Association of Cytokines IL6, IL10, IL18, TNFα in Acute Coronary Syndrome
AFFILIATIONS
AFFILIATIONS
AFFILIATIONS
AFFILIATIONS
Received Date: May 02, 2025 Accepted Date: May 15, 2025 Published Date: May 19, 2025
doi: 10.17303/jcvm.2025.11.102
Citation: Arulselvi Subramanian (2025) Association of Cytokines IL6, IL10, IL18, TNFα in Acute Coronary Syndrome. J Cardio Vasc Med 11: 1-9.
Abstract
Introduction: Cardiovascular diseases remain the leading cause of mortality and morbidity globally. A quarter of all mortality is attributable to CVD. In spite of guideline-directed treatment for patients with coronary artery diseases (CAD) that includes but not limited to the treatment of diabetes, hypertension and aggressive LDL lowering. In spite of all of this therapy, 10% of individuals had major adverse coronary events. We intended to study the role of cytokines in patients with acute coronary syndrome so as to pave a new frontier in the diagnosis and treatment of such patients.
Objectives: To determine serum cytokines levels (11--6, IL- 10, IL- 18, and TNF-alpha) and their significance in pa- tients with acute coronary syndrome ( ACS).
Methods: The study population included 120 patients with acute coronary syndrome (ACS) and 60 healthy controls. These patients were divided into two groups based on electrocardiographic evidence of ST-el- evation: 60 patients in Non-ST elevation MI (NSTEMI) (Group-I) and 60 patients in ST-elevation MI (STEM!) group(Group-2). Serial measurements of cytokines were done in 55 patients in group-I and 59 in group -2. rum levels of 11--6, 11=10, IL-18, and TNF-alpha, were measured by enzyme-linked immunosorbent assay (ELISA).
Results: Serum IL-6, 11.18, and TNF-alpha were significantly higher in ACS groups (ST EMI and NSTEMI) when compared to the control group. There was no significant difference in serum level of IL- 10 between STEMI, NSTEMI group and controls. In both, the groups, serum level of IL-IO was significantly higher and IL- 18 was significantly lower after 3 days of followup. There was no correlation between serum creatinine kinase, creatinine kinase-MB, troponin I and serum cyto- kine level in both ACS groups. There was no correlation found between serum levels of these cytokines and the site of MI (Anterior/ Inferior / Posterolateral).
Conclusion: Serum levels of cytokines (11.6, IL. 18 and TNF.alpha) were elevated in Indian patients with ACS as compared to healthy controls. Diagnostic and therapeutic role of such cytokines needs to be determined in future studies.
Keywords: Acute coronary syndrome; cytokines; Interleukins; TNF-alpha; inflammation.
Keywords: Coronary Artery; Trisomy 13; Patau Syndrome; Pregnancies; Edward Syndrome
Introduction
Cardiovascular diseases remain the leading cause of mortality and morbidity globally [ 11. A quarter of all mortality is attributable to CVD In spite of LDL lowering, of individuals had major adverse coronary events over 2 years fol. low up [21. There exists a lot ofscopes to improve the care of prog. nosis of such patients if we understand the pathogenesis of acute coronary syndrome completely. Though it was clear that it is the macrophage that gets converted to foam cell after engulfing lipid underscoring the role of the immune system in the pathogenesis of atherosclerosis since Virchow's time [3], the primordial role of the immune system and inflammation in atherosclerosis gained its importance only for last 3 decades [4]. Role of inflammation as an active process rather a passive prcxess was conceived only after the characterization of macrophage-derived cytokines [5]. Lots of available robust evidence confirms the involvement of in. flammation not only in the process of plaque vulnerability but also in the stages of recruitment of monocytes that later become foam cells in the process of plaque formation and progression [5-7]. Hence acute coronary syndrome is an inflammatory state. Understanding the function and role of the immune system in the progression of atherosclerosis into a full-blown state acute coronary syndrome may pave a new frontier in the treatment of acute coronary syndrome. Though many western literatures are available asses.sing cytokines in patients with acute coronary syn. drome, the same is not available from India. Hence, we intended to study the role of cytokines in the diagnosis of acute coronary syndrome and the role of such cytokines in prognosticating pa. tients with acute coronary syndrome.
Methods
Patients aged > 18 years admitted in the department of Cardiology were studied. Appropriate age and sex-matched healthy participants without any prior history of CAD were in. cluded as controls. We intended to study 120 patients with se- vere acute chest pain and suspected of acute coronary syndromes (A(S). Patients were divided into two groups Non-STEMI (Group-I) and STEMI (Group-2) of acute coronary syndrome (81. The diagnosis was based on positive ECG changes or enzyme elevations and angiography studies. Patients with characteristic symptoms and ST elevation 22 mm in Vl.V3 or 21 mm in other leads (in at least 2 continuous leads), ST depression consistent with posterior MI, new LBBB, established MI (old or recent): Q 20.04 s in VI -V6 or II, aVL, av or elevation of cardiac enzymes; at least two of the above criteria needed for inclusion of STEMI into the study. *Ihe Inclusion criteria of Non-STEMI had two of the following criteria, 1. Characteristic chest pain 2. ST depres- Sion > 1 mm 3. T wave inversion. 4. Positive troponin. Patients with known collagen vascular disease, advanced liver disease, renal failure, malignant disease, septicemia or other infectious disease were excluded from this study. The study was approved by the institutional Ethics Committee, and each patient gave in. formed consent, Care of the patients was not interfered by any means of this study Other than basic investigations that were done for the clinical management of the patients, we took two additional blood samples. The first sample collected immediately after admission from antecubital veins in supine position into silicon tubes with l: 9 ratio, 9ml EDTA blood. The other sam- ples collected in a similar manner 3 days later. Collected blockl samples were immediately centrifuged at 40C for 15 minutes at rpm. Divided plasma was stored at —80 oc until assayed. Estimation of cytokines (IL 6, TNF a, ILIO and ) were dong by the Enzyme-Linked Immunosorbent The study was funded by Indian Council (ICMR)
Principle of measurement of cytokines: A 5 mL of venous blood was collected on day 0 and on day 3 from each patient preferably in the morning time before 8 AM. Sample was centrifuged for 10minutes and the supernatant of the centrifuged sample was collected. Levels of IL- 6, IL-18, tumor necrosis factor-alpha (TNF-a) and IL-10 were measured in strict accordance with the instructions provided.
IL 18 was measured using Human IL 18 ELISA kit by sandwich ELISA method, The assay used two monoclonal anti- bodies against two different epitopes of human IL 18. In the wells coated with antihuman IL 18 monoclonal antitx»dy samples to be measured or standards were incubated After washing, a perox- idase.conjugated anti.human IL 18 monoclonal antitHkiy was added into the microwell and incubated. After another washing, the peroxidase substrate was mixed with the chromogen and allowed to incubate for an additional period of time. An acid solution was then added to each well to terminate the enzyme reaction and to stabilize the developed color. The optical density (OD) of each well was measured at 45() nm using a microplate reader. Ihe concentration of human IL 18 was calibrated from a dose.response curve based on reference standards, Similar ELL SA methods with the same principle were used for the other cy- tokines also,
Statistical analysisData was recorded on designed proforma and managed on excel spreadsheet. Descriptive statistics for each of the param. eters at various time points in the three groups were computed, One way analysis of variance kruskal wallis test was applied to compare mean / median of various parameters in the three groups, The relationship between post-treatment changes in cytokines as determined from peripheral blood and the treatment response was assessed using repeated aly. measures an ses. STAT 9.0 statistical software was used for statistical analysis.
Results
One hundred and twenty patients with acute coronary syndrome were studied. They were divided into two groups. Group 1 had NSTEMI and Group 2 had srEM1 (Table-I). Each group had 60 patients. In NSTEMI group (Group-I), total of 60 patients were included (l Ifemale) with mean age 55 (35-95 years). Sixty patients ( 16 female) in group 2 (STEMI group) with mean age of 54.5 years (26-82).60 individuals (17 female) were included as controls. There was no statistical difference between group 1 and group 2 with regard to risk factors for coronary artery disease. Diabetes and hypertension were present in 25% and 50 % of individuals respectively. Two-third of patients were in Killip< 3 class. Anterior wall remained the leading site of in- farction in 55% of the patient population. Similar to risk fac- tors, we did not find any difference in the Killip class, BP status, troponin elevation and site of infarction group 1 and group 2. Patients in group 1 had a significant history sugges- tive of alcohol consumption than group2. Similarly, patients in group 1 had elevated FSR and raised CK as compared to patients with group 2.
We measured TNF-alpha, 11.6, 11--10, and IL-18 on day 0 and day 3 in both groups. We intended to compare the cytokines levels measured on day 0 and day 3 amongst the par. ticipants in both groups, and also between the two groups. As compared to controls, both group I and group 2 had signifi- cantly elevated levels of all measured cytokines but IL. 10.
In group I(NSTEMI group), median IL-6 was 5.16ng/ mL (range-O-304.48) at day (hnd increased to 8.26 ng/mL (0- 324.05) on day 3 (P—NS); in addition, IL-10 increased from 1.87 ng./mL (O- 143.05) at day O to 2.96ngJmL (O- 143.57) at day3 was434.95ng/ml (23.93-4805.13) at day 0 and decreased to 123.73(0-1935.11) at day 3 (PZO.O). TNF-alfa was 33.48ng/ml (0-98.89) at day 0 to 33.48(9.41-216.43) at day 3(P-NS) (Table.2 and Figure.1&2). In group 2(STEMI group), median IL-6 was 1.07ng/ml (0-261.87) at day0 increased to 1.14 ng/mL (0-412.46) at day 3 (P-NS). IL-10 increased from the day0 value of 1.84 ng/mL (0-243.80) to 2.18 ng/mL (0- 64.70) at day3 (P-NS). IL-18 decreased from 263.08(0-4872.10) at day 0 to 108.40(0-3763.62) at day 3(p=0.002). TNF-alpha decreased from 60.68ng/ml (0-634.43) to 43.53(6.61-412.46) at day 3(p=0.008) (Table.2 and Figure.1&2).
Comparison between group 1 and group 2 showed sig- nificantly lower levels of IL-6 on day 0 and day3 in group 2 (Ta- ble.2 and Figure. I &2). In contrast, patients in group 2 had higher levels of TNF- alpha both on day 0 and day 3. No difference in ILIO and IL-18 was observed between the groups. There was no correlation found between serum levels of these cytokines and the site of MI (Anterior/ Inferior /Posterior). Other parameters which were also investigated were the relationship between the cytokine levels and creatinine kinase, creatinine kinase.MB and Tro onin I levels. 'Ihe influence of dru thera thrombolics. streptokinase, glycoprotein Ila —111b inhibitors, and inotro- pic agents on levels of cytokines were also studied. Patients in Group 2 patients had an influence of drug therapy (Thrombolyt- ics.streptokinase, Glycoprotein Ila —111b inhibitors, clopidogrel and Inotropics) only on the level of TNF-aIfa and the difference was significant (p=0.007),
Discussion
We found significantly elevated levels Of pro-inflamma- tory cytokines (IL-6, TNF-alpha and IL- 18) in patients with acute coronary syndrome without any difference in anti-inflammatory cytokine (IL-10) level. This confirms the theory Of immunoin- flammatory disease in acute coronary syndrome Dominance of T-helper-l cells was indirectly shown by elevated levels of pro-inflammatory cytokines like IL-6, IL-12and IL-18 With re- duced levels of IL- 10 191. Few studies have previously document- ed similar findings that inflammatory cytokines are increased in patients with ACS as compared to healthy controls 19-111. In contrary to our findings that suggested no significant difference in the levels of IL-10 between cases and controls, Ashraf et al found increased levels of IL-IO in patients with cardiovascu- lar diseases as compared to controls 110] while Yamashita et al found a reduced level in patients with CAD that included both patients with unstable angina and stable CAD [91. Hence the IL- 10 levels may be variable in patients with the acute coronary syn- drome. In addition to these studies, Chalikias et al proposed that it is the ratio of 11--18/11--10 b [11 | and not the individual levels that were found to be an independent predictor of adverse events (121. IL — 6 has been shown to be more sensitive and specific as compared to CRP in vascular inflammation and elevated IL -6 levels correlated with increased risk of future MI. It has been pro- posed that IL-6 cause plaque instability by modifying TNF-alpha and monocyte chemoattractant protein- 1 (MCP.I) 1131 Ridker et al showed that healthy individuals with higher interleukins had a higher chance to have future MI [14]. This again supports the role of cytokines in the initial stages of atherosclerosis. They also found IL - 6 to be an effective independent index of increased mortality in unstable CAD and is helpful in segregating patients who will be more benefitted by an invasive strategy, Similarly, IL6R signaling was shown to have a causal role in the pathogen. esis and progression of coronary heart disease. SOLID TIMIS2 [151 study revealed that patients with elevated interleukin-6 had pcx»r outcomes independent of other risk factors and biomark. ers. They also proposed that targeting IL-6 by novel therapeutic agents may create a paradigm shift in the management of pa. tients with acute coronary syndrome, In CARE study; effects of elevated TNF-alpha after many months post MI were studied. They found that patients who are clinically stable but with ele. vated TNF.alpha levels had recurrent coronary events indicating a role of the persistence of inflammatory in stability in such pa. tients 116].
There has been scarce data comparing biomarkers levels between Non STEM I and ST EMI patients. There was no difference in the level ofCRP between group I and group 2patients, Though plaque rupture is proposed as the major mechanism responsible for acute coronary syndrome both in STEMI and NSTEMI, the inflammatory cytokines released in these disease processes may not be the same Among patients with ACS, patients with STEMI had significantly elevated TNF- alpha levels and reduced levels of IL-6 as compared to patients with NSTEMI. No difference in the levels of IL- or IL-18 was observed. Similarly, the course of serum levels of such cytokines in patients with ACS is not stud- ied in Indian patients. The median IL-6 levels were significantly higher in the non-STEMI group as compared to the STEMI ACS group and in healthy control. Previously IL-6 has been shown to have a strong association with MACE and clinical outcomes in of patients with AHF and/or ACS. "Ihe difference in IL-6 between patients with NSTEMI and STEMI might be attributed to si- multaneous multiple plaque ruptures leading to many culprit le- sions that have been described more commonly in patients with NSTEMI as compared to STEML Similar statistically significant variations between NSTEMI and STEMI groups were not seen in IL-18 levels; There was no significant difference in serum IL 18 levels amongst Non-STEMI and STEMI the study done by Mallat, Henry, Fressonnet et al. [11]. IL-18 decreased significantly over three days in both group I and group 2. Though there was no difference in the levels of IL-IO between NSTEMI and STEMI patients, patients with NSTEMI showed a significant increase in the levels of IL- 10 on day 3 as compared to day-O. Studies have shown that IL- 10 is capable of down-regu- lating numerous inflammatory pathways that play an important role in the progression and stability of atherosclerotic plaque. We hypothesize that multiple simultaneous plaque rupture in such patients might have contributed to the stimulation of more re- quirement of anti-inflammatory cytokine involvement. TNFa levels were found to be higher in patients with STEMI as com- pared to NSTEMI. It decreased in STEMI patients while it did not show any change in patients with NSTEMI. This underlines the fact that patients with N STEMI might have slow indolent on- going inflammation as compared to patients with STEMI where anti-inflammation tries to overtake inflammatory cytokines. Previously, Heinisch et al showed persistently elevated TNF after 15 days in patients with ACS as compared to stable angina and healthy controls 117]. They also found elevated CRP and IL-6 in patients with ACS as compared to stable angina and healthy con- trols. Hence CAD may not be an inflammatory disease entirely but the pathogenesis of ACS revolves around inflammation.
NSTEMI and STEMI may follow different inflammato. ry pathway as patients with STEMI had higher levels of TNF and lower levels of IL-6 as compared to NSTEMI, Our study supports the previous literature that 11--6, IL-18, and TNF —a might be used as markers in patients with acute coronary events in diag. nosing them. Though it is very premature to conclude, a larger prospective study with sufficient sample size will be useful in the diagnosis and prognostication of such patients. It might also answer the finer difference between the pathogenesis between NSTEMI and STEML
Limitations of the study
Limitations of our study include a small sample size. We did not study coexisting or prior viral infections, unidenti- fied autoimmune diseases and other minor infections [ 18] that might affect the circulating cytokines level. We studied only a few cytokines but all of them are very important as compared to others. Recently IL-37 1181 has been found to be elevated in patients with ACS with poor prognosis. We have not attempted to compare different ratios amongst the participants. Effects of drugs like statin on such inflammatory cytokines has not been assessed. High dose statin therapy has been shown to decrease the level of inflammatory cytokines [19].
Conclusions
Our results suggest that ACS is associated with signif- icant elevation Of IL-6, IL-18, and TNF-alpha, 'Ihis observation indicates that different patterns of inflammatory reactions are implicated in the pathophysiology of two clinical conditions (STEMI and NON.STEMI group). Serum levels of certain cy- tokine might have some diagnostic value for ACS and can be a useful marker reflecting disease status.
Acknowledgement
We would like to thank ICMR for funding this study (F No RFC No BMS/20/2010-11). We would like to sincerely thank Renu Saini (SRF) and Rahul (Lab Attendant) who worked in this project.
- WHO | Global Action Plan forthe Prevention and Control of NCDs 2013-2020 [Internet]. [cited 2018 Dec 9].
- Natarajan P, Jaiswal S, Kathiresan S (2018) Clonal Hematopoiesis: Somatic Mutations in Blood Cells and Atherosclerosis. Circ Genomic Precis Med11:e001926.
- Virchow R (1858) Cellular Pathology. London: John Churchill.
- Libby P (2012) History of Discovery: Inflammation in Atherosclerosis. Arterioscler Thromb Vasc Biol 32:2045-2031.
- Libby P (1990) Inflammatory and immune mechanisms in atherogenesis. Vol. Vol 21. New York: Raven Press: 79—89.
- Pant S, Deshmukh A, Gurumurthy GS, Pothineni NV, Watts TE, Romeo F, et al. (2014) Inflammation and atheroscle- rosis—revisited.J Cardiovasc Pharmacol There 19:170-178.
- Kavurma MM, Rayner KJ, Karunakaran D (2017) The walking dead: macrophage inflammation and death in athero- sclerosis. CurrOpinLipidoL 28: 91-98.
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et ale (2012) Third universal definition of myo. cardial infarction. J Am CollCardiol 60: 1581-1598.
- Yamashita H, Shimada K, Seki E, Mokuno H, Daida H (2()()3) Concentrations of interleukins, interferon, and C-reac- tive protein in stable and unstable angina pectoris. Am J Cardiol 91'.133—136.
- Tabrez S, Ali M, Jabir NR, Firoz CK, Ashraf GM, Hindawi S, et al. (2017) A putative association of interleukin-IO promoter polymorphisms with cardiovascular disease. IUBMB Life 69:522-527.
- Chalikias GK, Tziakas DN, Kaski JC, Kekes A, Hatz- inikolaou EI, Stakos DA, et al. Interleukin-18/interleu- kin.10 ratio is an independent predictor of recurrent coronary events during a I -year follow-up in patients with acute coronary syndrome. Int J Cardiol 117:333-339.
- Mallat Z, Henry P, Fressonnet R, Alouani S, Scoazec A, Beaufils P, et al. Increased plasma concentrations of interleukin- 18 in acute coronary syndromes. Heart 88:467-469.
- Schieffer B, Schieffer E, Hilfiker-Kleiner D, Hilfiker A, Kovanen PT. Kaartinen M, et aL (2000) Expression of angio- tensin II and interleukin 6 in human coronary atherosclerotic plaques; potential implications for inflammation and plaque in- stability. Circulation 101: 1372—1378.
- Ridker PM, Rifai N, Stampfer MJ, Hennekens CH (2000) Plasma concentration of interleukin-6 and the risk of fu- ture myocardial infarction among apparently healthy men. Cir- culation 101: 1767-1772.
- Fanola CL. Morrow DA, Cannon CP, Jarolim P, Lukas MA, Bode C, et al. (2017) Interleukin-6 and the Risk of Adverse Outcomes in Patients After an Acute Coronary Syndrome: Ob. servations From the SOLID-TIMI 52 (Stabilization of Plaque Using Darapladib -Thrombolysis in Myocardial Infarction 52) Trial. J Am Heart Assoc- 6
- Ridker PM, Rifai N, Pfeffer M, Sacks F, Lepage S, Braun• wald E (NXX)) Elevation of tumor necrosis factor-alpha and in• creased risk of recurrent coronary events after myocardial infarc• tion. Circulation. 101:2149-2153.
- Heinisch RH, Zanetti CR, Comin F, Fernandes JL, Ramires JA, CV Serial Changes in Plasma Lev- els of Cytokines in Patients with Coronary Artery Disease. Vasc Health Risk Manag l: 245—250.
- Widen C, Holmer H, Coleman M, Tudor M, Ohlsson O, Sättlin S, et al. (2016) Systemic inflammatory impact of peri. odontitis on acute coronary syndrome. J Clin Periodontol 43: 713-719.
- Liu K, Tang Q, Zhu X, Yang X (2017) IL-37 increased in patients with acute coronary syndrome and associated with a worse clinical outcome after ST-segment elevation acute myocar- dial infarction. Clin Chim Acta Int J Clin Chem 468: 140—144.
- Wang K, Chen L, Liu L, cui Y, ZhangX, J (2018) The effects of atorvastatin on IL-6, CRR blood lipid and myocar- dial protection of interventional therapy in patients with acute myocardial infarction. Minerva Med.
FIGURE 1
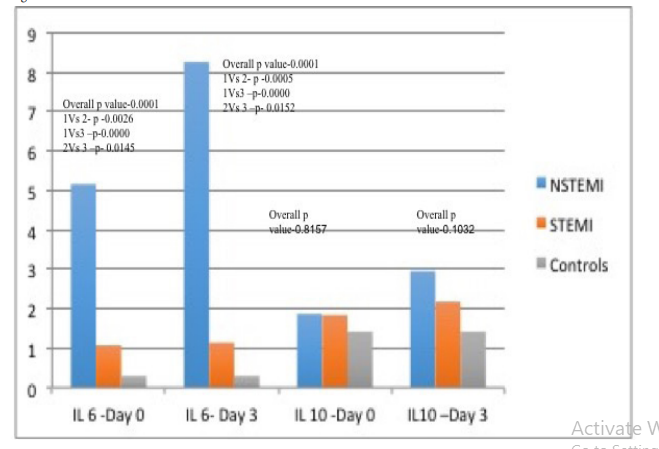
Figure 1:
FIGURE 2
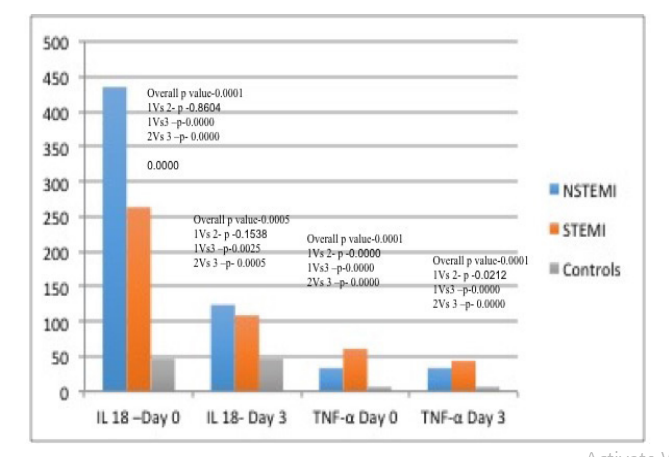
Figure 2:
Tables at a glance
Figures at a glance