately sitting the acetabular component: a retrospective comparative study. J Orthop Surg Res 28;14: 279.
- Chen X, Chen X, Zhang G, Lin H, Yu Z, Wu C, Li X, Lin Y, Huang W (2017) Accurate fixation of plates and screws for the treatment of acetabular fractures using 3Dprinted guiding templates: An experimental study. Injury, 48: 1147-54.
- Li BF, Zhang Y, Tai GL, Dai YY, Xie HB, Guo XZ, Zhu CR, Wang F (2016) Application of 3D digital orthopedic techniques in treatment of acetabular fracture. Nan Fang Yi Ke Da Xue Xue Bao, 36: 1014-7.
- Liu X, Zeng CJ, Lu JS, Lin XC, Huang HJ, Tan XY, Cai DZ (2017) Application of 3D printing and computer-assisted surgical simulation in preoperative planning for acetabular fracture. Nan Fang Yi Ke Da Xue Xue Bao, 37: 378-82.
- Upex P, Jouffroy P, Riouallon G (2017) Application of 3D printing for treating fractures of both columns of the acetabulum: Benefit of pre-contouring plates on the mirrored healthy pelvis. Orthop Traumatol Surg Res, 103: 331-4.
- Mai JG, Gu C, Lin XZ, Li T, Huang WQ, Wang H, Tan XY, Lin H, Wang YM, Yang YQ, Jin DD, Fan SC (2017) Application of three-dimensional printing personalized acetabular wing-plate in treatment of complex acetabular fractures via lateral-rectus approach. Zhonghua Wai Ke Za Zhi, 55: 172-8.
- Cai Z, Zhao Q, Li L, Zhang L, Ji S (2018) Can Computed Tomography Accurately Measure Acetabular Anterversion in Developmental Dysplasia of the Hip? Verification and Characterization Using 3D Printing Technology. J Pediatr Orthop, 38: e180-5
- Wan L, Zhang X, Zhang S, Li K, Cao P, Li J, Wu G (2019) Clinical feasibility and application value of computer virtual reduction combined with 3D printing technique in complex acetabular fractures. Exp Ther Med, 17: 3630-6.
- Zhou X, Zhang Q, Song W, Zhou D, He Y (2018) Clinical significance of three- dimensional skeleton-arterial model in the management of delayed reconstruction of acetabular fractures. BMC Surg, 18: 30.
- Wan L, Wu G, Cao P, Li K, Li J, Zhang S (2019) Curative effect and prognosis of 3D printing titanium alloy trabecular cup and pad in revision of acetabular defect of hip joint. Exp Ther Med, 18: 659-63.
- Liu ZJ, Jia J, Zhang YG, Tian W, Jin X, Hu YC (2017) Internal Fixation of Complicated Acetabular Fractures Directed by Preoperative Surgery with 3D Printing Models. Orthop Surg, 9: 257-60.
- Deng A, Xiong R, He W, Wei D, Zeng C (2014) Postoperative rehabilitation strategy for acetabular fracture: application of 3D printing technique. Nan Fang Yi Ke Da Xue Xue Bao, 34: 591-3.
- Fukushima K, Takahira N, Uchiyama K, Moriya M, Takaso M (2017) Pre-operative simulation of periacetabular osteotomy via a three-dimensional model constructed from salt. SICOT J, 3: 14.
- Duncan JM, Nahas S, Akhtar K, Daurka J (2015) he Use of a 3D Printer in Pre-operative Planning for a Patient Requiring Acetabular Reconstructive Surgery. J Orthop Case Rep, 5: 23-5.
- Kavalerskiy GM, Murylev VY, Rukin YA, Elizarov PM, Lychagin AV, Tselisheva EY (2018) Three-Dimensional Models in Planning of Revision Hip Arthroplasty with Complex Acetabular Defects. Indian J Orthop, 52: 625-30.
- Maini L, Sharma A, Jha S, Sharma A, Tiwari A (2018) Three-dimensional printing and patient-specific pre-contoured plate: future of acetabulum fracture fixation? Eur J Trauma Emerg Surg, 44: 215-24.
- Shon HC, Choi S, Yang JY (2018) Three-dimensional printing-assisted surgical technique with limited operative exposure for both-column acetabular fractures. Ulus Travma Acil Cerrahi Derg, 24: 369-75.
- Heunis JC, Cheah JW, Sabnis AJ, Wustrack RL Use of three-dimensional printing and intraoperative navigation in the surgical resection of metastatic acetabular osteosarcoma. BMJ Case Rep, 12: e230238.
- Brouwers L, Pull Ter Gunne AF, de Jongh MA, Maal TJJ, Vreeken R, van der Heijden FHWM, Leenen LPH, Spanjersberg WR, van Helden SH, Verbeek DO, Bemelman M, Lansink KWW (2019) What is the value of 3D virtual reality in understanding acetabular fractures? Eur J Orthop Surg Traumatol, 30: 109-16.
- Zeng CJ, Tan XY, Huang HJ, Huang WQ, Li T, Jin DD, Zhang GD, Huang WH (2016) Clincial effect of 3D printing-assisted minimal invasive surgery through a small incision lateral to the rectus abdominis for pelvic fracture. Nan Fang Yi Ke Da Xue Xue Bao, 36: 220- 5.
- Yang H, Lei Q, Cai L, Liu F, Zhou W, Chen S, Chen L, Liu T, Jiang M, Wang K, Xiao S, Liu W (2018) Treatment of unstable pelvic fractures by cannulated screw internal fixation with the assistance of three-dimensional printing insertion template. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi, 32: 145-51.
- Nie WB, Ye FG, Ma JL, Yu JP, Wang MX, Zhang ZH, Sun FJ (2018) Three-dimensional (3D) Printing Technology Assisted by Minimally Invasive Surgery for Pubic Rami Fractures. Curr Med Sci, 38: 827-33.
- Sanghavi PS, Jankharia BG (2016) Holding versus seeing pathology. Three-dimensional printing of the bony pelvis for preoperative planning of a complex pelvis fracture: A case report. Indian J Radiol Imaging, 26: 397-401.
- Wu C, Deng J, Tan L, Hu H, Yuan D (2019) Effectiveness analysis of three-dimensional printing assisted surgery for unstable pelvic fracture. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi, 33: 455-61.
- Hung CC, Li YT, Chou YC, Chen JE, Wu CC, Shen HC, Yeh TT (2019) Conventional plate fixation method versus pre-operative virtual simulation and three-dimensional printing- assisted contoured plate fixation method in the treatment of anterior pelvic ring fracture. Int Orthop, 43: 425-31.
- Lele D, Pengnian G, Rui L, Qiang Z, Yaxiong L, Ling W, Dichen L (2017) Three- dimensional printing technology facilitates customized pelvic prosthesis implantation in malignant tumor surgery: a case report. Int J Clin Exp Med, 10: 11020-5.
- Liang H, Ji T, Zhang Y, Wang Y, Guo W (2017) Reconstruction with 3D-printed pelvic endoprostheses after resection of a pelvic tumour. Bone Joint J, 99: 267-75.
- Bagaria V, Chaudhary K (2017) A paradigm shift in surgical planning and simulation using 3Dgraphy: Experience of first 50 surgeries done using 3D-printed biomodels. Injury, 48: 2501-8.
- Liu X, Liu Y, Lu W, Liao S, Du Q, Deng Z, Lu W (2019) Combined Application of Modified Three-Dimensional Printed Anatomic Templates and Customized Cutting Blocks in Pelvic Reconstruction After Pelvic Tumor Resection. J Arthroplasty, 34: 338-45.e1.
- Angelini A, Trovarelli G, Berizzi A, Pala E, Breda A, Ruggieri P (2019) Three- dimension-printed custom-made prosthetic reconstructions: from revision surgery to oncologic reconstructions. Int Orthop, 43: 123-32.
- Han Q, Zhang K, Zhang Y, Wang C, Yang K, Zou Y, Chen B, Wang J (2019) Individual resection and reconstruction of pelvic tumor with three-dimensional printed customized hemi-pelvic prosthesis: A case report. Medicine (Baltimore) 98: e16658.
- Wu XB, Wang JQ, Zhao CP, Sun X, Shi Y, Zhang ZA, Li YN, Wang MY (2015) Printed three-dimensional anatomic templates for virtual preoperative planning before reconstruction of old pelvic injuries: initial results. Chin Med J (Engl), 20: 477-82.
- Joseph Z, Yonatan C, Rajiv C, Kenneth E, Avneesh C (2016) Three-dimensional printing for preoperative planning of total hip arthroplasty revision: case report. Skeletal Radiol, 45:1431-5.
- Fang C, Fang B, Wong TM, Lau TW, Pun T, Leung F (2015) Fixing a fractured arthrodesed hip with rapid prototype templating and minimal invasive plate osteosynthesis. Trauma case reports, 1: 79-83.
- Tserovski S, Georgieva S., Simeonov, R., Bigdeli, A., Röttinger, H., Kinov, P (2019) Advantages and disadvantages of 3D printing for pre-operative planning of revision hip surgery. Journal of surgical case reports, 7: rjz214.
- Zhu W, Zhao Y, Ma Q, Wang Y, Wu Z, Weng X (2017) 3D-printed porous titanium changed femoral head repair growth patterns: osteogenesis and vascularisation in porous titanium. J Mater Sci Mater Med, 28: 62.
- Zhu Y, Liu K, Deng J, Ye J, Ai F, Ouyang H, Wu T, Jia J, Cheng X, Wang X (2019) 3D printed zirconia ceramic hip joint with precise structure and broad-spectrum antibacterial properties. Int J Nanomedicine, 30: 5977-87.
- Hansen B, Scott LZ, Brenton G, Steven L, Chandler M, Sumit P, Scott LP (2019) A 3D- Printed Simulator and Teaching Module for Placing S2-Alar-Iliac Screws. Operative Neurosurgery opz161.
- Zhang YZ, Lu S, Xu YQ, Shi JH, Li YB, Feng ZL (2009) Application of navigation template to fixation of sacral fracture using three-dimensional reconstruction and reverse engineering technique. Chin J Traumatol, 12: 214-7.
- Kim D, Lim JY, Shim KW, Han JW, Yi S, Yoon DH, Kim KN, Ha Y, Ji GY, Shin DA (2017) Sacral Reconstruction with a 3D-Printed Implant after Hemisacrectomy in a Patient with Sacral Osteosarcoma: 1-Year Follow-Up Result. Yonsei Med J, 58: 453-7.
FIGURE 1
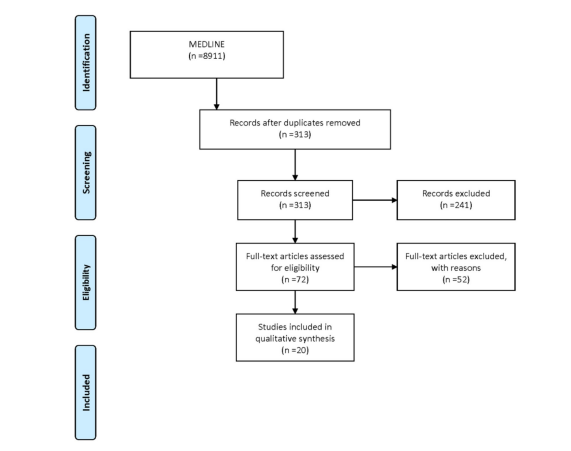
Figure 1:
Figures at a glance