Age and Gender Specific Reference Values of Brachial Flow-mediated Dilation and Carotid Intima-media Thickness in CATHAY Study: Atherosclerosis Surrogate Markers in Chinese Adults
Received Date: September 17, 2023 Accepted Date: October 17, 2023 Published Date: October 20, 2023
doi: 10.17303/jcvm.2023.9.103
Citation: Kam Sang Woo, Ping Chook, Yan J Hu, Mei Ki Wong, Yue Hui Yin et al. (2023) Age and Gender Specific Reference Values of Brachial Flow-mediated Dilation and Carotid Intima-media Thickness in CATHAY Study: Atherosclerosis Surrogate Markers in Chinese Adults. J Cardio Vasc Med 9: 1-19
Abstract
Background: Atherosclerotic diseases are currently important health hazard, and surrogate biomarkers (brachial flow-mediated dilation FMD and carotid intima-media thickness IMT) have been advocated for the documentation of early atherogenesis, epidemiological comparison and preventive measures.
Subjects and Methods To establish the reference values of brachial FMD and carotid IMT, we studied 2163 (male 983, female 1180) asymptomatic Han Chinese, aged 20-70 years in Southern and Northern China, and in Overseas Chinese (1996-2007). Fasting glucose, lipid profile (LDL-C, HDL-C, TG), hemoglobin A1-C, folate and vitamin B12 were measured. PM2.5 exposure, brachial FMD and carotid IMT (ultrasound-derived) were evaluated.
Results: The male and female subjects were similar in their mean age, blood glucose, HBA1-C and metabolic status (MS) (p>0.1), but males had higher smoking status, BMI, DBP, LDL-C and TG, and lower HDL-C, folate, vitamin B12 and PM2.5 exposure than the females (p< 0.0002). Brachial FMD (8.43±2.58, 95% CI 8.21-8.65%) was significantly greater, but carotid IMT (0.63±0.13, 95% CI 0.62-0.64) significantly lower in females than in the males (7.55±2.74, 95% CI 7.39-7.78, and 0.67±0.16, 95% CI 0.66-0.68mm respectively) p< 0.0001. The age specific percentile curves confirmed significant impairment of FMD but obvious increase in IMT after 40 years of age, in the males in particular.
On multivariate regression FMD was inversely related to age (beta=-0.166, p< 0.0001), gender (beta=0.152, p< 0.0001) and PM2.5 (beta=-0.486, p=0.005), independent of smoking, and carotid IMT was related to age (beta=0.454, p< 0.0001), gender (beta=0.116, p< 0.0001) and PM2.5 (beta=0.204, p=0.025), independent of BMI, SBP, DBP, LDL-C and MS. In comparison with the French, Italian and Latin American populations, carotid IMT in overall Chinese cohort was significantly lower.
Conclusions The age and gender specific reference values of early atherogenesis, brachial FMD and carotid IMT, in the Chinese were established, and carotid IMT was lower than those in the Caucasian and Latin-American populations
Keywords: Reference Values; Brachial Flow-mediated Dilation; Carotid Intima-media Thickness; Atherosclerotic Surrogates; Native vs Overseas Chinese; Comparative Epidemiology
Introduction
Atherosclerosis is currently a great health hazard, giving rise to heart attacks, stroke and peripheral vascular diseases [1,2]. Pathogenesis of atherosclerosis involves long process for decades of atherogenesis, starting with endothelial dysfunction, in early age, intima-media thickening, plaque formation with or without rupture and ultimately leading to angina, myocardial infarction, heart failure and ischemic stroke [3]. Early preventive measure before the onset of full-blown atherosclerotic diseases is the most important strategy. Advance in ultrasonic imaging has facilitated high resolution vessel-imaging noninvasively, in particular with automatic edge-detection and measurement, and become the gold standard, readily affordable and safe imaging modality. On this issue, two surrogate markers (brachial flow-mediated dilation FMD and carotid intima-media thickness IMT) have been advocated for the documentation of early atherogenesis and evaluation of preventive measures, as well as for comparative epidemiological studies [4-12]. These include the prevention modalities for smoking, hyperlipidemia, hypertension, diabetes mellitus, physical inactivities and air pollution (PM2.5) exposure [13-22].
Reference values of these 2 markers have been reported and derived mostly from the Caucasians [23-31]. with uncertain applicability to other ethnic groups, including Chinese, due to possible inter-ethnic differences. Hence, in the present study, we aimed to establish the reference values of brachial FMD and carotid IMT in Chinese subjects aged 20-70 years, as well as the determinant factors for these 2 markers in Chinese population.
Subjects and Methods
We studied 2670 asymptomatic Han Chinese, aged 20-70 years in Southern China (Hong Kong, Macau, Pan Yu), Northern China (Three Gorges Territories of Yangtze River, Yu County in Shanxi), and Overseas Chinese (San Francisco in USA, and Sydney in Australia) in years 1996-2007, as our multinational collaborative Chinese Atherosclerotic Study in the Aged and Young (CATHAY Study) community project (Figure 1). The project study protocol has been outlined and the preliminary findings of Chinese cohorts reported previously [32-40]. The majority of native Chinese were either born locally, or a minority had migrated to the locations from other Chinese cities for over 20 years, while the overseas Chinese were either born overseas or had migrated and stayed overseas for at least 15 years
All enrolled subjects were apparently healthy, asymptomatic and had no known major cardiovascular, hepatic, thyroid or renal disorders, and were not taking any regular medications or supplementary vitamins. Excluded from the study (n=507) were those discovered after a physical examination and blood test to have cardiovascular, thyroid or renal derrangements. (Figure 1) After fasting for over 12 hours and provision of written informed consent, their cardiovascular profiles were evaluated, including smoking status, body mass index (BMI), waist circumference and waist-hip ratio (WHR), systolic and diastolic blood pressures (SBP and DBP). Fasting blood samples were taken once at recruitment, for lipid profiles (low density lipoprotein cholesterol LDL-C, high density lipoprotein cholesterol HDL-C and triglycerides TG), glucose, hemoglobin A1-C, folate, vitamin B-12 and creatinine. Blood glucose was assessed by hemstix, folate and vitamin B-12 were evaluated by enzymatic immune assays (Abbott X analyses, Abbott Park, Illinous, USA). Blood were assayed in batches at the Prince of Wales Hospital in Hong Kong, the Centro Hospitalas Corde San Januario in Macau, and the Second Hospital of Chongqing Medical University in Chongqing, all currently accredited by USA laboratory centers. The long-term particulate matters < 2.5µm aerodynamic diameter (PM2.5) exposure over China, Sydney and San Francisco Bay Area were evaluated by satellite remote sensing technology, with a root-mean-squared error of 8.9µg/m3 , a correlation coefficient of >0.9 and a mean absolute percentage error within ±20%, against the ground observation [41-43]. Metabolic syndrome (MS) was diagnosed according to the International Diabetes Federation (IDF) criteria [44-45].
Prognostic atherogenesis surrogate markers, brachial FMD and IMT, were studied once at recruitment (2137, 26 defaulted), using high-resolution B-mode ultrasonography as outlined previously [32-40]. In brief, we used a linear array transducer (L10-5) with a medium frequency of 7.5MHz and a standard Advanced Technology Laboratories (ATL 3000, USA) or Sonosite (model Micromaxx, Bothell, USA) system to measure the diameter of the brachial artery. A forearm tourniquet cuff was applied to induce reactive hyperemia upon deflation. The scans were acquired at rest and during reactive hyperemia for flow-mediated endothelium-dependent dilation FMD and after 200µg sublingual glyceryltrinitrate (GTN, an endothelium-independent dilation). FMD and GTN were expressed as percentage dilation of the vessel diameter from the baseline. Hyperemia, as a stress indicator to the endothelium, was calculated as the maximum increase in the blood flow after cuff deflation, compared with the baseline.
Carotid IMT of both carotid arteries were measured, using a standardized scanning protocol as described by Salonen and Salonen, Bots, and Touboul [8,9,11].Images of the far wall of the distal 10 mm of the common carotid artery were acquired. All scans were measured offline by a verified automatic edge-detecting and measurement software package. The intra-observer reproducibility for mean IMT was 0.03±0.01mm, the coefficient of variation was 1% (R=0.99), while the inter-observer variability was optimally maintained (R=0.95).
The project database was processed to derive the mean values, standard deviations and 95% confidence intervals (CI) when appropriate. Standard testing of the normality of distribution was used for assessment of the normal distribution. An independent sample Students’ t-test and an one-way ANCOVA model were used for the evaluation of the intergroup differences. 60 subjects aged >70 years or recognized obviously outliers of FMD or IMT values were excluded from the final analyses. The primary study endpoints were carotid IMT and brachial FMD. The other outcome variables were compared after a Bonferroni adjustment for multiple comparisons [46]. Percentile curves for brachial FMD and carotid IMT were constructed using the LMS standard methods. The LMS method evaluates the measurement centiles in terms of three age – and gender-specific cubic spline curves: the Box-Cox power to transform the normally distributed data (L curve), the median (M curve) and the coefficient of variation (S curve).
(link: https://www.healthforallchildren.com/shopbase/shop/software/lmschartmaker-light/)
Multiple regression analyses were carried out to assess the determinants of the major risk factors for FMD and IMT in the CATHAY subjects respectively, including age, gender, smoking status, BMI, SBP, DBP, LDL-C, MS, PM2.5 and locations (Overseas, Southern or Northern China). The beta effect was evaluated by mixed effect. The variables with significant standard beta coefficients (beta value with 2p< 0.05) as a measure of the contribution to the model were identified, and the insignificant variables (2p>0.05) was subsequently discarded from the regression model. A group difference with an error probability of less than 5% (2p< 0.05) was considered to be statistically significant.
Sample size was calculated in terms of the standard deviation of the 100th centile (c100, alpha=0.05 for 95th percentile) using the sample size planning formula developed by Healy [47]. To obtain an extreme centile, i.e. the 97th centile, with an error of 5.0% and a power of 85%, the estimated sample size of subjects for FMD was 1002 and for IMT 1992 respectively. The statistical analyses were performed with SPSS version 25.
The project complied with the 1995 and 2003 Declaration of Helsinki for human studies. The research study and written informed consent form were approved by our institutional research ethics committee at the Chinese University of Hong Kong and Eastern New Territories of Hong Kong (CREC 2000-108 & CREC 2018-157).
A total of 2163 subjects were enrolled and included, 1180 were female and 983 were male (Table 1). They were similar in their mean age, fasting blood glucose, HBA1-C and metabolic syndrome status. The male subjects had higher smoking status (p < 0.0001), BMI (p< 0.0001), SBP (p=0.047), DBP (p< 0.0001), creatinine (p< 0.0001), LDL-C (p< 0.0001) and TG (p< 0.0001), but lower blood HDL-C (p< 0.0001), folate (p< 0.0001), vitamin B12 (p< 0.0001) and PM2.5 pollution exposure (p< 0.0002), compared with female subjects. 78.1% of females were native Chinese, compared with 74.8% of male subjects (p=0.1).
Vascular ParametersMean diameter of brachial artery in the females (2.98±0.56 mm) was significantly lower than that in the males (3.70±0.61 mm, p=0.0005), while the hyperemia (705.6±257.1% vs 664.9±265.1%) were similar (p=0.07), and GTN slightly greater in the females (18.8±4.2) than in the males (17.6±3.6), p=0.0005. The mean endothelium-dependent dilation FMD were significantly greater in the females (8.43±2.58, 95% CI 8.21-8.65%) than in the males (7.59±2.24, 95% CI 7.39-7.78), p< 0.0001. The mean carotid IMT, however, was significantly lower in the females (0.63±0.13, 95% CI 0.62-0.64 mm) compared with the male subjects (0.67±0.16, 95% CI 0.66-0.68mm), p=0.047.
Reference Values of Brachial FMD and Carotid IMTThe brachial FMD and carotid IMT curves were normally distributed (Figure 2). Mean FMD for the CATHAY cohort was 8.0±2.5%, and mean carotid IMT was 0.65±0.15mm. The gender and age-specific values of brachial FMD and carotid IMT were shown (Figure 3-4). The age and gender specific percentile curves of brachial FMD (Figure 5) and carotid IMT (Figure 6) were displayed. These all showed age-related decrease in brachial FMD and increase in carotid IMT, in particular in the males and age over 40 years.
Determinants of Brachial FMD and Carotid IMTOn multivariate regression analyses, brachial FMD was significantly related to age (beta=-0.166, p< 0.0001), gender (beta=0.152, p< 0.0001) and PM2.5 (beta=-0.486, p=0.005), independent of smoking status or locations (p< 0.03), but not to BMI, SBP, DBP, LDL-C or MS (Table 3). Carotid IMT was significantly related to age (beta=0.454, p< 0.0001), gender (beta=0.116, p< 0.0001) and PM2.5 (beta=0.204, p=0.025), independent of BMI, SBP, DBP, LDL-C and MS, but not to smoking status or locations (Table 4).
For 1 standard deviation (SD) of these significant determinants, brachial FMD decreased by 0.4-0.6% (Figure 7). For 1 SD of age increase (11.7 years), IMT increased by 0.07mm (95% CI 0.06-0.08mm), for 1 SD increase in LDL-C (0.96 mmol/l), IMT increased by 0.01mm (95% CI 0.006-0.019mm), and for 1 SD increase in PM2.5 (26.9 µg/m3), IMT increased by 0.012mm (95% CI 0-0.027mm) (Figure 8).
The normal values of brachial FMD (8.07±2.46, 95% CI7.81-8.30%) and carotid IMT (0.65±0.15, 95% CI 0.64-0.66mm) as prognostic atherosclerosis surrogates in different age and gender groups in the Chinese (n=2163) were established in Northern and Southern China as well as in overseas migrants. These confirmed the findings of our preliminary reports in 410-1656 CATHAY subjects on mean brachial FMD (ranging 7.75-8.15%) and mean carotid IMT (ranging 0.64-0.65mm) [14-15,21-22,32-35,38-40]. The current report included the subjects from all of these preliminary reports. These will be important and mandatory for epidemiological comparison and confirmation of the preventive strategies, both for traditional atherosclerosis risk factors and emerging factors such as PM2.5 air pollution.
FMD was significantly related to age, male gender, smoking and PM2.5 pollution, whereas carotid IMT was related to age, male gender, PM2.5 and traditional risk factors. The gender difference regarding FMD could be mainly attributed to difference in vessel size, apart from their different neurohormonal status [6,48,49]. Age, gender, PM2.5, BMI, SBP and MS were significant determinant factors of carotid IMT, with 0.02-0.06mm difference in carotid IMT for 1 SD of risk factors. To contextualize these differences, a 0.1mm increase in carotid IMT has been associated with a 41% increase in stroke and 43% increase in acute myocardial infarction over a follow-up period of 2-7 years [9]. The 8% difference in carotid IMT was approximately similar to the kind of difference seen between diabetic and non-diabetic Chinese adults [35].
In comparison with the Italian, French and Latin American cohorts [29-31, 50-52], using similar methodologies of ultrasonic scanning and analysis package, carotid IMT in the Chinese is identical to those of Lima cohort, but lower (thinner) than those reported in Italian, Buenos Aires Mexico cities and overall Latin American cohorts (Table 5A&5B). Similarly, for those without risk factor, carotid IMT in the Chinese is lower (thinner) than the French cohort (Table 5C). The mean IMT reported from Santiago is slightly lower than our CATHAY cohort.[30] On the same issue, we have previously reported better preservation of brachial FMD in Chinese than the Australian White on exposure to westernization, aging and smoking [32]. By enlarge, our normal values of these two atherosclerosis surrogate markers concur with our previous epidemiological findings of lower prevalence of atherosclerotic diseases in the Chinese compared with the Western peoples.
Brachial FMD and carotid IMT are both prognostic surrogates of atherogenesis related to long term cardiovascular or stroke outcome. FMD measurement is more dynamic and vulnerable to short term variability in physiological status, mental and physical stress, whereas IMT measurement is comparatively more stable [48-50]. We have previously reported carotid IMT is lower in working farmers than in ex-farmers in the 3-Gorgles Dam Territories. Lifestyle changes in ex-farmers is associated with a worse IMT, compared with those remaining in farming work [39]. In modernizing China, PM2.5 pollution is significantly related to worse IMT and to those with metabolic syndrome in particular, with thinner IMT in Southern Chinese, as compared with Northern Chinese and Overseas Chinese mi-grants [21-22, 38, 53]. Improvement in IMT was demonstrated after folate and vitamin C supplementation in Northern Chinese, and after vitamin B12 correction in the vegetarians in Hong Kong and in Northern Chinese with suboptimal vitamin B12 status, as compared with those with normal B12 status [54]. Similarly adjunctive traditional Chinese medicine treatment in coronary and hypertensive subjects was associated with a significant improvement in FMD and IMT in the randomized placebo-control studies [17,55].
In the present report, two different ultrasonic machine models (ATL3000 or Sonosite) were utilized for brachial and carotid imaging by two investigators (CP and HYJ). The images were measured and analysed blindly throughout, using the same scanning protocol and automatic edge-detecting analysing packages. Accordingly, variations due to technical differences were kept minimized, with good intra-observer reproducibility and inter-observer variability, despite the relatively long period of study (11 years) over 11 sites in mainland China and Overseas.
For a valid FMD measurement, we need an induction of forearm ischemia (by cuff inflation) and subsequent reactive hyperemia (on cuff deflation). Reactive hyperemia can be monitored by measuring the increase in blood flow compared with basal flow. The resulting flow or shear rate-- mediated dilation was measured offline retrospectively, compared with basal brachial diameter. In this regard, the short supply of video-recorder and tape for image storage has recently become a problematic logistic issue. More efficient continuous digital storage onsite for longer period (>2 minutes) in current ultrasonic machines and online measurement of vessel diameters by automatic edge-detecting technology, ought to be developed and popularized for the promotion of FMD measurement in the future. In-service training of ultrasonographer to familiarization of the ultrasonic acquisition and online measurement is equally important and mandatory for the reporting of more accurate and reproducible FMD results. On the other hand, much progress has been made in IMT imaging and analyses in recent years, including instantaneous digital acquisition and storage, automatic edge-detecting facility and measuring packages to facilitate a more user-friendly, practical and highly reproducible IMT measurement.
Limitation of StudyWe acknowledge certain limitations in the present CATHAY Study. Firstly, all subjects recruited were volunteers but not quota samples of specific cities and may not be truely representative of the real general population. Secondly for similar reason, female subjects are believed to be more health-concerned, and therefore we have slightly more females (54.6%) coming up for the study. However, the normal values of FMD and IMT in each gender are still valid for highlighting a gender difference. Thirdly our CATHAY cohort was studied prospectively for demographic factors, ultrasonic imaging and blood tests, although at different time over 11 years, no follow up vascular restudy was planned or arranged. Fourthly only the far wall of both common carotid arteries was measured and registered, which had made the IMT measurement more reproducible and decreased the variability. While the normal values of carotid IMT of both bifurcations may be more significant for reflecting the carotid atherosclerosis progression, their measurement would have increased the standard deviations of our reference values.
The normal values, age and gender distribution of brachial FMD and carotid IMT for Southern, Northern Mainland China and Overseas Chinese migrants were established. These were significantly related to traditional modifiable and non-modifiable atherosclerotic risk factors. Carotid IMT in the Chinese was lower than those in the French, Italian and most Latin American populations. These values should help adding local public health epidemiological information, and improving clinical efforts to reduce cardiovascular risk and diseases in Chinese population, in mainland China and overseas alike.
The research data will be available from the corresponding author to the editor and readers on reasonable request
This work was supported by Star Industrial Company, The Chinese Atherosclerosis Trust, Madam Leung Kit Wah Project Fund, Dr. Stanley Ho Medical Development Foundation (grant & donation) and Dr. Thomas HC Cheung Trust: They provided unrestricted sponsorship for the CATHAY study, without any involvement in study design, data collection, analysis or interpretation, nor in the writing of this report or the decision to submit the paper for publication.
We wish to acknowledge the valuable support of the Chinese Atherosclerosis Trust, Leung Kit Wah Project Fund, Dr. Stanley Ho Medical Development Foundation Trust, the Star Industrial Company Fund of The Chinese University of Hong Kong and Dr. Thomas HC Cheung Trust in sponsoring the study. We also gracefully acknowledge the Macau Heart Foundation, for helping recruitment of subjects, the Pathology Department of Centro Hospitalar Conde de Sao Januario in Macau for the blood assays, the superb statistical analyses and clerical work of Mr. Jason Leung, Dr Enoch So, Dr Kate Chan, and Ms. Daphne Chu, of The Chinese University of Hong Kong.
We declare no financial interests or connections, direct or indirect, or other situations that might raise the question of bias in the work reported or the conclusions, implications or opinions stated - including pertinent commercial or other sources of funding for the individual author(s) or for the associated department(s) or organization(s), personal relationships, or direct academic competition.
Woo KS: Project conception and design, research administration, statistical analysis and interpretation of data, drafting and revision of the article and final approval of the version to be published.
Chook Ping: Project conception and design, performance of ultrasonography analysis and interpretation of data, drafting, revision of the article and final approval of the version to be published.
Hu YJ: Research data collection, performance of ultrasonography analysis and interpretation of data, revision of the article and final approval of the version to be published.
Wong MK: Statistical analyses of database and interpretation of the CATHAY data.
Yin YH: Project conception, interpretation of data, revision of the article and final approval of the version to be published
Li AM: Analyses of data, revision of the paper and final approval of the version to be published.
Chan SW: Project conception and design, research recruitment, administration and interpretation of data, revision of the paper, and final approval of the version to be published.
Kwok CY, Timothy: Design of project, interpretation of data, revision of the article and final approval of the version to be published.
Celemajer DS: Project conception and design, interpretation of data, drafting and revision of the article, and final approval of the version to be published.
All authors agree to be accountable for all aspects of the works.
- Lloyd-Jones D, Adams R, Carnethon M et al. (2009) American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2009 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 119: 480-6.
- Roth GA, Johnson C, Abajobir et al. (2017) Global regional and national burden of cardiovascular diseases for 10 causes, 1990-2015. J Am Coll Cardiol 70: 1-25.
- Ross R (1993) The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature 362: 801-9.
- Celermajer DS, Sorensen K, Gooch V et al. (1992) Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 340: 1111-15.
- Neunteufl T, Heher S, Katzenschlager R, Wölfl G, Kostner K, Maurer G (2000) Late prognostic value of flow-mediated dilation in the brachial artery of patients with chest pain. Am J Cardiol 86: 207-10.
- Herrington DM, Fan L, Drum M, Riley WA, Pusser BE, Crouse JR et al. (2001) Brachial flow-mediated vasodilator responses in population-based research: methods, reproducibility and effects of age, gender and baseline diameter. Eur J Cardio Preve & Rehab 8: 319-28.
- Gokce N, Keaney JF Jr, Hunter LM, Watkins MT, Nedeljkovic ZS, Menzoian JO et al. (2003) Predictive value of noninvasively determined endothelial dysfunction for longterm cardiovascular events in patients with peripheral vascular disease. J Am Coll Cardiol 41: 1769-75.
- Salonen JT, Salonen R (1991) Ultrasonographically assessed carotid morphology and the risk of coronary heart disease. Arterioscler Thromb Vasc Biol 11: 1245-9.
- Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE (1997) Common carotid intima-media thickness and risk of stroke and myocardial infarction: The Rotterdam Study. Circulation 96: 1432-7.
- O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson Jr SK (1999) Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. N Engl J Med 340: 14-22.
- Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P et al. (2004) Advisory Board of the 3rd Watching the Risk Symposium 2004, 13th European Stroke Conference. Mannheim intima-media thickness consensus. Cerebrovasc Dis18: 346-9.
- Lorenz MW, Markus HS, Bots ML et al. (2007) Prediction of clinical cardiovascular eventswithcarotidintima-media thickness:Asystematicreviewandmeta-analysis.Circulation115: 457-67.
- DS Celermajer, MR Adams, P Clarkson et al. (1996) Passive smoking and impaired endothelium-dependent arterial dilatation in healthy young adults. N Engl J Med 1996; 334:150-4
- Woo KS, Chook P, Leung HC, Huang XS, Celermajer DS (2000) The Impact of Heavy Passive Smoking on Arterial Endothelial Function in Modernized Chinese. J Am College Cardiol 36: 1228-32.
- Thomas GN, Chook P, Yip TWC, Kwong SK, Chan TYK et al. (2008) Smoking without exception adversely affects vascular structure and function in apparently healthy Chinese: Implications in global atherosclerosis prevention. Int J Cardiol128: 172-7.
- Woo KS, Yip Thomas WC, Chook P, Koon KV, Leong HC, Feng XH et al. (2021) Vitamins B-12 and C Supplementation Improves Arterial Reactivity and Structure in Passive Smokers: Implication in Prevention of Smoking-Related Atherosclerosis. J Nutr Health Aging 25: 248-54.
- Woo KS, Yip Thomas WC, Chook P, Kwong SK, Szeto CC et al. (2013) Cardiovascular Protective Effects of Adjunctive Alternative Medicine (Salvia miltiorrhiza and Pueraria lobata) in High-Risk Hypertension. Evid Based Comple Alternat Med 2013: 132912.
- Kajikawa M, Maruhashi T, Hida E, Iwamoto Y, Matsumoto T et al. (2016) Combination of Flow-Mediated Vasodilation and Nitroglycerine-Induced Vasodilation Is More Effective for Prediction of Cardiovascular Events. Hypertension 67: 1045-52.
- Gallo G, Volpe M, Savoia C (2021) Endothelial dysfunction in hypertension: current concepts and clinical implications. Front Med 8: 798958.
- Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P et al. (2007) Mannheim carotid intima-media thickness consensus (2004–2006): an update on behalf of the Advisory Board of the 3rd and 4th Watching the Risk Symposium, 13th and 15th European Stroke Conferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006. Cerebrovasc Dis 23: 75-80.
- Woo KS, Lin CQ, Yin YH, Guo DS, Chook P, Kwok CY Timothy et al. (2021) The Impact of Air Pollution (PM2.5) on Atherogenesis in Modernizing Southern versus Northern China. Atmosphere12: 1552.
- Woo KS, Chook P, Hu YJ, et al. (2021) The Impact of Particulate Matter Air Pollution (PM2.5) on Atherosclerosis in Modernizing China: the report from CATHAY Study. Inte J Epid 50: 578-88.
- Bonithon-Kopp C, Scarabin PY, Taquet A et al. (1991) Risk factors for early carotid atherosclerosis in middle-aged French women. Arterioscler Thromb Vasc Biol 11: 966-72.
- Prati P, Vanuzzo D, Casaroli M et al. (1992) Prevalence and determinants of carotid atherosclerosis in a general population. Stroke 23: 1705-11.
- Salonen R, Tervahauta M, Salonen JT et al. (1994) Ultrasonographic manifestations of common carotid atherosclerosis in elderly eastern Finnish men. Prevalence and associations with cardiovascular diseases and risk factors. Arterioscler Thromb Vasc Biol 14: 1631-40.
- Mannami T, Konishi M, Baba S et al. (1997) Prevalence of asymptomatic carotid atherosclerotic lesions detected by high-resolution ultrasonography and its relation to cardiovascular risk factors in the general population of a Japanese city: the Suita study. Stroke 28: 518-25.
- Sonecha TN, Henein MY (2005) The role of intimamedial thickness (IMT) in clinical cardiovascular practice. Int J Cardiovasc Image 21: 505-7
- Touboul PJ, Vicaut E, Labreuche J et al. (2005) Design, baseline characteristics and carotid intima-media thickness reproducibility in the PARC study. Cerebrovasc Dis19: 57-63.
- Touboul PJ, Hernández-Hernández R, Serdar K, Woo KS, Vicaut E et al. (2007) for the PARC-AALA Investigators. Carotid artery intima media thickness, plaque and framingham cardiovascular score in Asia, Africa/Middle East and Latin America: the PARC-AALA Study. Int J Cardiovasc Imaging 23: 557-67.
- Schargrodsky H, Hernández-Hernández R, Champagne BM, et al. (2008) CARMELA: assessment of cardiovascular risk in seven Latin American cities. Am J Med121: 58-65.
- Touboul PJ, Labreuche J, Vicaut E, Belliard PJ, Cohen S et al. (2009) on behalf of the PARC Study Investigators. Country-Based Reference Values and Impact of Cardiovascular Risk Factors on Carotid Intima-Media Thickness in a French Population: The ‘Paroi Artérielle et Risque Cardio-- Vasculaire’ (PARC) Study. Cerebrovasc Dis 27: 361-7.
- Woo KS, Robinson JT, Chook P, et al. (1997) Differences in the effect of cigarette smoking on endothelial function in Chinese and white adults. Ann Intern Med 127: 372-5.
- Woo KS, McCrohon JA, Chook P, et al. (1997) Chinese Adults Are Less Susceptible Than Whites to Age-Related Endothelial Dysfunction. J Am Coll Cardiol 30: 113-8.
- Woo KS, Chook P, Raitakari OT, McQuillan B, Feng JZ, Celermajer DS (1999) Westernization of Chinese adults and increased subclinical atherosclerosis. Arterioscler Thromb Vasc Biol19: 2487-93.
- Thomas GN, Chook P, Qiao M et al. (2004) Deleterious impact of “high normal” glucose levels and other metabolic syndrome components on arterial endothelial function and intima-media thickness in apparently healthy Chinese subject: The CATHAY study. Arterioscler Thromb Vasc Biol 24: 739-43.
- Woo KS, Chook P, Yu CW, Sung RY et al. (2004) Overweight in children is associated with arterial endothelial dysfunction and intima-media thickening. Int J Obes 28: 852-57.
- Woo KS, Chook P, Yu CW et al. (2004) Effects of diet and exercise on obesity-related vascular dysfunction in children. Circulation109: 1981-86.
- Woo KS, Chan SW, Kwok Timothy CY, Yin YH, Chook P, Lin CQ, Celermajer DS (2022) The Different Impact of PM2.5 on Atherogenesis in Overseas vs Native Chinese in the CATHAY Study. Atmosphere 13: 1236.
- Woo KS, Hu YJ, Chook P, et al. (2020) The Impact of Lifestyle Changes on Cardiometabolic Health in Modernizing China: A Tale of Three Gorges in the Yangtze River. Metab Syndr Relat Disord 18: 65-71.
- Kwok CYT, Poon YKP, Chook P, Guo DS, Lin CQ, Yin YH et al. (2023) A Potential Strategy for Atherosclerosis Prevention in Modernizing China - Hyperhomocysteinemia, MTHFR C677T Polymorphism and Air Pollution (PM2.5) on Atherogenesis in Chinese Adults. J Nutr Health Aging 27: 134-41.
- Lin CQ, Li Y, Yuan ZB, Lau AKH, Li, CC, and Fung JCH (2015) Using satellite remote sensing data to estimate the high-resolution distribution of ground-level PM2.5. Remote Sens Environ156: 117-28.
- Lin CQ, Liu G, Lau AKH, Li Y, Li CC, Fung JCH, and Lao XQ (2018) High-resolution satellite remote sensing of provincial PM2.5 trends in China from 2001 to 2015. Atmos Environ180: 110-6.
- Li C, Lau AKH, Mao J, and Chu DA (2005) Retrieval, validation, and application of the 1-km aerosol optical depth from MODIS measurements over Hong Kong. IEEE Trans. Geosci. Remote Sens 43: 2650-8.
- Zimmet P, Alberti K, George MM and Rios MS (2005) A new International Diabetes Federation (IDF) worldwide definition of the metabolic syndrome: The rationale and the results. Rev Esp Cardiol 58: 1371-6.
- Woo KS, Hu YJ, Chook P, et al. (2019) A Tale of Three Gorges in the Yangtze River: Comparing the Prevalence of Metabolic Syndrome According to ATP III, WHO, and IDF Criteria and the Association with Vascular Health in Modernizing China. Meta Syndr Relat Disord 17: 137-42
- Hochberg Y (1988) A sharper Bonferroni procedure for multiple tests of significance. Biometrika 75: 800-2.
- Healy M (1978) Statistics of growth standards. Principles and Prenatal Growth. New York: Spring US 1978: 169-81.
- Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F et al. (2002) International Brachial Artery Reactivity Task Force. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol 39: 257-65.
- Deanfield John E., Halcox Julian P. and Rabelink Ton J (2007) Endothelial Function and Dysfunction Testing and Clinical Relevance. Circulation 115: 1285-95.
- Thijssen DHJ, Bruno RM, van Mil ACCM, Holder SM, Faita F et al. (2019) Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur Heart J 40: 2534-47.
- Touboul PJ, Labreuche J, Bruckert E, Schargrodsky H, Prati P et al. (2014) HDL-C, triglycerides and carotid IMT: a meta-analysis of 21,000 patients with automated edge detection IMT measurement. Atherosclerosis 232: 65-71.
- Tosetto A, Prati P, Baracchini C, Manara R, Rodeghiero F (2005) Age-adjusted reference limits for carotid intima-media thickness as better indicator of vascular risk: population-based estimates from the VITA project. J Thromb Haemost 3: 1224-30.
- Woo KS, Timothy KCY, Chook P, Hu YJ, Yin YH et al. (2021) Independent Effects of Metabolic Syndrome and Air Pollution (PM2.5) on Atherosclerosis in Modernizing China. Austin J Public Health Epidemiol 8: 1097.
- Woo KS, Kwok Timothy CY, Celermajer DS (2004) Vegan Diet, Subnormal Vitamin B-12 Status and Cardiovascular Health. Nutrients 6: 3259-73.
- Tam Wing Y, Chook P, Qiao M, Chan Lin T, Chan Thomas YK et al. (2009) The efficacy and tolerability of adjunctive alternative herbal medicine (Salvia miltiorrhiza and Pueraria lobata) on vascular function and structure in coronary patients. J Altern Complement Med 15: 415-21.
FIGURE 1
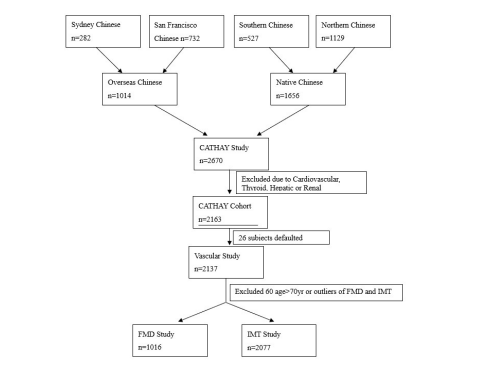
Figure 1: Schematic Diagram of Enrollment in CATHAY Study, Recruiting 2163 Native and Overseas Chinese adults
FIGURE 2
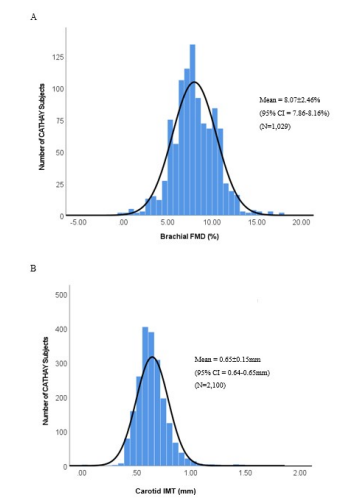
Figure 2: Normal distribution of (A) brachial flow-mediated dilation (FMD) and (B) carotid intima-media thickness (IMT) in CATHAY Cohort
FIGURE 3
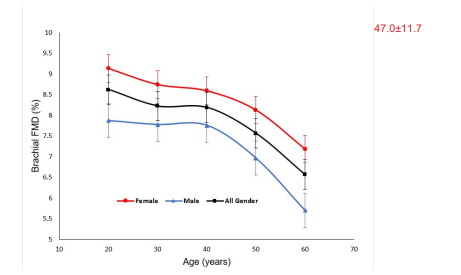
Figure 3: Gender-specific brachial flow-mediated dilation (FMD) in CATHAY subjects according to age, with display of the mean and standard deviation (%) in each age group.
FIGURE 4
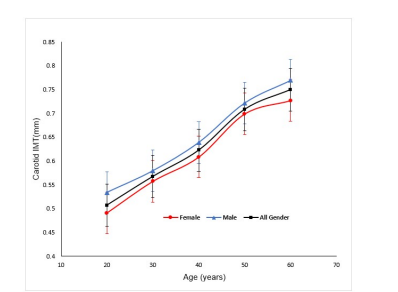
Figure 4: Gender-specific carotid intima-media thickness (IMT) in CATHAY subjects according to age, with display of the mean and standard deviation (mm) in each age group.
FIGURE 5
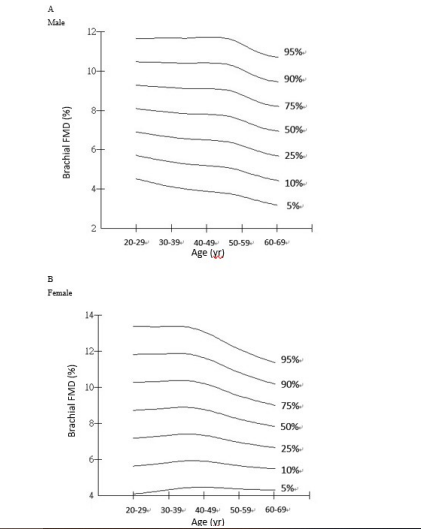
Figure 5: Smoothed brachial flow-mediated dilation (FMD) in centiles 5%-95%) of CATHAY subjects according to age in the males (A) and the females (B).
FIGURE 6
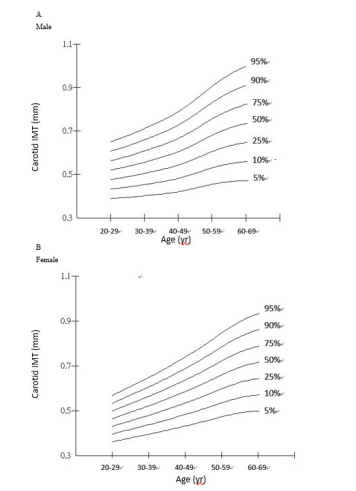
Figure 6: Smoothed carotid IMT in centiles in CATHAY subjects in centiles 5%-95%) of CATHAY subjects according to age in the males (A) and the females (B).
FIGURE 7
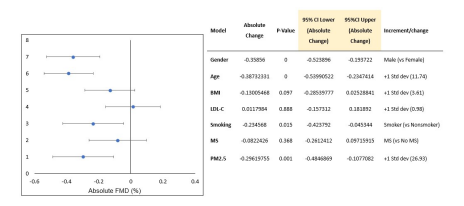
Figure 7: Forest Plot of Brachial Flow-mediated Dilation (FMD) in CATHAY Subjects
FIGURE 8
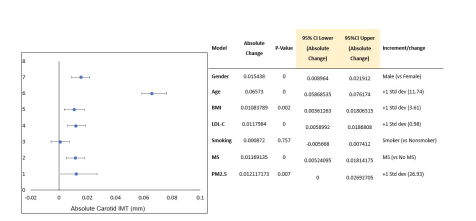
Figure 8: Forest Plot of Carotid Intima-media Thickness (IMT) in CATHAY Subjects
Tables at a glance
Figures at a glance