The "Silent" Arrest: Diagnostic Value of the Contrast Agent Pooling (CAP) Sign in CT Pulmonary Angiography
Received Date: February 28, 2026 Accepted Date: March 11, 2026 Published Date: March 14, 2026
doi:10.17303/jcvm.2026.12.103
Citation: Noor Hasmira Bismi, Noor Diyana Osman, Mohd Syafiek Abdul Haq Saifuddin (2026) The "Silent" Arrest: Diagnostic Value of the Contrast Agent Pooling (CAP) Sign in CT Pulmonary Angiography. J Cardio Vasc Med 12: 1-5
Abstract
Cardiac arrest during diagnostic imaging is uncommon but clinically critical event. In contrast-enhanced computed tomography (CECT), circulatory collapse may manifest as dependent contrast pooling and layering within the venous system and right-sided heart chambers. These radiographic features are documented indicators of absent or severely impaired cardiac output, and their prompt identification is essential for clinical recognition.
We report the case of a 48-year-old Indian male with a chronic subdural hematoma who underwent right-sided craniotomy and clot evacuation. On the fifth postoperative day, he experienced clinical deterioration, and CT pulmonary angiography (CTPA) was performed to evaluate for suspected pulmonary embolism. Imaging revealed dependent contrast pooling within the inferior vena cava, hepatic veins, and right heart chambers, with poor opacification in the pulmonary arteries, left heart and systemic circulation. These findings suggested that cardiac arrest had already occurred prior to contrast administration. Although immediate resuscitation achieved the return of spontaneous circulation, but the patient died three days later.
This case emphasizes the critical importance of recognizing CT features of cardiac arrest.
Keywords: Cardiac Arrest, Computed Tomography Pulmonary Angiogram, Contrast Pooling, Cardiopulmonary Resuscitation, Cardiac Output.
Introduction
Cardiac arrest is a critical event demanding immediate recognition and intervention. Although it is rarely encountered during radiologic procedures, when it does occur, contrast-enhanced computed tomography (CECT) may inadvertently reveal imaging features suggestive of circulatory failure. Previous literature has highlighted the significance of dependent pooling observed in the inferior vena cava, hepatic veins, and right-sided heart chambers during contrast-enhanced CT [4]. This pattern results from gravitational settling of contrast in the absence of effective forward blood flow, often indicating cardiac arrest. Similarly, documented findings in patients undergoing CT scanning during acute hemodynamic collapse suggest these radiologic signs may serve as early indicators of cardiac arrest or impending cardiogenic shock [3]. Recent retrospective analyses of the "Contrast Agent Pooling (CAP)" sign have demonstrated a strong association with poor prognoses, reinforcing its diagnostic and prognostic utility [2].
This report presents a postoperative neurosurgical patient who experienced cardiac arrest during CT pulmonary angiography (CTPA). The CT images demonstrated classical signs of contrast pooling and layering within the venous system and right heart, characterized by absence of opacification in the pulmonary arteries and left-sided heart structures which strongly suggest that the arrest preceded contrast injection. This case emphasizes the importance of recognizing these imaging patterns to facilitate rapid diagnosis and resuscitative efforts in critical care settings.
Case Presentation
A 48-year-old male was admitted to our service with altered mental status caused by a chronic right frontoparietal hematoma. After an initial non-contrast CT confirmed a significant midline shift and cerebral edema, he underwent a right-sided craniotomy for clot evacuation. While his immediate recovery was stable, he experienced a sudden clinical decline on postoperative day five. Given the suspicion of pulmonary embolism, the patient who remained intubated and mechanically ventilated was referred for CTPA to assess for thromboembolic disease.
The CTPA was initiated using the test bolus method. A 20 mL bolus of intravenous contrast was administered, followed by a saline flush, with a small region of interest (ROI) placed in the pulmonary trunk is repeatedly imaged at short intervals to obtain time–attenuation curve to tracks contrast arrival and peak opacification timing within the pulmonary trunk.
However, the acquisition revealed persistently poor opacification of the pulmonary trunk throughout the imaging interval (Fig. 1). The axial slices demonstrated pathognomonic features of circulatory collapse including dependent layering of contrast within the right ventricle, contrast pooling within inferior vena cava (IVC) and absence of contrast with in the left ventricle and aorta, indicating lack of forward flow (Fig. 2). Due to these highly suspicious findings, the examination was extended to the abdomen, which confirmed pooling of contrast within the hepatic veins (Fig. 3).
The presence of these radiological markers provided definitive evidence that a "silent" cardiac arrest had occurred prior to the contrast injection. Upon recognizing these features, our team immediately transitioned from diagnostic imaging to active resuscitation. Although we achieved the return of spontaneous circulation (ROSC), the patient succumbed to his illness three days later in the intensive care unit.
Discussion
Cardiac arrest during diagnostic imaging procedures is uncommon but represents acritical clinical challenge. While CTPA is typically indicated for evaluation of pulmonary embolism, it may inadvertently provide definitive evidence of circulatory failure. Recognition of these specific imaging findings is essential, as they may provide the initial clinical indicator of a cardiac arrest occurring within the CT suite.
The hallmark findings in this case were dependent contrast pooling and layering with in the inferior vena cava, hepatic veins, and right heart chambers, accompanied by absent opacification of the pulmonary arteries and left heart. These features reflect a total cessation of effective cardiac output. In the absence of forward flow, the high-density contrast medium (which is heavier than blood) leading to gravitational sedimentation of contrast in the most dependent venous structures. This phenomenon is further characterized by the absence of contrast opacification in the pulmonary arteries and left- sided cardiac structures. The additional observation of contrast stasis in the right heart further underscores the severity of circulatory arrest.
The radiographic manifestations observed in this study align with established literature in the context of cardiac arrest or profound cardiogenic shock which include dependent pooling as a contrast-enhanced sign of arrest [4], while other studies confirmed its association with imminent collapse and poor prognosis [2,3]. Other study [5] emphasized these signs as early radiological markers in critically ill patients, particularly when continuous ECG monitoring is unavailable or fails to trigger an immediate alarm. Likewise, there is a case report described comparable features in trauma patients, stressing the importance of prompt recognition during emergency imaging [1].
What distinguishes this case is the evidence that cardiac arrest likely preceded the contrast injection, rather than developing during or after scanning. This “silent” arrest highlights the importance of correlating CT findings with the immediate clinical context. A misinterpretation of poor arterial opacification could delay life-saving resuscitation. This case therefore reinforces the critical role of the radiologists and clinicians in identifying CAP sign and must be vigilant for dependent venous pooling and absent arterial enhancement on CT. Prompt identification and communication of these features allows for the immediate initiation of resuscitative efforts and improve the chances of patient survival.
Conclusion
Recognizing the pathognomonic patterns of the Contrast Agent Pooling (CAP) sign during a CTPA provides immediate, visual evidence of circulatory failure. By identifying contrast stagnation in the right heart and its total absence in the arterial system, clinicians can bypass technical troubleshooting and initiate life-saving resuscitation without delay. Our experience with this case demonstrates that for postoperative or critically ill patients, maintaining a high index of suspicion for these radiologic markers is essential for detecting unrecognized cardiac arrest and facilitating a rapid transition to emergency care.
Acknowledgement
The authors would like to express their sincere appreciation to Dr. Nik Fatimah Salwati binti Nik Malek, Consultant Radiologist and Head of the Department of Radiology, Hospital Sultanah Bahiyah, for her invaluable guidance, support, and contributions throughout the preparation of this case report.
- Kao HW, Wu CJ, Lo CP, Chang WC, Chen CY (2006) Computed tomographic features of circulatory arrest. Journal of the Formosan Medical Association, 105: 359–62.
- Lee YH, Kim HJ, Park SY, Kim SH, Kim KW (2022) Contrast agent pooling (C.A.P.) sign and imminent cardiac arrest: a retrospective study. BMC Emergency Medicine, 22: p.77.
- Roth C, Thoeny HC, Leidolt L (2006) CT scan in cardiac arrest and imminent cardiogenic shock. American Journal of Roentgenology, 186: 1116–9.
- Tsai PP, Chen JH, Huang JL, Shen WC (2012) Dependent pooling: a contrast-enhanced sign of cardiac arrest during CT. American Journal of Roentgenology, 178: 1095–9.
- Hong SH, Kang EY, Huh S, Yong HS, Kim YK, Woo OH, Seo TS (2013) Emergent CT findings of impending cardiac arrest: a report of 4 cases. The American Journal of Emergency Medicine, 31: 637.e3–637.e6.
FIGURE 1
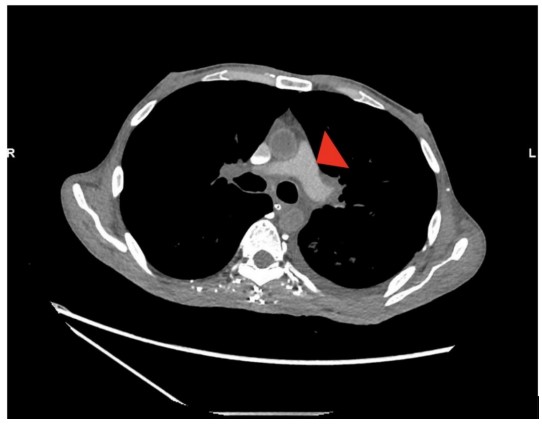
Figure 1: Poor opacification of the pulmonary trunk following the test bolus is annotated by an arrow head.
FIGURE 2
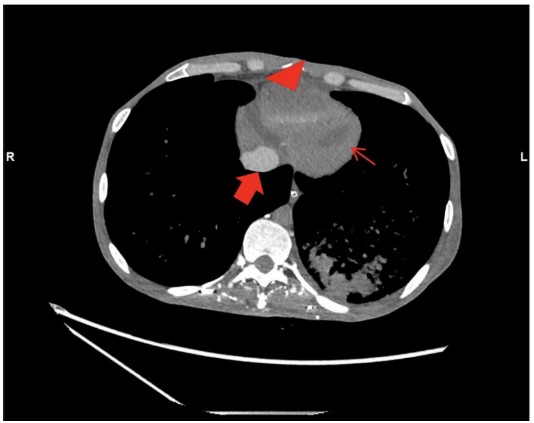
Figure 2: Dependent layering of contrast within the right ventricle is annotated by a red arrow head. Contrast pooling within inferior vena cava is annotated by a thick red arrow. Absent of contrast in the left ventricle and aorta is annotated by thin red arrows.
FIGURE 3
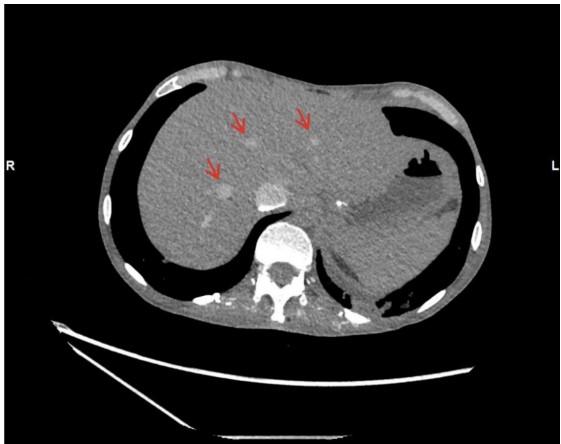
Figure 3: Pooling of contrast material in the hepatic veins annotated by thin red arrows.
Figures at a glance