Performance of MCMDM-1vWD Questionnaire for Bleeding in Saudi Patients with Coagulation Factors Deficiency
Received Date: June 06, 2021 Accepted Date: July 06, 2021 Published Date: July 08, 2021
doi: 10.17303/jcvm.2021.7.202
Citation: Khalid A AlSaleh (2021) Performance of MCMDM-1vWD Questionnaire for Bleeding in Saudi Patients with Coagulation Factors Deficiency. J Cardio Vasc Med 7: 1-15.
Abstract
Background: Coagulation factors entail a critical pathway in clot formation, and inherited deficiencies in any of these factors lead to a heterogeneous group of bleeding disorders. The current study aimed to find a correlation between bleeding symptoms and factor deficiency in Saudi Arabia.
Methods: Young Saudi adults with bleeding symptoms were questioned using a semistructured validated condensed MCMDM-1vWD questionnaire, and were tested for Prothrombin Time, activated partial thromboplastin time, and different coagulation factor levels. After testing, only those participants whose factor deficiencies were confirmed were selected for further analysis.
Results: GI bleeding and factor V were significantly co-related (P-value 0.019, Fisher exact 0.028). Out of 48 respondents with normal factor (F)V, 10.4% had GI bleeding symptoms, while out of 17 respondents with F-V deficiency, 35.3% had GI bleeding symptoms. Surgery and F-V were also significantly related (P-value 0.011, Fisher exact 0.017). Out of 48 respondents with normal F-V, 12.5% had bleeding during surgery, while out of 17 respondents with F-V deficiency, 41.2% had bleeding during surgery. We found no significant relationship between any other coagulation factor deficiency and bleeding responses, while epistaxis, oral bleeding, and surgery were significantly related to prolonged Prothrombin Time (PT); (P–value 0.02), (P–value 0.012), (P–value 0.039), respectively. Cutaneous bleeding, bleeding from minor wounds, and menorrhagia were significantly related to prolonged Activated Prothrombin Time (APTT); (P–value <0.0001), (P–value 0.038), (P–value <0.0001), respectively.
Conclusion: The current study signifies the correlation of mild bleeding symptoms with factor deficiency and highlights the higher prevalence of factor deficiencies which may need larger national surveys to increase the statistical power of such associations for better management of these patients.
Keywords: Inherited; Bleeding; Coagulation; Questionnaire
Introduction
Bleeding disorders are a group of heterogeneous, generally inherited conditions which are characterized by hemostasis abnormalities due to deficiencies in coagulation factors, leading to extended or spontaneous bleeding episodes [1,2]. The severity and frequency of these episodes depends on the specific coagulation factor deficiency. Hemophilia A and B, along with von Willebrand disease (vWBD) comprise of 95–97% of all bleeding disorders and are caused by deficiencies of factor VIII, factor IX and von Willebrand factor, respectively. All other disorders, called Rare blood disorders (RBDs), comprise the rest 3-5% of bleeding disorders [1]. Even though RBDs are prevalent in all populations, their incidence is higher in populations where consanguineous marriages are common and are caused due to factors (F) I, II, V, VII, X, XI or XIII deficiencies [3].
Distinct and robust diagnostic criteria for severe bleeding disorders are present in healthcare settings, but the diagnosis of mild bleeding disorders (MBDs) remains a challenge. As many as over 20% of the general population report at least one bleeding symptom [4] which leads to both over- and underdiagnosis of MBDs. Even though mild forms of bleeding disorders are not life-threatening, a correct diagnosis is essential to prevent and prepare for bleeding episodes during hemostatic challenges [4,5].
Occurrence of bleeding symptoms in otherwise healthy individuals is an indication of a possible underlying MBDs in many cases [3]. Over the years, several attempts have been made to standardize tools for diagnosing blood disorders with a history of bleeding symptoms in patients [6]. Common bleeding symptoms used for standardization include epistaxis, cutaneous symptoms, bleeding from minor wounds, oral bleeding, gastrointestinal bleeding, surgery, muscle/hemarthrosis, and menorrhagia [7]. Currently, a concise bleeding symptom questionnaire called condensed MCMDM-1vWD is being used to identify not only severe and common, but also mild bleeding disorders [5]. Along with MCMDM-1VWD, blood coagulation tests are also performed to confirm MBD diagnosis. In this regard, the most commonly used diagnostic assays are prothrombin time (PT) and activated partial thromboplastin time (APTT). Most of the rare bleeding disorders don’t depend on them, though, and require factor level assay [8].
The current study is aimed to evaluate the performance of MCMDM-1vWD as a tool for correctly detecting bleeding persons with MBD in the Saudi population.
Methods
Questions and subquestions asked were about bleeding symptoms, as well as about clotting factor deficiencies. Questions about bleeding symptoms pertained to: 1) Epistaxis, 2) Cutaneous Symptoms, 3) Bleeding from minor wounds, 4) Oral bleeding, 5) Gastrointestinal bleeding, 6) Surgery, 7) Muscle/hemarthrosis, and 8) Menorrhagia. The candidates were to answer 1) Yes or 2) No in response to these questions in accordance with their symptoms.
On the other hand, tests were performed to detect deficiencies for factors II, V, VII, VIII, IX, X, XI, and XIII, while Factor XII was not considered in this study because it is not commonly related with bleeding events.
Only those participants who answered positively to one of the primary questions were sampled for blood coagulation. All tests were performed at Centre of Excellence in Thrombosis and Hemostasis (CETH), Riyadh. Blood samples were collected in 10 cc sodium citrate (3.2%), 10 cc EDTA, and 5 cc sodium heparin tubes to carry out various coagulation tests. All coagulation tests, including prothrombin time (PT), activated prothrombin time (APTT), and all factor assays were performed using reagents from Stago, and STAR Max® Diagnostica Stago instrument at CETH. All samples were processed in 2–4 hours of collection.
Plasma separation was performed by centrifugation, and frozen samples were then transported to CETH for coagulation testing. For efficient testing, those with only prolonged PT (normal range: 11–14.5 seconds) were tested for the extrinsic pathways (Factors II, V, VII and X), while those with only prolonged APTT (normal range: 26–40 seconds) were tested for the intrinsic pathways (Factors VIII, IX, XI).
Only those participants whose factor deficiencies were confirmed after coagulation testing were selected for further analysis. Bleeding symptoms of participants with factor deficiency were examined, and statistical analysis was performed to determine if any correlation were present between the bleeding symptoms of participants and their coagulation factor deficiency.
Our objective was to compare bleeding questionnaire response with coagulation factor, PT and APTT related values.
Bleeding Assessment Tool
A bleeding assessment tool (BAT) for bleeding symptoms was used with coagulation factor deficiency of <50% (10). From the patient data, a symptom-specific score was generated for each bleeding symptom. We assigned the score according to the grading criteria depicted in Table 1, which was devised by the study steering committee and not available to the field physician. Finally, we summed up all symptom scores to achieve the final score.
Statistical Analysis
Descriptive statistics were computed for the categorical variables using frequency and percentages. Continuous variables were converted to categorical using normal ranges as criteria. Fishers Exact test was run to assess the significance between categorical variables related to the questionnaire and clotting factors. Odds ratios were computed between clotting factor and questionnaire, while ROC was computed between clotting factor and bleeding score. We used the software STATA v.13.0 (Stata Corp., College Station, TX, USA) in our analysis. A statistical significance threshold of P<0.05 was adopted.
Results
Out of 1,138 volunteering young adults in the initial survey, coagulation factor data were available for only 194 respondents.
A significant relationship was found between Factor V deficiency and two bleeding questions: GI bleed and Surgery (Table 2). GI bleeding and F-V were significantly related (P–value 0.028), as 6 (35.5%) out of 17 F-V deficient respondents confirmed bleeding, compared to 5 (10.4%) out of 48 with normal F-V value. Surgery and F-V were significantly related (P–value 0.017), as out of 48 respondents with normal F-V value only 6 (12.5%) had bleeding during the surgery, while out of 17 F-V deficient respondents, 7 (41.2%) had bleeding during surgery
Significant relationship was found between bleeding symptom responses and PT and APTT values (Table 3). Epistaxis response, oral bleeding, and surgery were significantly related to PT (P–value 0.02, 0.012, and 0.039, respectively). Cutaneous response, bleeding from minor wounds, and menorrhagia were significantly related to APTT (P–value <0.0001, 0.038, and <0.0001 respectively).
Table 4 shows the score ranges for each symptom and its likelihood. We show the highest likelihood for a factor when a score value is presented. For most clotting factors, the likelihood is highest for score 1.
Figure 1 shows odds ratios of Factor V to symptoms, with GI bleeding and surgery having an odds ratio values greater than 5. Figure 2 shows odds ratios of Von Willebrand factor activity as <2 for epistaxis and cutaneous symptoms, which does not reach the threshold of significance in predicting bleeding.
Figure 3 shows the bleed score and Factor V with ROC AUC 0.6 for Surgery, showing the predictability for surgical bleeding. For a sensitivity of 0.5, the specificity is 0.8. Figure 4 shows Factor V and PT prolongation with ROC AUC 0.67 and 0.5 for GI bleeding, respectively, again showing Factor V deficiency as a predictor of GI bleed. For a sensitivity of 0.55, the specify is 0.8.
Discussion
Rare bleeding disorders (RBDs) are caused by mainly autosomal recessive inherited clotting factor deficiencies of Factors I (fibrinogen), II (prothrombin), V, VII, X, XI, and XIII, as well as combined FV + FVIII. Coagulation factor deficiencies comprise of congenital bleeding disorders with a heterogeneous phenotype. These deficiencies can lead to sudden and chronic bleeding diathesis, which poses a significant impact on quality of life and can be lethal in rare instances. Quantification of bleeding disorders based upon the symptom is itself a challenging task. We utilized a condensed MCMDM-1vWD bleeding questionnaire for efficient screening of bleeding symptoms. The bleeding questions were related to epistaxis, cutaneous symptoms, bleeding from minor wounds, oral, gastrointestinal, surgery, muscle/hemarthrosis, and menorrhagia. To build the correlation insight, we tested blood samples for F II, V, VII, VIII, IX, X, XI, and XIII. A significant correlation was found between gastrointestinal bleeding and Factor V deficiency (P-value 0.019, Fisher exact 0.028); and surgery-related questions and factor V deficiency (P-value 0.011, Fisher exact 0.017).
Coagulation factor V is a glycoprotein that participates in the formation of the prothrombinase complexes, a critical step for clot formation (11). Incidence of Factor V deficiency (Owren’s disease or parahemophilia) is 1 /1,000,000 and is considered a rare bleeding disorder in the general population (12). Although the life-threatening manifestation is rare with factor V deficiency, however, it is manifested in a plethora of bleeding events including mucosal bleeding as the most common manifestation.
Peyvandi, et al. in reporting the results from the European Network of Rare Bleeding Disorders described that on linear regression analysis, there was a strong association between clotting factor activity level and clinical bleeding severity for fibrinogen, F-X, XIII, and combined V and VIII deficiencies. A weaker association was present for V and VII deficiencies [16,17]. These factor deficiencies also have been previously reported in the Saudi population in various regions. Ahmed MA, et al. reported FVII and X deficiency in Eastern Province [13] while Al-Sharief, et al. reported FXIII deficiency in Riyadh [14]. Al-Fawaz, et al. reported FXI, V, and VII deficiency [15] and Madkhali, et al. reported F-II, V, VII, X, XI, and XIII deficiencies [16]. Through a hematological panel assay, Al Numair, et al. was able to identify eleven FV deficiency patients with mutations [17].
A total of 321 cases of rare clotting factor deficiency were reported by Shetty, et al. from India, with 30% of patients having FXIII deficiency, 15.6% of patients with FX, 15% cases with FVII deficiency, 12.1% with fibrinogen deficiency, 9% with FXI deficiency, 5.6% with combined V and VIII deficiency, and 2.1% with congenital multiple vitamin K‐dependent coagulation factor deficiency [18].
Epistaxis is often presented as a common emergency, and routine coagulation studies such as PT and APTT have been questioned as a reliable marker for diagnosis [19]. The current study suggests the notion that prolonged PT and APTT in the presence of bleeding symptoms could be used as screening tests to predict underlying factor deficiency. Yet the absence of abnormal PT APTT doesn’t rule out clotting factor deficiency. In contrast to our study, Elden, et al. reported a limited value of PT and APTT in predicting bleeding disorders in children, arguing that PT, APTT only identify 20% of cases with bleeding disorders [20], while Al Zahrani, et al. demonstrated limited predictability power of routine coagulation testing in pediatric patients undergoing surgery [21]. Such discrepancies signify the ethnic distribution of hereditary elements and indicate the importance of regional studies. The rationale of the current study lies in the fact that specific bleeding symptoms may correlate with underlying genetic defects such as coagulation factor deficiency. A significant relationship between certain bleeding symptoms (GI and Surgery) with factor V deficiency warrant that such association must be studied nationwide to establish a bleeding questionnaire as a diagnostic tool.
Conclusion
Identification of clotting factor deficiency can significantly improve clinical management with better patient outcomes. The current study is an epidemiological survey which aimed to explore the correlation of bleeding symptoms with clotting factor deficiency, and a significant correlation was found between factor V deficiency and bleeding from GI and surgery independently. These correlations demand further studies with greater sample size to increase the power of such associations and establish validated methods to predict factor deficiencies resulting in improved management for patients with bleeding symptoms.
Declarations
Authors’ Contribution
KS & TO designed & developed the study. Both authors were responsible for contents & authenticity. NAN, AS, MZ, AA oversaw data collection, data entry. NAO, EA, NB, AT carried out final review of data and analysis. FZ, FA, AAA were responsible for direction of the study team, and facilitation of the project plan.
Funding and Source of Support
KACST (408-34)
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of King Faisal Specialist Hospital and Research Center, Kingdom of Saudi Arabia, with approval # RAC KFSHRC (2130036).
Consent for publication
All authors consent for publication.
Availability of data and materials
Furnished upon request.
Competing interests
None declared.
- Castaman G, Linari S (2017) Diagnosis and treatment of von Willebrand disease and rare bleeding disorders. J clin med 6: 45.
- Rhynders PA, Sayers CA, Presley RJ, Thierry JM (2014) Providing young women with credible health information about bleeding disorders. Ame J preventive med 47: 674-80.
- James P, Salomon O, Mikovic D, Peyvandi F (2014) Rare bleeding disorders–bleeding assessment tools, laboratory aspects and phenotype and therapy of FXI deficiency. Haemophilia 20: 71-5.
- Boender J, Kruip M, Leebeek F (2016) A diagnostic approach to mild bleeding disorders. J Thrombosis Haemostasis 14: 1507-16.
- Bowman M, Mundell G, Grabell J, Hopman W, Rapson D, et al. (2008) Generation and validation of the Condensed MCMDM‐1VWD Bleeding Questionnaire for von Willebrand disease. J thrombosis haemostasis 6: 2062-6.
- Moenen F, Nelemans P, Schols S, Schouten H, Henskens Y, et al. (2018) The diagnostic accuracy of bleeding assessment tools for the identification of patients with mild bleeding disorders: a systematic review. Haemophilia 24: 525-35.
- Peyvandi F, Di Michele D, Bolton-Maggs P, Lee C, Tripodi A, et al. (2012) Classification of rare bleeding disorders (RBDs) based on the association between coagulant factor activity and clinical bleeding severity. J thrombosis haemostasis: JTH 10: 1938.
- Chandler E, Kakkar N, Kaur R (2019) Comparison of Rapid Centrifugation Technique with Conventional Centrifugation for Prothrombin Time (PT) and Activated Partial Thromboplastin Time (APTT) Testing. Ind J of Hematology Blood Transfusion 35: 161-6.
- Tosetto A, Rodeghiero F, Castaman G, Goodeve A, Federici A, et al. (2006) A quantitative analysis of bleeding symptoms in type 1 von Willebrand disease: results from a multicenter European study (MCMDM‐1 VWD). J Thrombosis Haemostasis 4: 766-73.
- Rydz N, James PD (2012) The evolution and value of bleeding assessment tools. J Thrombosis Haemostasis 10: 2223-9.
- Kane WH, Majerus PW (1981) Purification and characterization of human coagulation factor V. J Biolog Chem 256: 1002-7.
- Tabibian S, Shiravand Y, Shams M, Safa M, Gholami MS, et al. (2019) editors. A comprehensive overview of coagulation factor V and congenital factor V deficiency. Seminars in thrombosis and hemostasis; 2019: Thieme Medical Publishers.
- Ahmed MA, Al-Sohaibani M, Al-Mohaya S, Sumer T, Al-Sheikh E, et al. (1988) Inherited bleeding disorders in the Eastern Province of Saudi Arabia. Acta haematologica 79: 202-6.
- Al-Sharif FZ, Aljurf MD, Al-Momen AM, Ajlan AM, Musa MO, et al. (2002) Clinical and laboratory features of congenital factor XIII deficiency. Saudi Med J 23: 552-4.
- Al-Fawaz IM, Gader AM, Bahakim HM, Al-Mohareb F, Al-Momen AK, et al. (1996) Hereditary bleeding disorders in Riyadh, Saudi Arabia. Annals Saudi med16: 257-61.
- Madkhali I, Owaidah T, Riash MA, Naser R, Al-Zahrani H (2012) Rare inherited clotting factor deficiencies: A single-center experience. Journal of Applied Hematology 3: 36.
- Al-Numair NS, Ramzan K, Saleh M, Alzahrani H, Tarawah A, et al. (2019) First description of the molecular and clinical characterization of hereditary factor V deficiency in Saudi Arabia: report of four novel mutations. Blood Coagulation & Fibrinolysis 30: 224-32.
- Shetty S, Shelar T, Mirgal D, Nawadkar V, Pinto P, et al. (2014) Rare coagulation factor deficiencies: a countrywide screening data from India. Haemophilia 20: 575-81.
- Awan MS, Iqbal M, Imam SZ (2008) Epistaxis: when are coagulation studies justified? Emergency Med J 25: 156-7.
- Elden L, Reinders M, Witmer C (2012) Predictors of bleeding disorders in children with epistaxis: value of preoperative tests and clinical screening. Int J ped otorhinolaryngology 76: 767-71.
- Alzahrani A, Othman N, Bin-Ali T, Elfaraidi H, Al Mussaed E, et al. (2019) Routine preoperative coagulation tests in children undergoing elective surgery or invasive procedures: are they still necessary? Clinical Medicine Insights: Blood Disorders 12: 1179545X18821158.
FIGURE 1
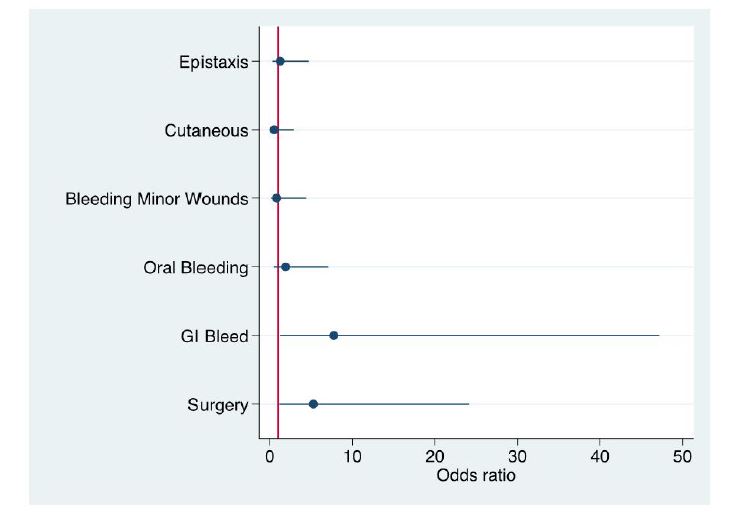
Figure 1: Odds-ratio for F-V compared to bleeding responses
FIGURE 2
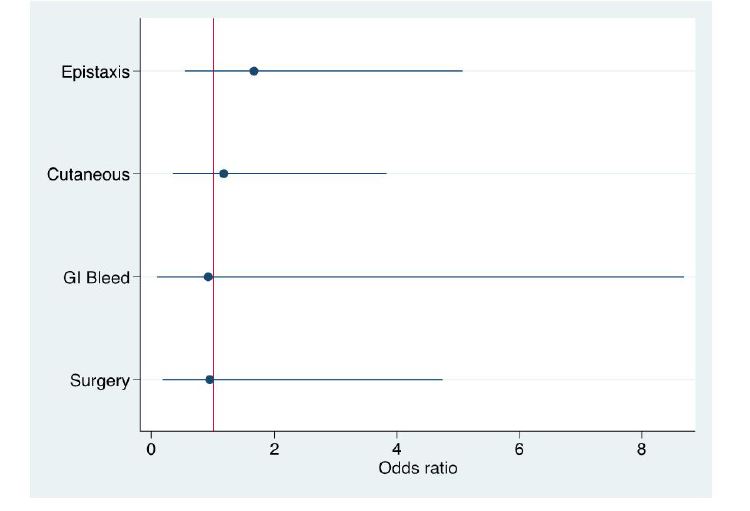
Figure 2: Odds ratio of vWF Activity against bleeding responses
FIGURE 3
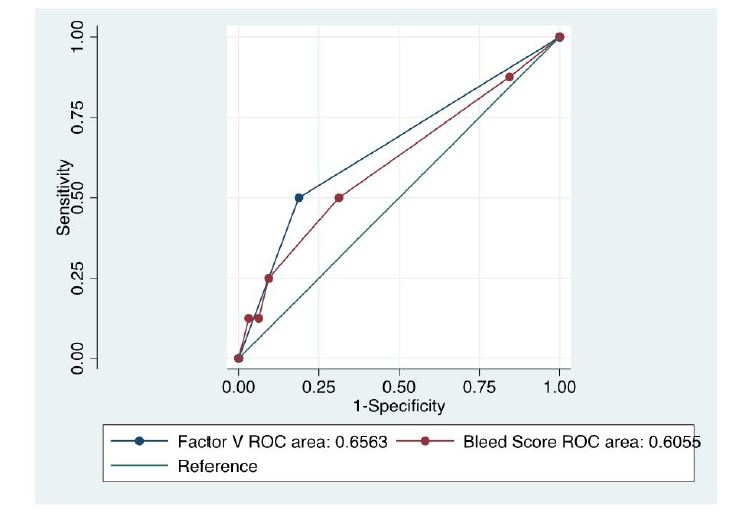
Figure 3: ROC of Surgery response to Factor-V and Bleed Score (binary variables)
FIGURE 4
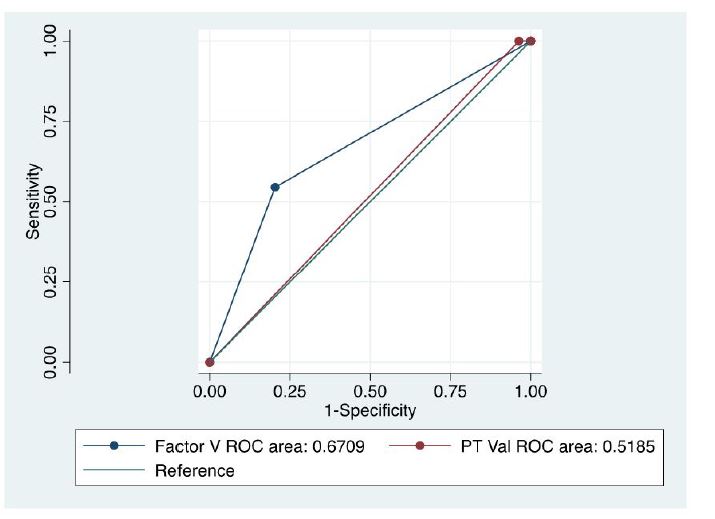
Figure 4: Serum ANGPTL4 levels in patients with OSA before and after nasal CPAP treatment
Tables at a glance
Figures at a glance