Post-operative Radiation Therapy in Surgically Resected Non-Small Cell Lung Cancer with Pleural Invasion in the Absence of Nodal Disease
Received Date: September 26, 2024 Accepted Date: October 26, 2024 Published Date: October 29, 2024
doi: 10.17303/jcrto.2024.12.404
Citation: Salman Ayaz, Grace Dy, Farrah R Khan, Jan A Paredes Mojica, Alejandro S Garcia (2024) Post-operative Radiation Therapy in Surgically Resected Non-Small Cell Lung Cancer with Pleural Invasion in the Absence of Nodal Disease. J Cancer Res Therap Oncol 12: 1-14
Abstract
Pleural invasion is a well-known adverse prognostic factor in non-small-cell lung cancer (NSCLC). While the role of postoperative radiotherapy (PORT) has been studied in cases with nodal involvement, its impact on NSCLC with pleural invasion in the absence of nodal disease remains unclear. We conducted a retrospective analysis of patients diagnosed with NSCLC with pleural invasion from 2010-2017, as identifffied in the SEER database. Patients were divided into two groups based on whether they received radiation therapy post-operatively. Propensity score matching (1:1) with nearest neighbor was employed to balance demographic and clinicopathologic characteristics between the two groups. Univariate and multivariate analyses were performed to assess the impact of PORT on 5-year CSS and OS. After propensity score matching, 422 patients in each group were analyzed. No significant survival benefit was observed with PORT. In fact, PORT was associated with a lower 5-year CSS and OS across all patient subgroups. The adjusted hazard ratio (aHR) for 5-year OS in the PORT group was significantly higher compared to the non-RT group (aHR 1.59, 95% CI 1.31-1.99, p < 0.001). The most pronounced survival detriment was observed in younger patients (age < 65) with an aHR of 1.73 (95% CI 1.30-2.31, p < 0.001), T2 tumors with an aHR of 2.29 (95% CI 1.53-3.43, p < 0.001), and those with visceral pleural invasion (aHR 2.15, 95% CI 1.44-3.19, p < 0.001). From the results of our analysis, it appears that PORT does not confer a survival benefit in patients with node-negative NSCLC with pleural invasion. Instead, it is associated with worse survival outcomes, particularly in younger patients and those with early-stage disease. These findings suggest that PORT should not be routinely recommended in this subset of patients.
Keywords: Non-Small Cell Lung Cancer; Pleural Invasion; Post-Operative Radiation Therapy
Background
Pleural invasion has been well-established as a negative prognostic factor in non-small-cell lung cancer (NSCLC) [1]. Pleural invasion is classified into four stages (PL0, PL1, PL2, and PL3) based on the extent of tumor invasion. Both PL1 and PL2 constitute visceral pleural invasion (VPI) whereas PL3 includes invasion of the parietal pleura and/or interlobar invasion [2,3].
This negative prognostic impact is accounted for in the tumor, node, metastasis (TNM) staging system, as VPI increases the T staging factor to T2 regardless of tumor size while PL3 is considered a T3 marker independent of size as well [4]. Both VPI and parietal pleural invasion are associated with an increase in mortality [2,3].
In patients with resectable disease staged IIA (T2b, N0) with high-risk features (e.g. size, pleural invasion) or stage IIB (T3, N0; T2b, N1), the NCCN guidelines recommend adjuvant chemotherapy with concurrent testing of PD-L1 status, EGFR mutations, and ALK rearrangements [5].
However, the role of postoperative radiotherapy (PORT) in resectable NSCLC remains debated and studies so far have found conflicting results [6]. Currently, PORT is not recommended in patients with early-stage resectable NSCLC unless they are found to have positive margins. Even the role of PORT among those who have N2 (mediastinal node involvement) on pathology after surgical resection is controversial, with recent randomized phase III trials indicating no disease-free survival benefit or overall survival benefit [7,8]. There is some retrospective evidence that PORT confers survival benefit in patients with VPI with N2 disease, however, evidence of the role of RT in pleural invasion in the absence of nodal disease is lacking [10].
The effects of PORT on recurrence or mortality in NSCLC with pleural invasion have not been thoroughly studied. We aim to retrospectively analyze the impact of PORT in surgically resected node-negative NSCLC with pleural invasion using the SEER database.
Materials and Methods
The SEER (Surveillance, Epidemiology, and End Results) database, maintained by the National Cancer Institute (NCI), is a comprehensive, population-based cancer registry that collects data from multiple regions across the United States, covering approximately 48% of the U.S. population. It systematically gathers detailed information on patient demographics, primary tumor site, tumor morphology, stage at diagnosis, initial treatment, and follow-up for vital status. By providing high-quality, longitudinal data, SEER serves as a critical resource for tracking cancer incidence, treatment outcomes, and survival trends over time. We used SEER research data from 17 state registries (Nov 2022 submission) to identify our population of interest.
Using the International Classification of Diseases for Oncology (ICD-O-3) recode, microscopically confirmed cases of lung cancer with any degree of pleural invasion, diagnosed between 2010-2017 were identified. The following variables within SEER stat (software version 8.4.3) were used to identify demographic, diagnosis, staging treatment, and survival data: age recode with singles and 85+, race and origin recode, sex, ICD-O-3, hist/behav - malignant, Grade recode (thru 2017), visceral and parietal pleura invasion recode (2010+), reason no cancer-directed therapy, Rx summ–surg prim site (1998+), Rx summ-Surg/Rad Seq, radiation recode, chemotherapy recode (yes, no/unk), SEER cause-specific death classification, and Vital Status recode.
Patient SelectionWe used the following inclusion criteria: 1- Microscopically confirmed cases of lung cancer 2- Patients diagnosed with NSCLC histology (Histology code: 8012, 8022, 8032, 8046, 8050, 8070, 8071, 8074, 8083, 8084, 8140, 8230, 8244, 8250, 8252-5, 8260, 8290, 8310, 8323, 8333, 8430, 8430, 8480, 8481, 8490, 8507, 8550, 8551, 8560 and 8574) 3- All cases underwent surgery (surgery codes: 21, 22, 30, 33, 45, 46, 47, 48, 55, 56, 66 were used to include patients that underwent likely curative surgery). 4- Only cases who received adjunct chemotherapy as part of their initial treatment were included in the study. Since SEER only captures treatment given as part of the initial treatment regimen (before relapse or progression), all cases of chemotherapy reported to be given after surgery can be presumed to be in the adjuvant setting. 5- Any degree of pleural invasion (PL1/PL2 or PL3 or any degree of pleural invasion present) was included in the study. 6- Complete information was available regarding staging data according to ACJJ 7th edition and Derived SEER combined T, N, and M (which is based on 7th edition of TNM classification). 7- Only cases with N0 and M0 disease were selected as SEER does not provide information regarding the site at which radiation therapy was given (e.g. mediastinum or local radiation etc).
The following cases were excluded from the study: Not microscopically confirmed disease. Incomplete data regarding vital status (alive or dead), unknown histologic grade, incomplete data regarding TNM stage, patients who did not undergo surgery or had surgery which was likely not with curative intent based on surgical codes. This was done to ensure inclusion of patients who underwent curative surgery. The excluded surgical codes corresponded to either vague surgical procedures or procedures that are not expected to be done with curative intent, such as cryoablation, electrocautery etc. The following surgical codes were excluded: 00 (no surgery of primary site, autopsy only), 19 (local tumor destruction or excision NOS), 15 (local tumor destruction NOS), 12 (laser ablation or cryosurgery), 13 (Electrocautery, fulguration), 24 (laser excision), 80 (resection of lung NOS), 90 (surgery NOS), 99 (unknown if surgery performed). After excluding all these cases, a total of 2,320 patients were identified. We divided these patients into two cohorts based on post-op RT status. We only included patients who received radiation therapy post-operatively. The non-RT group contained 1,752 patients while the RT group contained 422 patients.
Statistical Analysis
Propensity Score MatchingOne-to-one (1:1) propensity score matching between the no-RT and RT groups was conducted using a nearest neighbor algorithm. The matched variables were age, race, year of diagnosis, histology, and marital status.
After propensity score matching, a comparison of the variable distributions between the no-RT and RT groups was performed again using Pearson’s chi-square test to evaluate the effectiveness of propensity score matching.
Univariate and Multivariate AnalysesAfter propensity score matching, univariate analysis of the effect of each variable on the 5-year CSS rate was performed using the Kaplan-Meier survival with 95% confidence intervals.
Variables that were statistically significant with a p-value of < 0.05 in the univariate analysis were then incorporated into a multivariate analysis. Multivariate analysis using the Cox proportional hazards model was performed to generate an adjusted hazard ratio (aHR) and a p-value for each variable.
Comparison of 5-year CSS Rates Between the no-RT and RT GroupsIn each classified risk group, the 5-year CSS rates were calculated and then compared between the no-RT and RT groups using the Kaplan-Meier method followed by the log-rank test. A Cox proportional hazards model was used for multivariate analysis, incorporating all variables, to calculate the aHR for RT in each risk group.
Statistical AnalysisThe SEER database offers the SEER cause-specific death classification data. The CSS was defined as the time from diagnosis to death attributable to this lung cancer. Individuals who were alive or dead due to other causes were considered to be censored. OS was defined as the time from diagnosis to death due to any cause.
The R software (ver. 4.2.3, http://www.r-projec t.org/) package ‘MatchIt’ was used to perform propensity score matching, and packages ‘survminer’ and ‘survival’ were used to generate plots comparing the 5-year CSS rate between the no-RT and RT groups in each risk group.
Results
Propensity Score AnalysisTable 1 presents a comparison of various demographic and clinicopathologic characteristics between the RT group and the non-RT group.
The patient's age was dichotomized and age 65 (median of the entire cohort) at the time of diagnosis was chosen as the cutoff value. For tumor grade, grades I and II were grouped together while grades III and IV were grouped together. We reported the size of the tumor using the T of TNM (7th ed) instead of reporting tumor size in cm inferred from the reported T of the TNM. Since the presence of pleural invasion to various degrees would have affected the T stage making the size of the tumor in cm derived from the T stage inaccurate. NSCLC tumor histology which was not squamous or adenocarcinoma was categorized as “other”.
All clinicopathologic and demographic variables were well-matched between the 2 groups via propensity score matching and there was no significant difference between the 2 groups for any clinicopathologic or demographic variable after PSM (p-value > .05)
Survival Analysis Outcomes after PSMAs shown in table 2 and table 3, both univariate and multivariate analyses show a significant difference. Male sex and age ≥ 65 are at risk of poorer CSS compared to females and age < 65 (aHR 1.32 p=0.012, aHR 1.33 p=0.012). Similarly, the T stage also showed a significant difference in survival with both T3 and T4 having worse survival compared to T2 (aHR 1.48 p=0.008, aHR 1.52 p= 0.021). The extent of pleural invasion did not show any significant difference in survival. Similarly, no significant survival difference was found between various racial groups, tumor grade, and tumor histology.
Comparing OS according to post-op RT status, the median OS in the Non-RT group was 72 months (95% CI 58-94 months) while 48 months (95% CI 40-60 months) in the RT group (Figure 3). The 5-year OS rate was 56% in the non-RT group and 43% in the RT group (HR 1.59 95% CI 1.32-1.91 p < 0.001). Across all variable subgroups, the RT group had a worse 5-year OS compared with the nonRT group. Within each category, relatively worse outcomes were observed in lower-risk patient categories such as younger age ( HR 1.73 p < 0.001), lower T stage (HR 2.29, p value < 0.001) and visceral pleural invasion only (HR 2.15, p value < 0.001). Details are shown in Table 4.
The 5-year CSS rate was 64% in the non-RT group and 54% in the RT group (HR 1.51 95% CI 1.22-1.87 p < 0.001). Subgroup analysis for cancer specific survival had similar findings as overall survival (supplementary table 1 and supplementary figure 1).
Discussion
Our present study indicates that RT does not confer a positive impact on survival in patients with pleural invasion. Interestingly, the degree of pleural invasion itself also does not appear to be an independent predictor of survival in our cohort, which is a surprising finding [15]. These worse survival outcomes seen in our study, particularly with T2 tumors and VPI alone compared with higher T stage and more extensive pleural invasion, are consistent with many prior studies such as the landmark 1998 PORT meta-- analysis [19], which showed worse survival outcomes with PORT in lower stage tumors, especially Stage I/N0 disease, and a trend of improved outcomes in stage III/N2 patients.At the time the survival determent seen with PORT was attributed to non-cancer related causes of death such as cardiopulmonary toxicity associated with outdated techniques used for delivering radiation therapy in many of the clinical trials (7 out of 9 included trials). This meta-analysis was updated in 2016 and analyzed results from 11 randomized clinical trials [18], and the conclusion remained the same. Although RT reduced local recurrences, the reduction was off-set by a higher number of deaths in the RT group, favoring surgery alone in terms of local-recurrence-free survival. Notably, a subgroup analysis showed that trials using linear accelerators for radiation delivery demonstrated no statistically significant difference in survival with PORT. These findings suggest that RT's benefit may depend on the extent of recurrence risk. Based on our results, we hypothesize that PORT may only provide a survival advantage when the risk for local recurrence is sufficiently high. While pleural invasion poses a higher risk for local recurrence, VPI alone or smaller tumors may not be sufficient to offset the toxicities associated with PORT. This might explain the worse outcomes observed in this subset of patients.
Another possible explanation for the lack of survival benefit from PORT may relate to the pattern of recurrence in pleural invasion cases, which tends to manifest as distant recurrence, even in node-negative disease [16,17]. Assuming that patients who received PORT had complete surgical resection, additional local control with RT may offer little benefit for the systemic nature of their disease recurrence.
As with any retrospective observational study, our research has inherent limitations. One key limitation of the SEER database is the absence of data on surgical margin status, introducing the possibility of confounding by indication. Although PORT in this study is attributed to pleural invasion status, we cannot con rm whether PORT was given due to positive margins, which could negatively influuence survival outcomes. Hancock et al. [14] retrospectively analyzed 3102 patients who had microscopic residual disease (R1) after surgery and found significantly worse 5-year OS at all stages {stage I, 37% vs 62% (P < 0.0001); stage II, 29% vs 41% (P< 0.0001); and stage III, 19% vs 33% (P < 0.0001) with significant improvement in survival with adjuvant chemotherapy and radiation {(stage pI (44% vs 35%; p = 0.05), stage pII (33% vs 21%; p = 0.0013), and stage pIII (30% vs 12%; p < 0.0001 However, we addressed this limitation by excluding surgical procedures that were less likely to result in incomplete resection.
Further limitations of our study include the inability to perform propensity matching for poor prognostic features such as lymphovascular invasion and spread through airspaces (STAS), as these data are not available in SEER. We also did not adjust for the type of surgical procedure or patients’ functional status, both of which could be important prognostic factors. Additionally, imbalances in access to effective systemic therapies after disease progression are not accounted for in our analysis.
In conclusion, while the use of PORT in the setting of nodal metastasis particularly pN2 remains a topic of debate [12,13], our study adds to the evidence against the routine use of PORT in completely resected non-small cell lung cancer (NSCLC). Even with modern techniques of delivering radiation therapy, PORT still appears to be associated with survival detriment. Pleural invasion, regardless of extent, does not appear to confer a survival benefit from PORT in our cohort.
- Jiang L, Liang W, Shen J, et al. (2015) The impact of visceral pleural invasion in node-negative non-small cell lung cancer: a systematic review and meta-analysis. Chest. 148: 903-11.
- Adachi H, Tsuboi M, Nishii T, et al. (2015) Influence of visceral pleural invasion on survival in completely resected non-small-cell lung cancer. European Journal of Cardio-thoracic Surgery. 48: 691-7.
- Shimizu K, Yoshida J, Nagai K, et al. (2004) Visceral pleural invasion classification in non-small cell lung cancer: A proposal on the basis of outcome assessment. Journal of Thoracic and Cardiovascular Surgery. 127: 1574-8.
- Travis WD, Brambilla E, Rami-Porta R, et al. (2008) Visceral pleural invasion: Pathologic criteria and use of elastic stains: Proposal for the 7th edition of the TNM classification for lung cancer. Journal of Thoracic Oncology. 3: 1384-90.
- National Comprehensive Cancer Network. Non-Small-Cell Lung Cancer.
- Krupitskaya Y, Loo BW (2008) Post-operative radiation therapy (PORT) in completely resected non-small-cell lung cancer. Curr Treat Options Oncol. 9: 343-56.
- Le Pechoux C, Pourel N, Barlesi F, et al. (2022) Postoperative radiotherapy versus no postoperative radiotherapy in patients with completely resected non-small-cell lung cancer and proven mediastinal N2 involvement (Lung ART): an open-label, randomised, phase 3 trial. Lancet Oncol. 23: 104-14.
- Hui Z, Men Y, Hu C, et al. (2021) Effect of Postoperative Radiotherapy for Patients with pIIIA-N2 Non-Small Cell Lung Cancer after Complete Resection and Adjuvant Chemotherapy: The Phase 3 PORT-C Randomized Clinical Trial. In: JAMA Oncology. American Medical Association; 7:1178-85.
- Dziedzic DA, Rudzinski P, Langfort R, Orlowski T (2016) Risk Factors for Local and Distant Recurrence After Surgical Treatment in Patients With Non–Small-Cell Lung Cancer. Clin Lung Cancer. 17: e157-67.
- Liu B, Wang Z, Zhao H, et al. (2023) The Value of Radiotherapy in Patients With Resectable Stage IIIA Non–Small- -Cell Lung Cancer in the Era of Individualized Treatment: A Population-Based Analysis. Clin Lung Cancer. 24: 18-28.
- Burdett S, Rydzewska L, Tierney J, et al. (2016) Postoperative radiotherapy for non-small cell lung cancer. Cochrane Database of Systematic Reviews, 2016: 10.
- Burdett S, Rydzewska L, Tierney J, et al. (2016) Postoperative radiotherapy for non-small cell lung cancer. Cochrane Database of Systematic Reviews, 2016: 10.
- Douillard JY, Rosell R, De Lena M, Riggi M, Hurteloup P, Mahe MA (2008) Impact of Postoperative Radiation Therapy on Survival in Patients With Complete Resection and Stage I, II, or IIIA Non-Small-Cell Lung Cancer Treated With Adjuvant Chemotherapy: The Adjuvant Navelbine International Trialist Association (ANITA) Randomized Trial. Int J Radiat Oncol Biol Phys. 72: 695-701.
- Hancock JG, Rosen JE, Antonicelli A, et al. (2015) Impact of adjuvant treatment for microscopic residual disease after non-small cell lung cancer surgery. Ann orac Surg. 99: 406-13.
- Wu LL, Li CW, Li K, Qiu LH, Xu SQ, Lin WK, Ma GW, Li ZX, Xie D (2022) The Difference and Significance of Parietal Pleura Invasion and Rib Invasion in Pathological T Classification With Non-Small Cell Lung Cancer. Front Oncol. 12: 878482.
- Tian D, Pei Y, Zheng Q, et al. (2017) Effect of visceral pleural invasion on the prognosis of patients with lymph node negative non-small cell lung cancer. Thorac Cancer. 8:97-105.
- Hung JJ, Jeng WJ, Hsu WH, Chou TY, Lin SF, Wu YC (2012) Prognostic significance of the extent of visceral pleural invasion in completely resected node-negative non-small cell lung cancer. Chest. 142: 141-50.
- urdett S, Rydzewska L, Tierney J, et al. (2016) Postoperative radiotherapy for non-small cell lung cancer. Cochrane Database Syst Rev. 10: CD002142.
- ostoperative radiotherapy in non-small-cell lung cancer: systematic review and meta-analysis of individual patient data from nine randomised controlled trials. PORT Meta-analysis Trialists Group. Lancet. 352: 257-63.
FIGURE 1
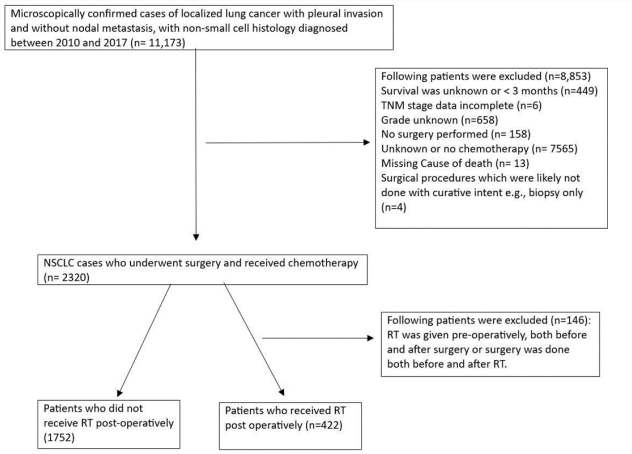
Figure 1: Flowchart demonstrating patient selection process
FIGURE 2
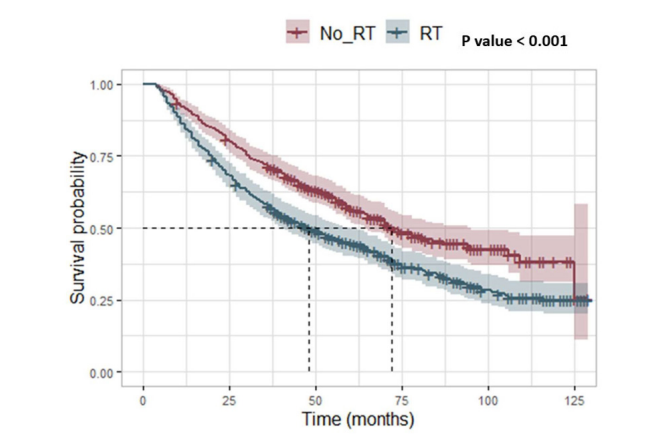
Figure 2: Kaplan Meier curve for Overall survival
FIGURE 3
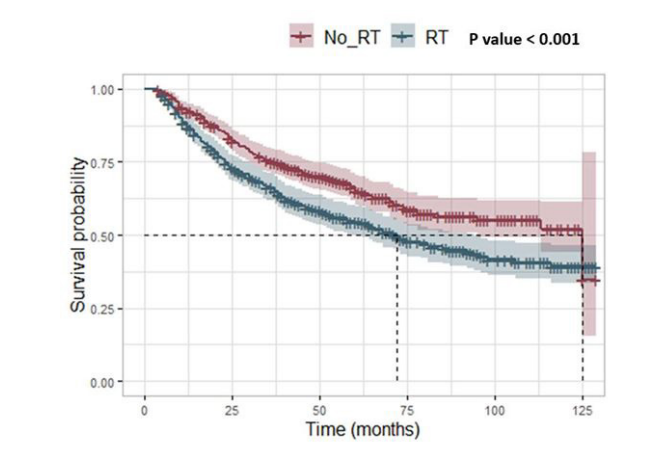
Supplementary Figure 1: Kaplan Meier Curve for Cancer-specific survival: Similar to overall survival, RT was associated with worse CSS compared to the non-RT group
Tables at a glance
Figures at a glance