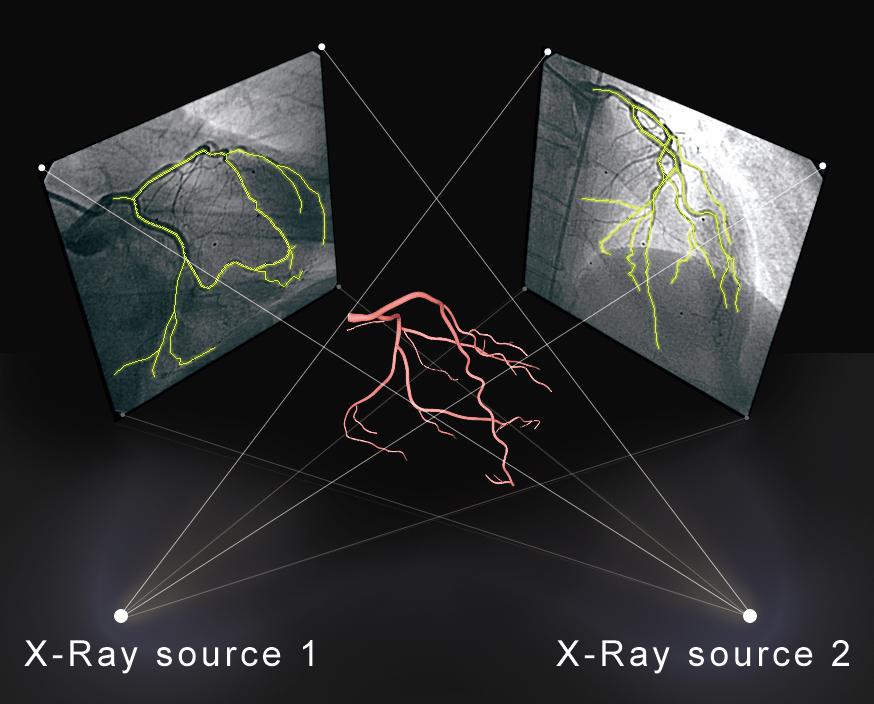
Figure 1: Three Dimensional coronary models reconstructed from two planar angiograms.
| N=26 patients | |
| Mean Age | 59 ±10 yrs |
| Male | 80% |
| CAD | 11 (42%) |
| Diabetes Mellitus | 5 (19%) |
| Hypertension | 20 (77%) |
| Dyslipidemia | 17 (65%) |
| Chronic Kidney Disease | 1 (4%) |
| Family History of CAD | 5 (19%) |
| Tobacco | 8 (31%) |
| Acute Coronary Syndrome | 7 (27%) |
| LVSD | 3 (12%) |
| LAD | 15 (58%) |
| RCA | 7 (27%) |
| LCx | 3 (12%) |
| Ramus | 1 (4%) |
| Operator Selected | 3D Assisted | p-value | |
| Foreshortening | 9.2 ± 7.6% | 2.8 ± 2.7% | 0.0003 |
| Length in mm | P-value | |
| Actual stent length | 18.6 ± 6.5 | |
| 3D assisted stent length | 19.4 ± 6 | 0.663 |
| Operator stent length | 19.2 ± 7 | 0.74 |
3D= three dimensional
Table 3: Comparison of operator predicted, 3D assisted and actual stent length used.
Figure 1: Three Dimensional coronary models reconstructed from two planar angiograms.
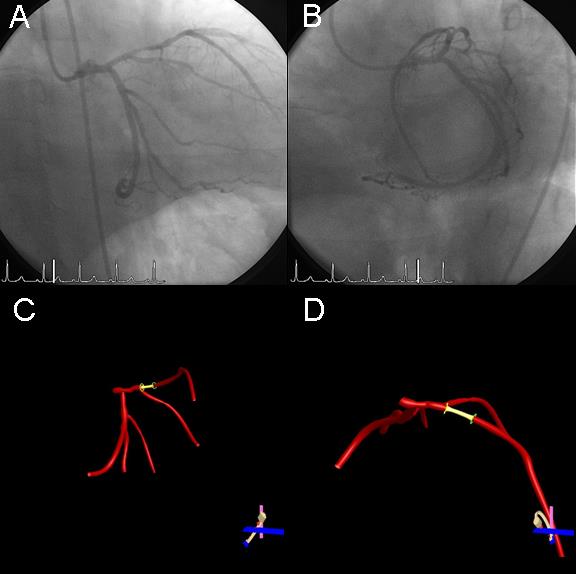
Figure 2: 3DRA analysis of the mid-LAD lesion.
A) and B) Initial RAO CAUD and LAO CAUD projections > 30° in angulation
utilized for 3D coronary model reconstruction. C) 3D model in operator
selected view of RAO 1/CAUD 39 projection with 17% foreshortening as
described on the Optimal View Map (OVM). B) Rotated 3D reconstruction
to RAO 45/CRAN 30 minimizing the foreshortening to 0% while enabling
visualization of the first diagonal branch.
3D= three dimensional, CRAN= cranial, CAUD= caudal, LAD=left anterior
descending artery, RAO= right anterior oblique
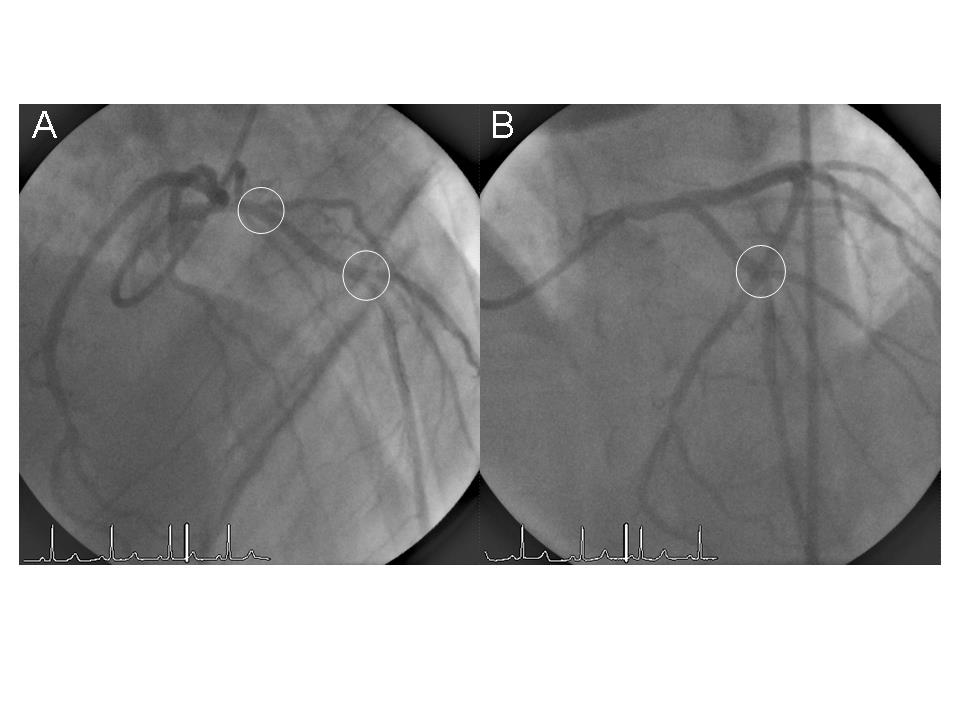
Figure 3: 3DRA assisted optimal view projection of the mid-LAD minimizing
foreshortening and overlap.
A) 3DRA assisted projection of the post-PCI mid-LAD illustrating well separated
diagonal branches (circles) with a minimally foreshortened mid-LAD.
B) Prior operator selected view of the mid-LAD with an obscured first diagonal
branch and overlapped second diagonal (circle). The impact of foreshortening
length estimation is noted with a 17% difference length of the segment
between the two diagonal branches in panel A versus panel B.
3DRA= three dimensional reconstruction, CRAN= cranial, LAD=left anterior
descending artery, PCI= percutaneous coronary intervention