Surviving Against the Odds: More than 10-Year Survival for Nasopharyngeal Carcinoma with Brain Metastases
Received Date: August 29, 2025 Accepted Date: September 16, 2025 Published Date: September 18, 2025
doi:10.17303/jcrto.2025.13.202
Citation: Pei-Jun Xie; Jie-Yi Lin, Jia-Shi Xiao, Jia-Ying Lin, Jin-Jing Lu, et al. (2025) Surviving Against the Odds: More than 10-Year Survival for Nasopharyngeal Carcinoma with Brain Metastases. J Cancer Res Therap Oncol 13: 1-8
Abstract
Brain metastases (BM) from nasopharyngeal carcinoma (NPC) are rare and historically associated with a dismal prognosis, with a 5-year survival rate approaching zero. However, emerging evidence from larger cohorts suggests potential for improved outcomes with modern management. Here, we report three cases of NPC with brain metastases who achieved exceptional long-term survival of over 10 years following multidisciplinary individualized treatment, alongside a synthesis of recent systematic data. While recent studies report a median overall survival (OS) of 11.2–25 months and a 3-year OS rate of 16.3% for this patient population, our cases demonstrate that prolonged survival is attainable. We present their distinct metastatic patterns, clinical characteristics, and treatment regimens. These outcomes, consistent with recent findings that local therapy for BM and control of extracranial disease are significant positive prognostic factors, suggest that selected NPC patients with brain metastases can achieve long-term survival with aggressive and personalized multimodal therapy.
Introduction
Brain metastases (BM) are a common and devastating complication of many solid tumors, such as those originating from the lung, breast, and colon. The current median survival for these patients remains poor, typically ranging from 3 to 27 months despite multimodal palliative treatment approaches involving surgery, radiotherapy, and systemic therapy [1, 2]. Nasopharyngeal carcinoma (NPC), known for its high propensity for locoregional invasion and distant metastasis, sees distant failure in approximately 10% of patients at initial presentation, with up to 40% of those with locally advanced disease eventually developing metastases[3,4]. While the bones, lungs, and liver are the most common sites of dissemination, brain metastasis from NPC is considered a rare event, historically associated with an extremely poor prognosis and a nearly zero 5-year survival rate [5].
Previous case reports and small series have documented the clinical challenge of NPC-derived BM, with the longest reported survival previously being 24 months [6]. Larger-scale systematic analyses have recently become available, providing a clearer epidemiological and prognostic picture. These studies, with cohorts of 40-41 patients, report a median overall survival of 11.2 to 25 months and a 3-year survival rate of 16.3%, identifying the control of extracranial disease and the application of local therapy for BM as critical independent prognostic factors [7, 8].
Contrary to the historical consensus and even these improved but still modest survival figures, our clinical experience has identified a subset of patients who achieve remarkably long-term survival. Within our center's cohort, we have observed patients surviving beyond 5 years after the diagnosis of BM. This report details three such exceptional cases, each with survival exceeding 10 years post-BM diagnosis. To the best of our knowledge, this is the first report documenting survival beyond 10 years in NPC patients with brain metastases, highlighting the potential for exceptional outcomes with modern multidisciplinary management. We meticulously describe their heterogeneous clinical presentations, metastatic patterns, and individualized treatment regimens. By presenting these cases in the context of emerging evidence, we aim to offer practical insights for managing this condition and to underscore that long-term survival is an attainable goal with aggressive and personalized multidisciplinary treatment, instilling renewed optimism in treating this challenging clinical scenario.
Method
We conducted a retrospective review of NPC patients with brain metastases treated at Sun Yat-sen University Cancer Center between November 2003 and July 2020. Demographic, clinical, treatment, and outcome data were collected from electronic medical records. Histological analysis of the brain metastasis was possible in all cases, and confirmed findings consistent with the patient’s primary tumor. Survival was calculated from the date of brain metastasis diagnosis to the last follow-up (August 2025). Informed consent was waived due to the retrospective nature of the study.
Result
Case Presentation
Case 1
A 39-year-old male was initially diagnosed with stage T3N2M0 NPC and achieved a complete response (CR) following induction chemotherapy and radiotherapy. He remained disease-free for seven years until presenting with neurological symptoms. Imaging revealed a solitary brain metastasis in the left temporal lobe. The patient underwent surgical resection of the lesion, which was pathologically confirmed as metastatic NPC. He has experienced no further recurrence and remains alive 171 months after the diagnosis of brain metastasis.
Case 2
A 47-year-old female presented with de novo metastatic NPC (T4N2M1) involving the rib and thoracic vertebra. After achieving a CR with initial chemoradiotherapy, she developed an isolated brain metastasis in the left occipital lobe 19 months later. A subsequent lung nodule was also detected. She received radiotherapy for both sites, resulting in a CR in the lung and partial response in the brain. A new small cerebellar lesion was noted six months later and managed with active surveillance due to her asymptomatic status. She has survived 132 months since the diagnosis of brain metastasis.
Case 3
A 34-year-old female with stage T3N1M0 NPC attained a CR after curative chemoradiotherapy. She developed a solitary parietal lobe metastasis 11 months later, which was resected and histologically confirmed. Despite adjuvant therapy, she subsequently developed widespread extracranial metastases (liver, lung, bone) and additional intracranial lesions. She demonstrated significant sensitivity to continued radiotherapy and chemotherapy, leading to marked tumor regression. She remains alive 125 months after the initial brain metastasis diagnosis, currently undergoing further treatment for new metastases.
(A-F) Magnetic resonance imaging (MRI) and pathological images in case 1. (G-L) MRI and pathological images in case 2. (M-R) MRI and pathological images in case 3.
Histological sections of brain lesions were used in this study. Hematoxylin‐eosin (HE) stain and Epstein–Barr virus (EBV)‐encoded small RNAs (EBERs) in situ hybridization are shown. The HE staining showed tumor cells surrounded and infiltrated by lymphocytes and the tumor cells show strong staining for EBERSs. The red arrow in the MRI points to the intracranial lesion. The dashed boxes in the pathological map represent the enlarged area.
Summary of Literature Review
A systematic literature search was conducted on PubMed (January 1985 to August 2025) using the keywords "nasopharyngeal carcinoma," "brain metastases," "NPC," "nasopharyngeal cancer," "intracranial metastasis," and "central nervous system metastasis." Manual searches of reference lists from relevant articles were also performed.
Historically, BM from NPC were documented primarily in case reports and small series. Our initial review identified 16 such individually published cases (Table 2), with the largest series comprising 3 cases, reflecting the rarity of this condition and the challenge of studying it systematically.
Recent larger-scale retrospective studies have profoundly enhanced our understanding of this clinical scenario. As highlighted by the analyses post provided, cohorts of 40-41 patients have been systematically studied, reporting an incidence of BM in NPC of approximately 0.06% and a median overall survival (OS) ranging from 11.2 to 25 months, with a 3-year OS rate of 16.3%. These studies identify key prognostic factors, including the burden of extracranial metastatic organs and the response of extracranial disease to therapy. Most significantly, they establish that the application of local therapy (e.g., radiotherapy or surgery) to BM is an independent positive prognostic factor, associated with a markedly superior median post-BM survival compared to systemic therapy alone (47.0 vs. 11.0 months).
Discussion
The exceptional long-term survival outcomes observed in our case series demonstrate the remarkable efficacy of an aggressive, personalized treatment strategy. Each patient achieved a post-metastasis survival of over 10 years, a finding that substantially revises the historical prognosis for NPC patients with BM. Our findings are consistent with recent larger studies by [7, 8], which emphasized the importance of local therapy and extracranial disease control in improving survival outcomes for NPC patients with brain metastases. Notably, the median overall survival of 11.2–25 months and a 3-year OS rate of 16.3% reported in these studies are substantially exceeded by our cases, suggesting that highly selected patients may achieve long-term survival with aggressive multimodal approaches. In all cases, the presence of brain metastasis from NPC was pathologically confirmed through biopsy. At the time of the last follow-up, the patients were still alive. To the best of our knowledge, these cases reported, for the first time, a survival time of over 10 years for brain metastasis in NPC, surpassing previous cases by a considerable margin.
In the first case, the patient experienced a single isolated brain metastasis throughout the entire treatment process. The lesion was located in a suitable location for surgical resection, resulting in a very good therapeutic outcome. In the second case, the patient had bone metastasis at the initial diagnosis of NPC, and she achieved a favorable outcome after undergoing radical treatment. Later on, the patient developed four isolated lesions in the brain and lung. Radiotherapy was implemented and yielded a favorable therapeutic response, likely attributed to the limited extent and low number of lesions. In addition, the fact that EBV remained at a level of 0 during the whole treatment period may have been an important factor contributing to her favorable prognosis. In the third case, the patient experienced multiple intracranial metastases and widespread extracranial metastasis throughout the body after undergoing radical treatment for NPC. The sheer number and extent of metastases were staggering. However, through continuous aggressive and effective treatment, coupled with the patient's sensitivity to radiotherapy and chemotherapy, the survival period was prolonged, and the patient is currently living with the disease.
These cases demonstrate the potential for combating this perilous situation and achieving outcomes that exceed expectations, which deviates from prior research and consensus. Given the lack of specific guidelines for brain metastasis in NPC patients, we based our approach on central nervous system metastasis guidelines while adapting to the unique biological features of NPC. Notably, the sensitivity of undifferentiated non-keratinizing NPC to radiotherapy or chemotherapy may play a critical role in our successful approach. Another noteworthy aspect is that, the prolonged survival time of these patients may also be attributed to the relatively low intracranial lesion burden. Also, our findings suggest that clinicians should be vigilant of the possibility of BM in those with locally advanced or metastatic disease, given that patient No.3 were already presented with symptoms of BM at a nasopharyngeal MRI reexamination, however, due to insufficient scan coverage, the intracranial lesions were not promptly detected. Appropriate and timely management can lead to outperforming prognostic expectations, instilling greater confidence and hope in the treatment of this challenging disease. Furthermore, the emergence of immunotherapy offers new avenues for systemic control. A recent phase 3 trial demonstrated that adding Toripalimab, an anti-PD-1 antibody, to first-line chemotherapy significantly improved progression-free survival in patients with recurrent or metastatic NPC [10], suggesting that immunotherapy may also benefit selected patients with brain metastases by enhancing extracranial disease control. Beyond PD-1 inhibition alone, novel combination immunotherapies are under investigation. A recent phase Ib/II trial of LBL-007 (an anti-LAG-3 antibody) in combination with toripalimab demonstrated promising antitumor activity and a manageable safety profile in patients with previously treated advanced NPC, particularly in those who were immunotherapy-naïve [11]. This suggests that dual immune checkpoint blockade could represent a viable therapeutic strategy for controlling systemic disease in advanced NPC, which is paramount for achieving long-term survival in patients with brain metastases.
Further research is needed to determine the optimal treatment strategy for BM in NPC patients, and a larger retrospective study is needed to demonstrate the survival and prognostic factors of this disease.
- Brastianos PK, Carter SL, Santagata S, et al. (2015) Genomic Characterization of Brain Metastases Reveals Branched Evolution and Potential Therapeutic Targets. Cancer Discov. 5: 1164-77.
- Achrol AS, Rennert RC, Anders C, et al. (2019) Brain metastases. Nat Rev Dis Primers. 5: 5.
- Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J (2019). Nasopharyngeal carcinoma. Lancet. 394: 64-80.
- Tang XR, Li YQ, Liang SB, et al (2018). Development and validation of a gene expression-based signature to predict distant metastasis in locoregionally advanced nasopharyngeal carcinoma: a retrospective, multicentre, cohort study. Lancet Oncol. 19: 382-93.
- Zheng SH, Liu SR, Wang HB, et al. (2021).Treatment and Survival Outcomes Associated With Platinum Plus Low-Dose, Long-term Fluorouracil for Metastatic Nasopharyngeal Carcinoma. JAMA Netw Open. 4: e2138444.
- Kuo CL, Ho DM, Ho CY. (2014). Dural metastasis of nasopharyngeal carcinoma: rare, but worth considering. Singapore Med J. 55: e82-4.
- Chen K, Shi M, Mo S, et al. (2024) Clinical features and prognostic factors of nasopharyngeal carcinoma with brain metastases. Oral Oncol.151: 106738.
- Huang N HQ, Yang Y, Wang X, Han F. (2024) Clinical characteristics and prognostic factors in nasopharyngeal carcinoma with brain metastasis: A retrospective, single-center study. Head Neck. 46: 749-59.
- Hellman S, Weichselbaum RR. Oligometastases. J Clin Oncol. Jan 1995; 13: 8-10.
- Mai H-Q, Chen Q-Y, Chen D, et al. (2021) Toripalimab or placebo plus chemotherapy as first-line treatment in advanced nasopharyngeal carcinoma: a multicenter randomized phase 3 trial. Nat Med. 27: 1536-43.
- Chen G, Sun D-C, Ba Y, et al. (2025) Anti-LAG-3 antibody LBL-007 plus anti-PD-1 antibody toripalimab in advanced nasopharyngeal carcinoma and other solid tumors: an open-label, multicenter, phase Ib/II trial. J Hematol Oncol. 18: 15.
FIGURE 1
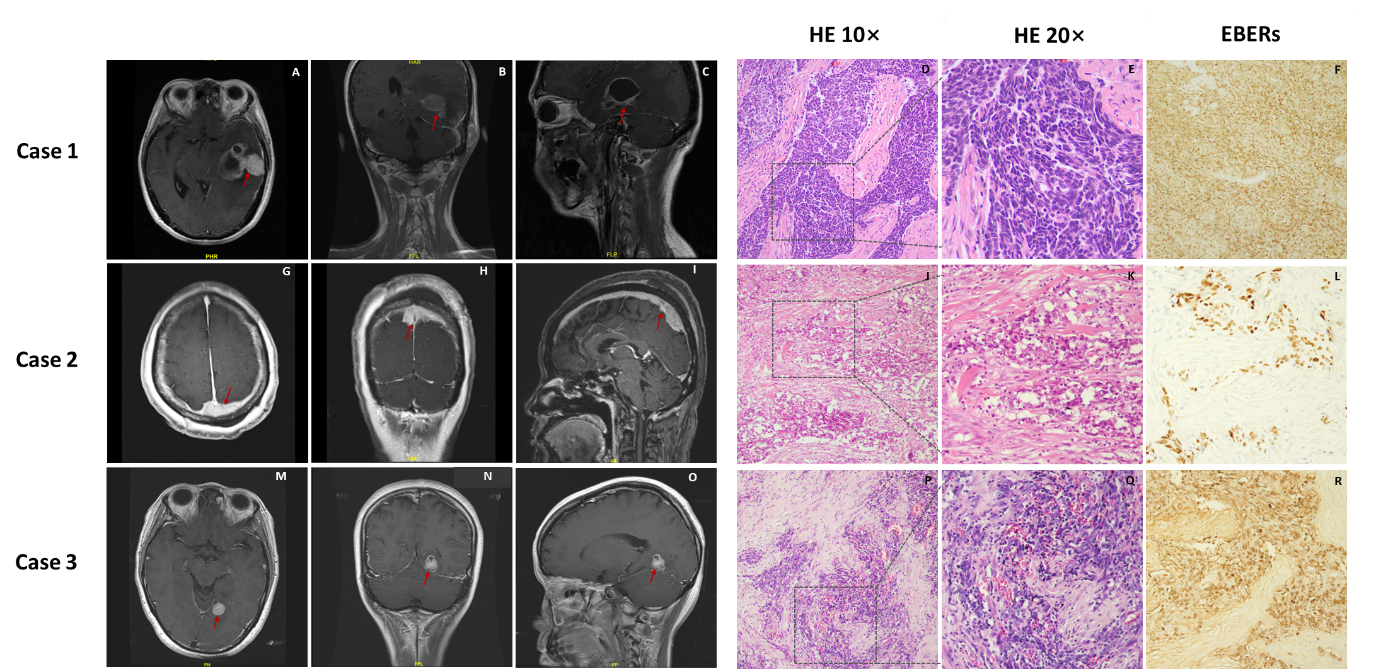
Figure1: Magnetic resonance and pathological images of patients.
Tables at a glance
Figures at a glance