Multiple Arterial Bypass Graft Surgery Vs Drug-Eluting Stent in Patients with Three-Vessel or Left Main Coronary Artery Disease: A Meta-Analysis of Observational Studies
Received Date: July 21, 2023 Accepted Date: August 21, 2023 Published Date: August 24, 2023
doi: 10.17303/jcvm.2023.9.102
Citation: Yanwei Wang, Yutao Wu, Yanqin Li, Xi Yang (2023) Multiple Arterial Bypass Graft Surgery Vs Drug-Eluting Stent in Patients with Three-Vessel or Left Main Coronary Artery Disease: A Meta-Analysis of Observational Studies. J Cardio Vasc Med 9: 1-13
Abstract
Background: The choice of multiple arterial bypass graft surgery (MAG) versus drug-eluting stent (DES) among patients with multivessel coronary artery disease (MCAD) or left main coronary artery disease (LMCAD) continues to be challenging.
Objectives: The aim of this study was to evaluate the efficacy and safety of MAG with DES- percutaneous coronary intervention (PCI) in patients with multivessel coronary artery disease or left main coronary artery disease.
Methods: PubMed, EMBASE and Clinical trials were systematically searched for studies which reported the clinical outcomes of MAG versus DES-PCI in patients with three-vessel or left main coronary artery disease. Clinical endpoints including all cause death, myocardial infarction (MI), stroke, repeat revascularization and major adverse cardiac and cerebrovascular events (MACCE) were assessed.
Results: From 2000 to 2023, 13 clinical studies comprising 17255 patients were identified. Pooled results shown similar safety between MAG and DES-PCI after short-term follow up. While, MAG was associated with significant lower incidence of death from any cause, MI, repeat revascularization and MACCE with long-term follow up.
Conclusions: Among patients with multivessel coronary artery disease or left main coronary artery disease, MAG led to comparable clinical outcomes to PCI with short-term follow up, and shown superior clinical outcomes after long-term follow up.
Keywords: Multiple Arterial Bypass Graft Surgery; Percutaneous Coronary Intervention; Bilateral Internal Thoracic Arterial; Drug-Eluting Stent
Introduction
Optimal revascularization approaches for patients with multivessel coronary artery disease (MVCAD) or left main coronary artery disease (LMCAD) remain controversial despite multiple randomized trials and retrospective series [1,2]. The choice of coronary artery bypass graft surgery (CABG) versus percutaneous coronary intervention (PCI) among patients with MVCAD or LMCAD continues to be challenging. Overall, data from both randomized and observational studies suggest that CABG should be preferred over PCI in patients with MVCAD [3,4]. US and European guidelines recommend CABG for patients with three-vessel or two-vessel disease with proximal left anterior descending CAD (class I); while PCI recommend as an option of uncertain benefit (class IIb) in this population [5,6]. As a less invasive approach, PCI benefit from earlier recovery, lower periprocedural risk, smaller periprocedural MI, less risk of procedural complications and periprocedural bleeding, was usually considered in patients unsuitable for operation. Recently, advances in PCI techniques, such as physiologic assessment of lesions, intravascular imaging guidance, use of a new-generation stent have resulted in improved degree of revascularization [7]. PCI with stent implantation for LMCAD had become technically feasible and had shown favorable clinical outcomes, especially in people with low or intermediate SYNTAX scores [8]. Improved long-term mortality with drug-eluting stent (DES)-PCI helped to drive increased use of PCI in the treatment. What is more, PCI has achieved recognition as a reasonable therapeutic alternative to CABG for unprotected LMCAD [9]. In a recent pooled analysis of 11 randomized trials comparing CABG with PCI, 5-year all-cause mortality was not significantly lower in CABG group without diabetes [4]. On the other hand, CABG offers the advantage of bypassing long segments of disease or diffuse disease and complete revascularization. Which is a more durable procedure with less repeat revascularization. CABG has also evolved significantly over the last two decades with increasing utilization of multiple arterial grafts (MAG) and more sophisticated surgical revascularization techniques [10]. Compelling evidence has rapidly accumulated over the past decade suggesting a second arterial graft improves intermediate and long-term outcomes substantially compared with those of single arterial-CABG [11]. It’s important to consider different surgical techniques when comparing outcomes of CABG with PCI. To further confirm the efficacy of MAG over DES-PCI, we performed meta-analysis focused on contemporary outcomes after MAG or DES-PCI in patients with MVCAD and/or LMCAD.
Methods
Systematic database search was performed on PubMed, EMBASE and Clinicaltrials.gov for relevant articles. The key words we used for screening included following terms: “percutaneous coronary intervention”, “PCI”, “drug-eluting stent”, “DES”, “multiple arterial bypass graft”, “MAG”, “bilateral internal thoracic arterial” and “BITA”. The references of relevant studies and reviews, editorials, and letters, together with related conference abstracts were also searched.
Inclusion criteria for study selection were clinical trials directly comparing clinical outcomes between PCI using DES and MAG in patients with left main coronary artery disease or multivessel coronary artery disease. All titles and abstracts were screened. If either reviewer judged that the study could meet the inclusion criteria, we assessed eligibility using the full text. We excluded studies that were non-human or without clinical data. We also excluded studies using bare metal stent or balloon angioplasty mixed with DES in PCI group.
The efficacy endpoints of the analysis include: (a) Death from any cause, (b) Cardiovascular death, (c) non cardiovascular death, (d) Myocardial infarction (MI), (e) Stroke, (f) Repeat revascularization and (g) Major adverse cardiac and cerebrovascular events (MACCE). All of them were defined according to respective study definition.
Two investigators independently assessed reports for eligibility at title and/or at abstract level, with divergences resolved by a third reviewer; studies that met inclusion criteria were selected for further analysis. The risk of bias was evaluated by the same two reviewer reviewers, in accordance with The Cochrane Collaboration methods [12].
Data was analyzed using the Review Manager 5.3 statistical software. Reported event frequencies were used to calculate risk ratios (RR) with 95% confidence intervals (CI). Heterogeneity of the trial results was quantified with the Chi2 heterogeneity statistic, inconsistency assessed by means of I2 . Results were reported as the p value of the Chi2 test (p < 0.05 for heterogeneous results) and percent of the I 2 . Interpretation of the I2 was made by assigning attribute of low, moderate, and high in case of 0–25%, 50–75% and more than 75%, respectively. The trials included in the meta-analysis had heterogeneous patient cohorts with differing clinical presentations, treatment indications, coronary anatomy, and procedural characteristics, we used a random effects model based on associated heterogeneity, with the latter used when I2 >50%. To study the relevance of publication bias, funnel plots were constructed plotting the trial results against their precision.
Results
After deduplication, screening of titles and abstracts, and full text review based on inclusion and exclusion criteria, 13 observational studies involving 17255 patients were qualified for the analysis [13-25] (Figure1). The detailed characteristics of the included studies are shown in Supplementary table1. Studies varied according to the year published clinical presentation and duration of follow up. In general, 9292 (53.9%) patients were treated with DES-PCI, while 7963 (46.1%) treated with MA-CABG. 7 trials using bilateral internal thoracic arterial (BITA) in CABG arm. In PCI with DES implantation, 4 studies only used second-- generation DES.
We first investigated the short-term clinical outcomes (in-hospital or 30 days) of MAG and PCI. MAG group was associated with non-significantly lower incidence of all-cause death (RR 0.67; 95%CI: 0.34-1.31; p=0.24; I2 =61%), MI (RR 0.82; 95%CI: 0.35-1.94; p=0.66; I2 =66%). However, MAG might increase the rate of stroke with no significant difference (RR 2.86; 95%CI: 0.84-9.78; p=0.09; I 2=0%), MACCE (RR 1.48; 95%CI: 0.94-2.34; p=0.09; I 2=0%) and significant increase the incidence of bleeding events (RR 3.14; 95%CI: 1.78-5.53; p<0.0001; I2 =0%) (Figure2).
For the long-term clinical outcomes, the cumulative incidence of all cause death was 7.09% in the MAG group and 17.6% in the PCI group with significant difference (RR 0.40; 95%CI: 0.30-0.53; p<0.00001; I2 =84%). MAG also have significant benefit in cardiovascular death (RR 0.22; 95%CI: 0.06-0.80; p=0.02; I2 =0%), non- cardiovascular death (RR 0.16; 95%CI: 0.03-0.88; p=0.04; I2 =0%), my ocardial infarction (RR 0.29; 95%CI: 0.14-0.60; p=0.0008; I2 =83%), repeat revascularization (RR 0.17; 95%CI: 0.11-0.27; p<0.00001; I2 =91%) and MACCE (RR 0.42; 95%- CI: 0.38-0.47; p<0.00001; I2 =47%). MAG might decrease the incidence of stroke (RR 0.39; 95%CI: 0.10-1.58; p=0.19; I2 =77%) with no significant difference (Figure3).
Subgroup analysis for MAG with first-generation DES-PCI was performed. After long-term follow up, MA-- CABG was associated with significant lower incidence of MACCE, all cause death and repeat revascularization. MA-- CABG might decrease the incidence of stroke without significant difference. Same results were confirmed when comparing MA-CABG with second-generation DES-PCI. Pervious study demonstrated bilateral internal thoracic artery grafting is superior to other forms of multiple arterial grafting in providing survival benefit [26]. We pooled results in trials using BITA in CABG arm, CABG with BITA also superior to PCI in MACCE, all cause death, stroke, MI and repeat revascularization (Table1).
Bias assessment showed low-to-moderate risk of bias in all studies. The funnel plot did not show asymmetry consistent with publication bias (Figure 4).
Discussion
Optimal revascularization approaches for patients with multivessel coronary artery disease or left main coronary artery disease remain controversial. Advances in PCI techniques have resulted in improved degree of revascularization and clinical outcomes.
As a less invasive approach, PCI offers quicker recovery, lower incidence of early adverse cardiovascular events and possibly short-term reduced risk of stroke. While higher rate of residual angina was seen in patients treated with PCI that contributes to higher rates of repeat revascularization. The SYNTAX II trial compared patients undergoing PCI with contemporary techniques, shown improved clinical outcomes even compared with the SYNTAX I CABG arm [27]. In a recent pooled analysis of 11 randomized trials comparing CABG with PCI, 5-year all-cause mortality was significantly lower after CABG in patients with diabetes but not in those without diabetes [4]. As the gap in the treatment effect between two strategies has gradually diminished. The less invasive interventional approach has been recognized as a reasonable therapeutic alternative for LMCA disease instead of CABG with the widespread use of drug-eluting stents [28,29]. However, the recommendation of optimal revascularization approaches for patients with LMCAD also were debated.
The pathophysiological effects of CABG were quite different with PCI. The cardioprotective superiority of CABG was postulated to result from bypass grafts to the mid-coronary vessels that not only treat culprit lesion, but also afford prophylaxis against new proximal disease by mitigating the impact of plaque rupture and atherothrombosis on future events. While, CABG is associated with delayed recovery, longer length of stay in hospital and issues with healing and infection, in addition to higher costs. Nevertheless, outcomes following CABG may vary according to the type of grafts used. Pervious retrospective and pooled observational studies have shown lower long-term mortality when both internal-thoracic-artery grafts are used for CABG than single internal-thoracic-artery graft CABG [30-33]. There remains an ambiguity regarding the superiority of multiple arterial grafts compared to single arterial grafts (SAG) in randomized controlled trials. ART trial concluded there was no significant between-group difference in the rate of death from any cause at 10 years in the intention-to-treat analysis [34]. Changal et al also shown similar survival advantage between MAG and SAG, but MAG has better revascularization and stroke outcomes in randomized data [35]. When directly compares short-term/long-term outcomes of PCI vs CABG with MAG, current evidence was limited and conflicting.
In our analysis, we included studies direct compare clinical outcomes of MAG with PCI using DES in MVCAD/LMCAD. Most of pooled results shown significant benefit in MAG arm with long-term follow up. As previous study demonstrated the use of all-cause mortality reduces the risk of adjudication bias. In our study, MA-CABG significant decrease the incidence of all cause death (RR 0.40; 95%CI: 0.30-0.53; p<0.00001; I2 =84%), while there was high heterogeneity in the overall pooled result. The high heterogeneity was mostly associated with the study published by Nambiar. The heterogeneity between pooled studies decreased when exclude this study (RR 0.47; 95%CI: 0.38-0.59; p< 0.00001; I2 =69%), without change the result. Nambiar et al retrospective 940 patients underwent multivessel minimally invasive cardiac surgery (MICS) CABG via a left mini-thoracotomy as MA-CABG arm, giving excellent short-term and long-term mortality. When propensity score matched with PCI arm from SYNTAX trial, the mortality of CABG arm was significantly lower than PCI arm (0.9% vs 11.4%). This result might partly because of higher rate of complete revascularization in CABG arm (97% vs 56%). Incomplete revascularization is common after PCI in patients with three-vessel disease and/or left main coronary artery disease, the degree of incompleteness was associated with long-term mortality [36]. Our study also demonstrated superiority of MAG-CABG in patients with three-vessel disease and/or left main coronary artery disease even comparing with second-generation DES. CABG might still the most optimal revascularization approaches for these patients.
Our study has several limitations. First, there was no randomized clinical trials direct compare MAG with DES-PCI, we included observational and observational propensity-score matched studies in this meta-analysis, which was prone to selection bias and confounding. Indeed, the complexity of equipoise and influence of surgical expertise are herculean challenges for randomized clinical trials [37]. while traditional RCTs have low external validation, high costs, need for numerous staff and heavy documentation leading to low adherence from surgeons [38]. As the observational study represent the everyday practice, our pooled results from these studies might also give a primary conclusion. Second, half of included studies using first-generation DES in PCI arm, which may lead to inferior clinical outcomes. However, in our subgroup analysis, the result from MAG-CABG vs. second-generation DES was consistent with the result from MAG-CABG vs. first-generation DES. Third, most studies compare MAG vs PCI included patients with left main or multivessel coronary artery disease at the same time. In our study, we performed a meta-analysis in study level and included these patient groups together. Recent study demonstrated lesion site (ostial or shaft vs. distal bifurcation) and PCI technique (1-stent vs. 2-stent) mainly affected the efficacy of intervention therapy [39]. LMCAD might a specify situation when compare surgery and intervention. It is still doubt whether the long-term adverse events following the use of a single stent for distal LMCA lesions can be comparable with CABG. Unfortunately, without data from patient level, we cannot perform a detailed analysis with separated situation (MVCAD/LMCAD). As CABG mainly performed in both patients with left main or multivessel coronary artery disease in the real-world practice, our analysis given a general conclusion. What is more, our analysis could not control for variations in clinical practice in different study centers, although our funnel plot did not show significant publication bias between included studies, publication bias may still exist despite our best efforts to conduct a comprehensive search.
Conclusion
Our meta-analysis showed that among patients with multivessel coronary artery disease or left main coronary artery disease, multi arterial coronary artery bypass graft was associated with comparable clinical outcomes in short-term, and superior efficacy with long-term follow up compared with PCI. As the existence of a learning curve and perception of increased sternal wound problems were still the concerns over MAG. These findings should be extended to large, multi-site randomized controlled trials.
Funding
None.
Disclosures
The authors have no conflicts of interest to disclose.
- Burack JH (2008) Drug-eluting stents vs. coronary-artery bypass grafting. N Engl J Med 358: 2643.
- Mulukutla SR, Gleason TG, Sharbaugh M et al. (2019) Coronary Bypass Versus Percutaneous Revascularization in Multivessel Coronary Artery Disease. Ann Thorac Surg 108: 474-80.
- Sipahi I, Akay MH, Dagdelen S, Blitz A, Alhan C (2014) Coronary artery bypass grafting vs percutaneous coronary intervention and long-term mortality and morbidity in multivessel disease: meta-analysis of randomized clinical trials of the arterial grafting and stenting era. JAMA Intern Med 174: 223-30.
- Head SJ, Milojevic M, Daemen J et al. (2018) Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 391: 939-48.
- Windecker S, Kolh P, Alfonso F et al. (2015) 2014 ESC/EACTS guidelines on myocardial revascularization. EuroIntervention 10: 1024-94.
- Patel MR, Calhoon JH, Dehmer GJ et al. (2017) ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 Appropriate Use Criteria for Coronary Revascularization in Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. J Am Coll Cardiol 69: 2212-41.
- Hu X, Wang Y (2021) Importance of complete revascularization and surgical techniques when comparing outcomes of CABG with PCI. Am Heart J 236: 107-8.
- Stone GW, Sabik JF, Serruys PW et al. (2016) Everolimus-Eluting Stents or Bypass Surgery for Left Main Coronary Artery Disease. N Engl J Med 375: 2223-35.
- Harskamp RE, Park DW (2015) Stenting versus surgery for significant left main disease. Curr Cardiol Rep 17: 18.
- Boden WE, Caterina R, Taggart DP (2021) Is there equivalence between PCI and CABG surgery in long-term survival of patients with diabetes? Importance of interpretation biases and biological plausibility. Eur Heart J.
- Buxton BF, Shi WY, Tatoulis J, Fuller JA, Rosalion A, Hayward PA (2014) Total arterial revascularization with internal thoracic and radial artery grafts in triple-vessel coronary artery disease is associated with improved survival. J Thorac Cardiovasc Surg 148: 1238-43.
- Higgins JP, Altman DG, Gotzsche PC et al. (2011) The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343: d5928.
- Rocha RV, Fang J, Tam DY et al. (2021) Multiple arterial coronary bypass grafting is associated with better survival compared with second-generation drug-eluting stents in patients with stable multivessel coronary artery disease. J Thorac Cardiovasc Surg.
- Bianco V, Mulukutla S, Aranda-Michel E et al. (2023) Coronary Artery Bypass With Multiarterial Grafting vs Percutaneous Coronary Intervention. Ann Thorac Surg 115: 404-10.
- Locker C, Mohr R, Lev-Ran O et al. (2004) Comparison of bilateral thoracic artery grafting with percutaneous coronary interventions in diabetic patients. Ann Thorac Surg 78: 471-5.
- Herz I, Moshkovitz Y, Loberman D et al. (2005) Drug-eluting stents versus bilateral internal thoracic grafting for multivessel coronary disease. Ann Thorac Surg 80: 2086-90.
- Herz I, Moshkovitz Y, Braunstein R, et al. Comparison between multivessel stenting with drug eluting to the LAD and bilateral internal thoracic artery grafting. Heart Surg Forum. 2006;9(1):E522-527.
- Moshkovitz Y, Mohr R, Medalion B et al. (2012) Drug-eluting stents compared with bilateral internal thoracic artery grafts for diabetic patients. Ann Thorac Surg 94:1455-62.
- Habib RH, Dimitrova KR, Badour SA et al. (2015) CABG Versus PCI: Greater Benefit in Long-Term Outcomes With Multiple Arterial Bypass Grafting. J Am Coll Cardiol 66: 1417-27.
- Benedetto U, Caputo M, Vohra H, Bryan A, Angelini GD (2016) State of the art in coronary revascularization: Everolimus eluting stents versus multiple arterial grafting. Int J Cardiol 219: 345-9.
- Locker C, Schaff HV, Daly RC et al. (2016) Multiple arterial grafts improve survival with coronary artery bypass graft surgery versus conventional coronary artery bypass grafting compared with percutaneous coronary interventions. J Thorac Cardiovasc Sur 152: 369-79.
- Raja SG, Ilsley C, De Robertis F et al. (2018) Mid-to-- long term mortality following surgical versus percutaneous coronary revascularization stratified according to stent subtype: An analysis of 6,682 patients with multivessel disease. PLoS One 13: e0191554.
- Nambiar P, Kumar S, Mittal CM, Sarkar IC (2019) Outcomes of Bilateral Internal Thoracic Arteries in Minimally Invasive Coronary Artery Bypass Grafting With Analogy to the SYNTAX Trial. Innovations (Phila) 14: 227-35.
- Thuijs D, Head SJ, Stone GW et al. (2019) Outcomes following surgical revascularization with single versus bilateral internal thoracic arterial grafts in patients with left main coronary artery disease undergoing coronary artery bypass grafting: insights from the EXCEL trialdagger. Eur J Cardiothorac Surg 55: 501-10.
- Davierwala PM, Gao C, Thuijs D et al. (2021) Single or multiple arterial bypass graft surgery vs. percutaneous coronary intervention in patients with three-vessel or left main coronary artery disease. Eur Heart J.
- Kelly R, Buth KJ, Legare JF (2012) Bilateral internal thoracic artery grafting is superior to other forms of multiple arterial grafting in providing survival benefit after coronary bypass surgery. J Thorac Cardiovasc Surg 144: 1408-15.
- Takahashi K, Serruys PW, Fuster V et al. (2020) Redevelopment and validation of the SYNTAX score II to individ ualise decision making between percutaneous and surgical revascularisation in patients with complex coronary artery disease: secondary analysis of the multicentre randomised controlled SYNTAXES trial with external cohort validation. Lancet 396: 1399-412.
- Stefanini GG, Holmes DR (2013) Drug-eluting coronary-artery stents. N Engl J Med 368: 254-65
- Byrne RA, Joner M, Kastrati A (2015) Stent thrombosis and restenosis: what have we learned and where are we going? The Andreas Gruntzig Lecture ESC 2014. Eur Heart J 36: 3320-31.
- Taggart DP, D'Amico R, Altman DG (2001) Effect of arterial revascularisation on survival: a systematic review of studies comparing bilateral and single internal mammary arteries. Lancet 358: 870-5.
- Yi G, Shine B, Rehman SM, Altman DG, Taggart DP (2014) Effect of bilateral internal mammary artery grafts on long-term survival: a meta-analysis approach. Circulation 130: 539-45.
- Buttar SN, Yan TD, Taggart DP, Tian DH (2017) Long-term and short-term outcomes of using bilateral internal mammary artery grafting versus left internal mammary artery grafting: a meta-analysis. Heart 103: 1419-26.
- Tam DY, Rocha RV, Fang J et al. (2021) Multiple arterial coronary bypass grafting is associated with greater survival in women. Heart 107: 888-94.
- Taggart DP, Benedetto U, Gerry S et al. (2019) Bilateral versus Single Internal-Thoracic-Artery Grafts at 10 Years. N Engl J Med 380: 437-446.
- Changal K, Masroor S, Elzanaty A et al. (2020) Meta-- Analysis Comparing Multiple Arterial Grafts Versus Single Arterial Graft for Coronary-Artery Bypass Grafting. Am J Cardiol 130: 46-55.
- Takahashi K, Serruys PW, Gao C et al. (2021) TenYear All-Cause Death According to Completeness of Revascularization in Patients With Three-Vessel Disease or Left Main Coronary Artery Disease: Insights From the SYNTAX Extended Survival Study. Circulation 144: 96-109.
- Gaudino M, Kappetein AP, Di Franco A et al. (2020) Randomized Trials in Cardiac Surgery: JACC Review Topic of the Week. J Am Coll Cardiol 75: 1593-604.
- Zolin SJ, Petro CC, Prabhu AS et al. (2020) Registry-Based Randomized Controlled Trials: A New Paradigm for Surgical Research. J Surg Res 255: 428-35.
- Hyun J, Kim JH, Jeong Y et al. (2020) Long-Term Outcomes After PCI or CABG for Left Main Coronary Artery Disease According to Lesion Location. JACC Cardiovasc Interv 13: 2825-36.
FIGURE
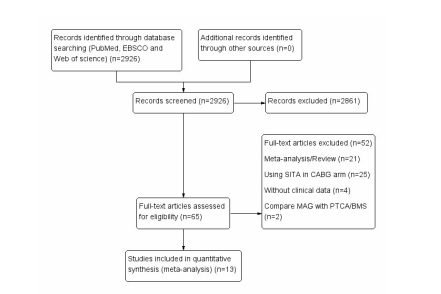
Figure 1: Graphical abstract
FIGURE 1
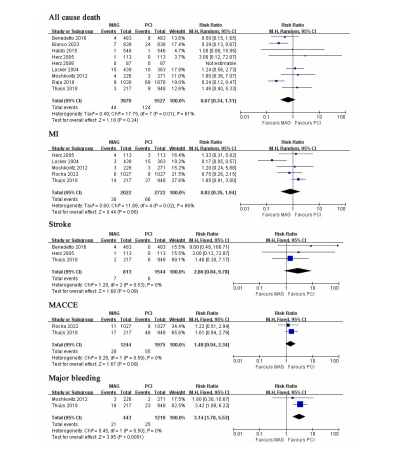
Figure 2: Flowchart of study selection
FIGURE 2
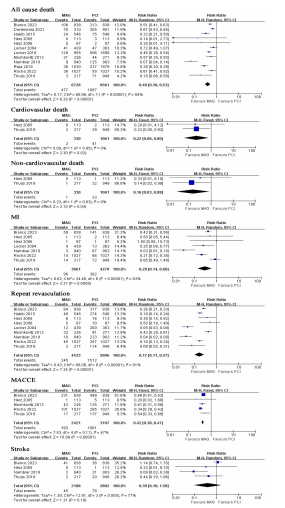
Figure 3: MAG vs. DES-PCI with short-term follow up
Forest plot for short-term incidence of MACCE, all cause death, stroke, MI, repeat revascularization and major bleeding. Risk ratio for individual studies (squares) and meta-analysis (diamonds) and 95% CI (horizontal lines) are presented.
FIGURE 3
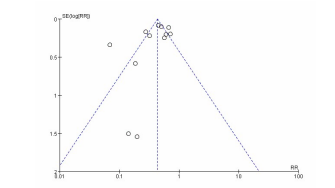
Figure 3: MAG vs. DES-PCI with long-term follow up
Forest plot for long-term incidence of MACCE, all cause death, stroke, MI and repeat revascularization. Risk ratio for individual studies (squares) and meta-analysis (diamonds) and 95% CI (horizontal lines) are presented.
FIGURE 4

Figure 4: The funnel plot for incidence of all cause death with long-term follow up
Tables at a glance
Figures at a glance