Understanding Cancer Epidemiology in Himachal Pradesh, India: A Focus on Age and Gender-Wise Trend Analysis
Received Date: August 15, 2024 Accepted Date: September 15, 2024 Published Date: September 18, 2024
doi:10.17303/jctro.2024.12.402
Citation: Dr. Randhir Singh Ranta, Ms. Sakshi Sharma, Mr. Manoj Chauhan (2024) Understanding Cancer Epidemiology in Himachal Pradesh, India: A Focus on Age and Gender-Wise Trend Analysis. J Cancer Res Therap Oncol 12: 1-10
Abstract
Background: Cancer remains a significant global public health challenge, with incidence rates influenced by demographic and regional factors. This study investigated the distribution of cancer cases across different age groups, sexes, and regions in Himachal Pradesh, India, with the aim of informing targeted public health strategies.
Methods: Cancer incidence data were collected from various age groups, sexes, and blocks. Statistical analyses, including chi-square tests, were used to assess the significance of differences in cancer case distribution by age, sex, and region.
Results: Cancer incidence increased with age, peaking in the 58-67 years age group. The highest number of cases was reported, particularly among individuals aged 38 years and above. Minimal cases were observed in the youngest age groups (<17 years and 18-27 years), while a significant increase was noted in the middle age groups (28-57 years). Cancer cases were nearly equally distributed between males (50.1%) and females (49.9%). A chi-square value of 180.18 indicated a statistically significant difference in cancer incidence by age and sex. Gender-specific trends revealed higher cancer incidences in females during middle age (28-57 years) and in males during older age (58 years and above). The highest number of cases was 18.1%, followed by 14.7% and 14.6%, while the lowest incidence was 1.5%.
Conclusion: The present study underscores the need for comprehensive and targeted public health strategies to manage the cancer burden effectively. Focusing on high-incidence regions and ensuring equitable healthcare access for all genders can improve cancer outcomes and reduce mortality rates associated with the disease.
Keywords: Cancer Incidence; Age Distribution; Gender Distribution; High-Incidence Regions; Public Health Strategies
Introduction
Cancer, as defined by [1], refers to a disease characterized by the uncontrolled division of abnormal cells that subsequently invade surrounding tissues and can result in death if not treated [2]. Although there are more than 200 distinct types of cancer, they are predominantly named after the organ or cell type from which they originate. A key characteristic of cancer cells is their reduced adhesion compared to that of normal cells [3,4]. This diminished adhesion facilitates their detachment and subsequent dissemination to other parts of the body via the blood or lymphatic system. This process, known as metastasis, results in the formation of new neoplasms termed metastatic tumors.
Several behavioral factors have been reported to be associated with the incidence, screening, recurrence, and mortality of cancer. For instance, cigarette smoking significantly contributes to the mortality rates of various cancers, including lung cancer, oral cancer, and cancers of the esophagus, larynx, bladder, stomach, pancreas, kidney, and cervix [1].
Cancer is emerging as a significant public health concern in India, including in the state of Himachal Pradesh. India ranks third globally in terms of the estimated number of new cancer cases, with 1.2 million patients diagnosed in 2018, and second in cancer-related deaths, with 785,000 mortalities in the same year. According to the Global Cancer Observatory [5], the age-standardized rates per 100,000 people were 89.4 for cancer incidence and 61.4 for cancer mortality.
Cancer can affect any part of the human body and individuals of all ages, although the risk of developing cancer generally increases with age, particularly from middle age onwards. For all types of cancer combined, incidence rates for the disease quadruple between the ages of 40 and 80 [6,7]. Breast cancer is the most common form, affecting both men and women. In India, the most prevalent cancers among men are oral cancer (age-standardized rate: 13.9), lung cancer (7.8), stomach cancer (6.2), colorectal cancer (5.8), and esophageal cancer (5.5). Among women, the most prevalent types were breast cancer (24.77), cervical cancer (14.77), ovarian cancer (5.55), oral cancer (4.33), and colorectal cancer (3.11). The incidence rates of various cancers vary significantly across different regions of India, with a minimum fivefold difference for any cancer type [8,9]. However, globally, approximately 18.1 million individuals are living with cancer (National Cancer Institute, 2020). Lung, stomach, liver, colon, and breast cancers cause the most cancer deaths each year. Cancer constitutes a major public health burden in both developed and developing countries, with approximately 70% of all cancer deaths in 2020 occurring in low- and middle-income countries (WHO International Agency for Research on Cancer, 2020). In India, approximately 850,000 new cancer cases are diagnosed annually, and approximately 580,000 cancer-related deaths occur each year [10]. However, in Himachal Pradesh, the number of cancer cases is increasing at an alarming rate, with approximately 8,500 cases being detected annually, although many cases remain unnoticed and undetected in remote areas of the state (Times of India, 10 May 2023). Himachal Pradesh, with its breath taking landscapes and rural charm, presents a unique context for studying the burden of cancer. Himachal Pradesh (HP) is predominantly dominated by rural regions with 89.97% of the population living in rural areas. The population growth rate was 12.65 percent in rural areas and 15.61 percent in urban areas. According to the health indicators, Himachal Pradesh performs better than other states, and the crude birth rate (15.4) and crude death rate (6.9) of Himachal are lower than those of India as a whole. The infant mortality rate is 19, and the total fertility rate is 1.6, which proves that the state is performing well in certain health indicators (International Institute for Population Sciences [11] where other high focus states are lacking. The state faces a rising incidence of cancer, attributed to various factors, including tobacco use, lifestyle patterns, exposure to environmental risks, and genetic predispositions. In rural Himachal Pradesh, where access to healthcare services is already limited, the burden of cancer creates additional complexities and hardships for individuals, families, and local communities. However, the state has 12 districts headed by a CMO and each district is divided into health blocks. There are 75 health blocks that are headed by a senior doctor designated the Block Medical Officer (BMO). Each health block comprises community health centers, PHCs with medical doctors, and subcenters with health workers. The process of upgrading all the subcenters as health and wellness centers started with the appointment of community health officers in a progressive manner. The health institutions set up in Himachal Pradesh include 3 zonal hospitals, 9 district/regional hospitals, 6 teaching hospitals, 79 civil hospitals, 93 community health centers, 585 primary healthcare centers and 2085 health subcenters. The population of the Shimla district is 8,14,010 (census, 2011), of which 4,25,039 (52%) are males and 3,88,971 (48%) are females with a 215777 schedule caste population and 8755 schedule tribe population. The rural and urban populations are 6,12,659 (75%) and 2,01,351 (25%), respectively. Shimla has a sex ratio of 916 females for every 1000 males and a literacy rate of 83.64%. Its population growth rate over the decade 2001-2011 was 12.58%. Therefore, it is important to study the trends of cancer in Himachal Pradesh so that advanced measures may be taken to control this disease in the near future. In view of these facts, an attempt has been made to study the trends of cancers in rural areas of Shimla district, Himachal Pradesh. The objective of the present study was to examine the age and gender trends of cancer patients in rural areas of Shimla district.
Methods
The present study employed a retrospective observational design to examine the age and gender trends of cancer patients in rural areas of Shimla district, Himachal Pradesh, India. The cancer data were collected from the Regional Cancer Hospital, IGMC, Shimla, within the specified period of 2014-2022, as part of the Hospital-Based Cancer Registry. The study encompasses all cancer patients diagnosed and treated at the Regional Cancer Hospital, IGMC, Shimla.
The sample selection was based on available records that met the inclusion criteria of having a confirmed cancer diagnosis and being a resident of a rural area within the Shimla district. Patients were excluded if they resided in urban areas or were from outside Himachal Pradesh. The demographic factors and other background variables recorded included; age (categorized as below 11 years and 68 years and above), place of residence (rural/urban), gender (male/female), type of cancer, and stage at diagnosis. The stages of cancer were classified as "early" (Stages I and II) or "advanced" (Stages III and IV).
This study aimed to provide comprehensive insights into the distribution and trends of cancer incidence in the rural population of Shimla district, thereby informing targeted public health interventions and resource allocation.
Results
The present study addresses the following research questions:
Research Question 1: What is the age distribution of cancer patients in Shimla District's rural areas?
Age -wise distribution of cancer patients
The data on the frequency of cancer incidence across different age groups provide a clear illustration of the relationship between age and cancer risk. Below is a detailed analysis and interpretation of the data:
Table 1 clearly indicates that the frequency of cancer incidence increases significantly with age. This trend is particularly evident when examining the cumulative percentage of cases in each age group. Older adults (those aged 58 years and above) had the highest frequency of cancer incidence. The 58-67 years and 68 years and above age groups together accounted for 2142 patients, accounting for 57.2% of the total patients. This significant proportion highlights the increased vulnerability to cancer with advancing age and the critical need for targeted interventions and healthcare resources for the elderly population.
The incidence of cancer in middle-aged adults (38-57 years) has notably increased. Individuals aged between 38 and57 years; accounted for 1270 patients, representing 33.9% of the total patients. This substantial increase underscores the importance of regular cancer screening and preventive measures for this age group.
The incidence rate of young Adults (18-37 years) has begun to increase, with 293 cases or 7.8% of the total cases occurring in individuals aged 18-37 years. This indicates a modest increase in cancer risk as individuals enter adulthood.
Children and adolescents (younger than 18 years) had a low frequency of cancer among individuals younger than 18 years of age, accounting for only 38 cases or approximately 1.0% of the total cases.
The data underscore the strong correlation between age and cancer incidence, with a marked increase in frequency from middle age onwards. These findings highlight the importance of age-specific cancer prevention strategies, early detection, and effective management, particularly for elderly adults, who represent the majority of cancer cases. The implementation of comprehensive cancer control programs that focus on these high-risk age groups could significantly reduce the overall burden of the disease.
Research Question 2: How does the prevalence of cancer vary among different age groups in Shimla District's rural population?
Age -wise trend of cancer patients in each block
The data presented in Figure 1 and the corresponding graph illustrates the distribution of cancer cases across various age groups in different regions. The analysis is as follows:
Figure 1 shows that there is a clear trend toward increasing cancer incidence with advancing age. The cases are minimal in the youngest age groups and increase significantly from 28 years onwards, peaking in the 58-67 years age group. Theog consistently reported the greatest number of cases across all age groups, particularly those aged 38 years and older. Rampur and Jubbal & Kotkhai also had high incidences, especially in the middle to older age groups. Regions such as Chopal, Rohru, and Chirgaon exhibited a lower but still significant number of cases, particularly in older age groups.
The data suggest a need for targeted cancer prevention and screening programs, particularly focusing on regions with high incidence rates such as Theog, Rampur, and Jubbal & Kotkhai.
These strategies should be prioritized for elderly adults, especially those older than 38 years, as they represent the majority of cancer cases.
The data underscore the importance of age and regional factors in cancer incidence. This highlights the necessity for age-specific and region-specific interventions to manage and mitigate the cancer burden effectively. The implementation of comprehensive and targeted public health strategies could significantly reduce the incidence and mortality rates associated with cancer in these regions.
Research Question 3: How does the gender distribution of cancer patients differ in Shimla District's rural areas?
Gender - wise distribution of cancer patients
The data on the distribution of cancer cases by gender are summarized as follows:
Table 2 reveals that the frequency of cancer cases is almost evenly distributed between males and females, with males accounting for 50.1% and females accounting for 49.9% of the total cases. The difference in the number of cases between the two genders was minimal, with males having only 5 more cases than females. The nearly equal distribution of cancer cases between males and females suggests that cancer affects both genders similarly in this population. This equitable incidence implies that cancer prevention and treatment strategies should be equally targeted towards both men and women.
Research Question 4: What are the specific age and gender distribution of patients with different types of cancer in Shimla District's rural areas?
Chi-square test showing the association between age and gender
The data on the distribution of cancer cases by age and gender were significantly different according to the Chi-square test. The analysis is as follows:
Table 3 shows gender differences in younger age groups (<17 and 18-27 years); females tended to have higher cancer incidences than males did. In the middle aged group (aged 28-57 years), females had a greater incidence of cancer than males did. In older age groups (those aged 58 years and older), the trend reversed, with males showing higher cancer incidences than females. However, for both sexes, the incidence of cancer increased significantly with age, peaking in the 58-67 years age group and slightly decreasing in the 68 years and older age group. The substantial increase in cancer cases in middle-aged and older adults highlights the need for targeted screening and early detection efforts in these age groups. The chi-square value (χ²=180.18) indicated a statistically significant difference in cancer incidence by age and gender. This high value suggests that the distribution of cancer cases is not uniform across age groups or between genders.
The data revealed significant age and gender disparities in cancer incidence. While the overall distribution between males and females is nearly equal, specific age groups show marked differences. Middle aged females exhibit greater incidences of cancer, whereas older males have greater incidences. The statistically significant chi-square value underscores the importance of considering these differences in designing and implementing effective cancer prevention, screening, and treatment programs.
Blockwise Distribution
The data provide the distribution of cancer cases across various blocks, summarized in the table below:
Table 4 shows that the total number of cancer cases was 3743, distributed across 11 blocks. Theog, Rampur, and Jubbal & Kotkhai are identified as high-incidence regions, collectively accounting for nearly half (47.4%) of the total cancer cases. This concentration suggests a need for focused healthcare resources and interventions in these areas. These regions should be prioritized for cancer screening programs, awareness campaigns, and medical facilities to manage the high disease burden effectively. Rohru, Chaupal, and Narkanda also exhibit considerable numbers of cancer cases. Efforts should be made to enhance healthcare services and support systems in these areas to ensure early detection and treatment. Public health initiatives in these blocks should aim to identify potential risk factors and implement preventive measures to control the spread of cancer. Blocks such as Mashobra, Nankhari, Chirgaon, Basantpur, and particularly Kupvi, which have lower incidences, still require attention to maintain and improve their current status.
The distribution of cancer cases across the blocks revealed significant regional disparities, with Theog, Rampur, and Jubbal & Kotkhai being the most affected areas. Targeted public health strategies, including enhanced screening, resource allocation, and preventive measures, are essential to address the high burden of cancer in these regions. By focusing on these high-incidence areas, healthcare systems can improve cancer management and outcomes for affected populations.
Chi-square test showing the association between block and gender
The data provide the distribution of cancer cases across various blocks, broken down by gender. The table is summarized as follows:
Table 5 shows that the overall parity in cancer incidence between males and females across most blocks suggests a uniform risk of cancer for both genders within the population studied. The nonsignificant chi-square value indicates that gender does not play a significant role in the distribution of cancer cases within these blocks. Blocks such as Theog, Rampur, and Jubbal & Kotkhai exhibit the highest incidence rates, requiring targeted public health interventions to manage and mitigate cancer cases effectively.
The data revealed a nearly equal distribution of cancer cases between males and females across different blocks, with no significant gender disparity. High-incidence blocks such as Theog, Rampur, and Jubbal & Kotkhai require focused public health interventions, including enhanced screening and resource allocation. The nonsignificant chi-square value underscores the need for gender-neutral strategies in cancer prevention and treatment efforts. By addressing the specific needs of high-incidence regions and ensuring equitable healthcare access, public health systems can effectively manage the cancer burden in these communities.
Conclusion
The comprehensive analysis of cancer incidence in Himachal Pradesh reveals critical insights into the distribution of cases across different age groups, genders, and regions. The data highlight several key findings that have important implications for public health strategies and resource allocation.
The incidence of cancer increases significantly with age, peaking in the 58-67 years age group. The frequency of cases is minimal in the youngest age groups (<17 years) and starts to rise noticeably from 28 years onwards. This trend underscores the necessity for targeted cancer screening and early detection programs, particularly for older adults.
The distribution of cancer cases between males and females was nearly equal, with males accounting for 50.1% and females accounting for 49.9% of the total cases. This near parity suggests that cancer affects both genders similarly, emphasizing the need for gender-neutral public health interventions and resources.
Significant regional disparities in cancer incidence are evident, with Theog, Rampur, and Jubbal & Kotkhai reporting the highest number of cases. These regions collectively account for nearly half of the total cancer cases, indicating a greater disease burden. Conversely, blocks such as those containing Kupvi exhibit the lowest incidence rates.
The chi-square value (χ² = 180.18) for age and gender distribution indicated a statistically significant difference in cancer incidence by age and gender. However, the chi-square value for regional distribution by gender (χ² = 12.21) is nonsignificant, suggesting a uniform risk distribution across genders within the regions.
Concentrating upon the conclusion of the present research as per the analysis drawn, the following pertinent strategic initiatives need to be focused upon.
- Healthcare resources, including diagnostic and treatment facilities, should be prioritized in high-incidence regions such as Theog, Rampur, and Jubbal & Kotkhai. Ensure equitable access to healthcare services for both males and females in these regions.
- Widespread and regular cancer screening should be implemented for high-risk age groups (those aged 38 years and older) to facilitate early detection and treatment. Targeted screening in high-incidence regions can significantly improve cancer outcomes.
- Region-specific educational campaigns focusing on lifestyle changes, early detection, and cancer prevention strategies should be conducted. These campaigns should address both male and female populations equally.
- Involve technical experts and scientists from agriculture, horticulture and related areas to educate rural people regarding precautions needed to be taken while using pesticides and chemicals in agricultural or horticultural crops and in household usages.
- Surveillance systems should be strengthened to monitor cancer incidence trends continuously and evaluate the effectiveness of public health interventions. Further research is needed to understand the underlying causes of regional variations in cancer incidence.
The present study underscores the critical need for age specific, gender-neutral, and region-specific public health strategies to effectively manage and mitigate the cancer burden in Himachal Pradesh. By focusing on high-incidence regions and ensuring equitable healthcare access for all age groups and genders, public health systems can improve cancer outcomes and reduce mortality rates associated with the disease. The implementation of comprehensive and targeted cancer prevention and screening programs will be essential for addressing the significant public health challenges posed by cancer in these communities.
Conflicts of Interest
The authors declare that there is no conflict interest regarding the publication of this article.
Acknowledgements
The authors express sincere gratitude to Prof. Manish Gupta, Head of the Regional Cancer Hospital at Indira Gandhi Medical College (IGMC), Shimla, for his invaluable assistance in the collection of data. Additionally, we extend our heartfelt appreciation to Ms. Anamika, Social Worker cum Technical Officer, for her exceptional support with secretarial tasks. Their contributions were indispensable to the successful completion of this work.
- Holland JC (2009) Psycho-oncology (2nd ed.) New York: Oxford University Press.
- American Cancer Society (2024) Cancer Prevention & Early Detection Facts & Figures 2024; American Cancer Society.
- Laszlo J (1987) Understanding cancer. New York: Harper & Row.
- Williams CJ, Dennis NR (1990) Cancer Biology and Management: An Introduction. New York.
- GLOBOCAN (2018) estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, 68: 394-424.
- Mor V, Masterson‐Allen S, Goldberg RJ, Cummings FJ, Glicksman AS, Fretwell MD (1985) Relationship between Age at Diagnosis and Treatments: Received by Cancer Patients. Journal of the American Geriatrics Society, 33: 585-9.
- Sarafino EP (1998) Health psychology: Bio psychosocial interactions. New York: John Wiley & Sons.
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics.
- NCRP (2016) Consolidated Report of Hospital Based Cancer Registries 2012-2014, National Cancer Registry Programme (Indian Council of Medical Research), Bangalore.
- Dhanamani M, Lakshmi Devi S, Kannan S (2011) Ethnomedicinal plants for cancer therapy- A review. Hygeia-Journal for Drugs and Medicines, 3: 1-10.
- International Institute for Population Sciences (IIPS) and ICF (2021) National Family Health Survey (NFHS-5), 2019- For additional information about the 2019-21 National Family Health Survey (NFHS-5).
FIGURE 1
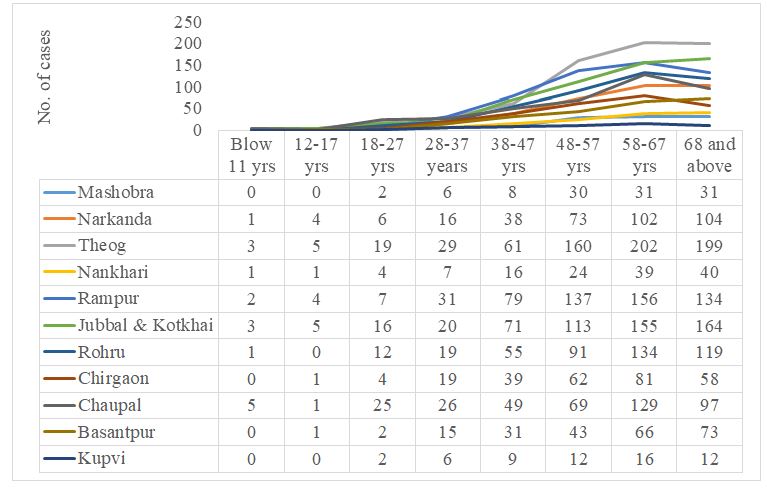
Figure 1: Age -wise trend of cancer patients in each block of the Shimla district
Tables at a glance
Figures at a glance