Stenotic Ileal Crohn Associated with a Chronic Large Ileosigmoidal Fistula
Received Date: September 08, 2024 Accepted Date: October 08, 2024 Published Date: October 11, 2024
doi: 10.17303/jddh.2024.2.101
Citation: Zeinab El Zein, Alain Njeim, Mayssam Meouche, Peter Raffoul, Elie Mokled, et al. (2024) Stenotic Ileal Crohn Associated with a Chronic Large Ileosigmoidal Fistula. J Digestive Disord Hepatol 1: 1-9
Abstract
Ileocolic fistulas and strictures of the small bowel are serious complications of Crohn’s disease and may greatly influence the course of the disease and affect the patient’s quality of life. We report a case of a 37-year-old man who presented, within 1 year of his Crohn’s disease diagnosis, with a 1-day history of severe abdominal pain and obstipation. His previous bowel movements were normal and he denied experiencing diarrhea or constipation before presentation. The patient was found to have a small bowel obstruction after imaging. Dilated small bowel loops and a transitional zone were observed on CT. Moreover, the patient reported to have been on Adalimumab and steroids since the time of diagnosis. He was operated on emergently and was found to have a stricture measuring about 8cm in length with a large ileosigmoidal fistula at the site of stricture. His small bowel proximal to the stricture and fistula was noted to have a large diameter of 10cm with a leather-like texture. Fistulectomy was done with enterectomy of the stenosed segment and bowel continuity was not established. Instead, a loop ileostomy was extracted. Post-operatively, the patient was transferred to the floor where he received low doses of steroids, to avoid adrenal insufficiency, and broad-spectrum antibiotics in addition to total parenteral nutrition. He was discharged home on the fifth post-operative day in good condition with further follow-up in the clinic.
Keywords: Crohn’s Disease; Ileocolic Fistula; Small Bowel Obstruction; Stricture; Enterectomy; Loop Ileostomy
Introduction
Crohn’s disease (CD), a type of inflammatory bowel disease whose cause is not yet entirely clear, is a chronic disease affecting the GI tract and may involve any part of it [1]. Its incidence has been increasing globally [2]. Gastrointestinal symptoms, such as pain and diarrhea, may be the main presenting symptoms [1]. Moreover, extraintestinal manifestations such as scleritis and pyoderma gangrenosum may also be observed. Complications of CD may occur in about half of all patients within 20 years of their diagnosis and may involve fistulas, abscesses, strictures, and even malignancies [1,3]. CD seems to cause more fistulas and strictures when occurring in the proximal gastrointestinal tract, ileum or ileocolic segments [3]. Management of such complications may often be complex and require a multidisciplinary approach [4]. Clinical suspicion of ileocolic fistulas should remain high in the setting of strictures caused by CD even when patients are not complaining of fistula related symptoms.
Case Presentation
A 37-year-old male, who has been diagnosed with CD for 1 year, presented to the emergency department with a one-day history of diffuse abdominal pain and obstipation. The patient has been initially receiving Adalimumab as his treatment, which did not improve his overall clinical condition, before changing his gastroenterologist. His new gastroenterologist started him on Infliximab and a daily Prednisone dosage of 50mg by mouth. At presentation he reported the pain to have been diffuse and relentless similar to previous episodes but more severe and associated with bloating and obstipation. On physical exam he was ill-looking, cachectic with dull-sunken eyes. His abdomen was soft but distended, tympanic, and diffusely tender with involuntary guarding. His vital signs were stable. The patient’s blood work on admission revealed marked leukocytosis with a left shift, normal liver enzymes and an increased c-reactive protein. The patient was resuscitated with colloids and was started on wide spectrum antibiotics. Surgical consult was obtained next.
A CT scan of the abdomen and pelvis with intravenous contrast was done and revealed the presence of multiple dilated small bowel loops, with a diameter reaching about 8cm, multiple air fluid levels, fluid in the Douglas pouch and a clear transitional zone in the distal ileum before the ileocecal valve (Figure 1). Given his clinical condition and imaging findings, the surgery team decided to operate on the patient. Therefore, a laparotomy was performed.During the surgery, fluid was encountered in the pelvic region which was aspirated and sent for culture studies. Intraoperative findings revealed remarkable small bowel distension reaching up to 10cm in diameter (Figure 2). The distension extended along the entire length of the ileum. A very large ileosigmoidal fistula measuring 5cm in length and 0.5cm in diameter was detected along the distended small bowel 15 cm from the ileocecal valve. A stricture measuring about 8cm in length, representing the transitional zone seen on imaging, existed 5 cm proximal to the ileocecal valve. The fistula was emerging from the stenosed bowel segment.
The sigmoid colon was slightly hyperemic but did not appear sick and no gross involvement with CD was observed. Thus, a fistulectomy was started by stapling the end of the ileosigmoidal fistula at the sigmoid colon using a purple 60mm GIA stapler without resecting the involved sigmoid (Figure 3). An enterectomy of the stenosed segment that included the fistula was performed using a 60mm purple GIA stapler about 3cm proximal to the ileocecal valve and no bowel continuity between the ileum and colon was established (Figures 4,5). A loop ileostomy was then extracted due to an inability to extract an end ileostomy given its very large diameter. This decision was taken given the intraabdominal condition of the bowels and colon and in order to avoid possible complications of a primary anastomosis. A hemovac drain was inserted and kept in the Douglas pouch. Finally, the abdomen was closed layer by layer in the respective manner in which it was opened.
Post-operatively, he was transferred to the floor where he received wide-spectrum antibiotics and total parenteral nutrition. During his hospital stay, an infectious diseases specialist consult was obtained for adjustment of the antibiotics he was taking after his intra-operative fluid culture was positive for E. coli ESBL. His clinical condition improved and was started on enteral feeding on the second post-operative day. He was then discharged on the fifth post-operative day, after removal of the drain and ensuring resolution of his leukocytosis, with a plan for establishing bowel continuity once he becomes in the remission phase of his disease. Furthermore, his pathology studies of the resected small bowel showed no malignancy and only chronic inflammatory changes including ulceration and fistulization which are compatible with his CD. Disease remission is measured by improvement of his symptomatology. His quality of life, post-operatively, is expected to improve after resection of the diseased bowel segment and resolution of his antibiotic Restoration of bowel continuity is also planned to take place 8 weeks after primary surgery if approval is given by his gastroenterologist.
Discussion
CD can be classified as an incurable condition that surgical treatment, despite not being definitive, is primarily used to manage its complications, including fistulization, which signals a more aggressive course [5]. Ileosigmoid fistulas (ISF) account for 5% of CD cases and 20% of fistulizing abdominal CD [6,7]. Clinical features typically associated with ISF at diagnosis include increased diarrhea, weight loss, crampy abdominal pain, and fever [8]. However, our patient presented unusually, with regular stool patterns and normal consistency until one day before the presentation.
Despite being treated with anti-TNF alpha for a year, which is effective in managing steroid-resistant or immunomodulator-refractory CD, especially fistulizing disease, our patient developed a fistula within a year of diagnosis, as revealed intraoperatively. An uncommonness worth the mention, as clinical benefits of anti-TNF therapy typically manifest within two weeks of initiation [9].
Often, ISFs are unexpected intraoperative findings that can significantly alter the surgical plan. In fact, up to two-third of ISFs go undetected until surgical exploration [10]. In our patient's case, the ISF was missed on the CT scan, which is consistent with reports that CT scans detect only about 40% of ISFs. Moreover, this percentage increases to 77% when the imaging is performed with po contrast [22]. However, contrast studies are usually avoided in the emergent setting.
The literature contains only a few case series discussing the outcomes of surgical treatment for ISF, and current guidelines provide no definitive recommendations, leaving the surgical approach to the discretion of the operating surgeon. The fate of the sigmoid colon is a key concern in surgical decision-making [11]. ISF management has always involved either ileocecal resection or right hemicolectomy alongside addressing the fistula. Key considerations include whether to perform a sigmoid resection or primary repair of the fistula defect. Segmental resection is indicated when the sigmoid is affected, has a significant defect, a defect on the mesenteric side, or shows abscess formation [10,12,13]. Otherwise, primary repair, such as excision or wedge resection of the fistula with simple suturing, is the indicated approach [11]. A case series of 69 case reports published in 2020 reported that 42% underwent sigmoidal resection as part of the ISF management due to the involvement of the sigmoid with CD [21]. In our patient’s case, the sigmoid appeared hyperemic but was deemed disease-free intraoperatively and the defect was not on the mesenteric side. Thus, a simple excision of the fistulous tract with sparing of the sigmoid colon was done to avoid extensive and unnecessary resection of a bowel or colonic segment.
Another critical decision is whether to create a stoma or not. Current practice recommends a tailored approach. A stoma is recommended when at least one risk factor is present, including intra-abdominal abscess, steroids > 20 mg/day, low albumin level, the need for additional surgical intervention beyond ileocecal resection, severe perianal disease, biological therapy, and prior surgical failure. However, when it comes to the stoma type, there is no definitive recommendation, as various types have been reported in the literature, including synchronous ileo- and ascendo-/- transverse colostomy, loop colostomy, terminal colostomy after Hartmann's procedure, and protective loop ileostomy [11]. In patients with CD, like ours, diverting ileostomy is often preferred over primary anastomosis, especially when multiple risk factors for an anastomotic leak, such as prolonged steroid use and biological therapy, and weight loss, are present [14]. A loop ileostomy was performed due to the inability to create an end ileostomy, given the large diameter of the ileum.
A stricture is another complication of CD that represents an abnormal narrowing of the involved bowel segment and may result in partial or total occlusion of the gastrointestinal tract. It is a relatively common complication that eventually requires surgical resection [15]. Strictures may be acute or chronic. Acute strictures are associated with bowel wall edema whereas chronic strictures tend to have a fibrotic nature. It is reported that about 71% of patients required one surgical intervention for abdominal complications of CD within 10 years of their diagnosis and over half of the surgeries performed were in the setting of an obstruction due to strictures [1,15]. The data published has led to the conclusion that the most common complication of small bowel CD is obstruction [16]. Strictures are more common when ileal involvement is present and when CD is diagnosed at a younger age [17].
Surgical intervention in the case of strictures is more likely to be done when an associated complete obstruction, an enterocolic fistula, a stricture measuring at least 5mm in length, an abscess, or a proximal dilated small bowel of more than 3 cm exists [14]. Our patient was young with ileal CD and had an ileosigmoidal fistula emerging from the stricture measuring 5cm in length and associated with a 10 cm diameter of the proximal bowel. Thus, he had all the factors associated with a stricture that placed him at an increased risk for surgical intervention.
If a patient with CD presents to the emergency department with a picture of an acute abdomen, an abscess, and a free perforation must be ruled out. When both are ruled out and the patient is found to be clinically stable, medical therapy may be first initiated even in the setting of an obstruction [18]. However, when the patient is unresponsive to medical treatment, surgical intervention must be carried out and these patients represent up to 66% of patients with CD complicated by a stricture [18]. Our patient has been on steroids for about 2 months and has changed his immunomodulation therapy to no avail. Hence, requiring surgical intervention.
Strictures may also represent malignant lesions and not just fibrotic changes that have occurred with time. Malignant strictures are more common when occurring in the large bowel compared to the small bowel [15]. 6.8% of colonic strictures are found to be malignant, whereas, malignant small bowel strictures are relatively rare and represent less than one percent [19]. Thus, the global consensus is that the strictured segment should be resected [15].
Management of strictures may be endoscopic or surgical. Some endoscopist specialists employ the usage of balloon dilation or “stricturotomy” for fibrotic strictures with success rates reaching 92% [18]. Strictures that are believed to be ideal for balloon dilatation are those that are accessible by an endoscope, measure less than 5cm in length, and are theoretically straight. The two best benefits of endoscopic balloon dilation include the minimally invasive approach and preservation of bowel length by avoiding resection of the bowel [18]. However, the procedure includes complications such as perforation, bleeding, and dilation-related need for surgery occurring in about 2.8% of cases. Moreover, a follow-up period of 36 months revealed that 47.5% of patients had a symptomatic recurrence and 28.6% went on to need surgical intervention [18].
Surgical intervention was traditionally the treatment of choice for the treatment of strictures [15,18]. Laparoscopic approach has been gaining popularity but lesser so in the setting of recurrent or complicated cases. A wide range of conversion, to open, rate was reported to be between 6.7 to 42.3% [20]. When the involved segment is significant in length, short bowel syndrome may occur if resected and thus, stricturoplasty should be considered instead if possible [18]. Complication rates in the short and long periods in patients who underwent stricturoplasty alone, resection with anastomosis alone, or both were reported to be similar by Landerholm and colleagues [20].
Conclusion
With the global increasing incidence of CD and increasing mortality it has become important for healthcare practitioners to thoroughly understand the multiple complications that may occur and how to manage them. A multidisciplinary approach with specialists should be adapted in all these patients and especially when presenting to the emergency department with complications. Appropriate medical therapy should be based on the patient’s disease severity. Surgical consult should always be obtained and surgical intervention should be carried out in patients with complications such as strictures causing small bowel obstruction, fistulizing disease, abscesses, free perforation or suspicion of malignancy. It may also be better to perform a resection with a diverting ileostomy rather than a primary anastomosis or stricturoplasty when operating on a Crohn’s patient in an acute setting and particularly with an involvement of the ileum or ileocecum.
Consent
This study was approved by the ethics committee of the hospital, IRB approval was obtained and consent was given from the patient for publication.
Competing of Interest
The authors declare that they have no conflicts of interest concerning the publication of this paper.
Funding Sources
The authors haven’t received any funding
Author Contributions
Antoine Kachi and Antoine Geagea followed up the patient and cared clinically for him. Antoine Kachi operated on the patient, organized the photos and reviewed the article. Zeinab El Zein and Alain Njeim wrote the manuscript. Maysaam Meouche, Elie Mokled and Peter Raffoul helped obtain the IRB approval and reviewed the article.
- Ranasinghe IR, Tian C, Hsu R. Crohn Disease (2024). In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024
- Zhou JL, Bao JC, Liao XY et al. (2023) Trends and projections of inflammatory bowel disease at the global, regional and national levels, 1990–2050: a bayesian age-period-cohort modeling study. BMC Public Health 23: 2507.
- Thia KT, Sandborn WJ, Harmsen WS, Zinsmeister AR, Loftus EV (2010) Risk factors associated with progression to intestinal complications of Crohn's disease in a population-based cohort. Gastroenterology. 139: 1147-55.
- Luglio G, Cassese G, Amendola A, Rispo A, Maione F, De Palma GD (2018) Novel Approaches to Ileocolic and Perianal Fistulising Crohn's Disease. Gastroenterol Res Pract. 2018: 3159543.
- Windsor AC (2002) Ileal Crohn's disease is best treated by surgery. Gut. 51: 11-2.
- Yoon YS, Yu CS, Yang SK, Yoon SN, Lim SB, Kim JC (2010) Intra-abdominal fistulas in surgically treated Crohn's disease patients. World J Surg. 34: 1924-9.
- Saint-Marc O, Vaillant JC, Frileux P, Balladur P, Tiret E, Parc R (1995) Surgical management of ileosigmoid fistulas in Crohn's disease: role of preoperative colonoscopy. Dis Colon Rectum. 38: 1084-7.
- Broe PJ, Cameron JL (1982) Surgical management of ileosigmoid fistulas in Crohn's disease. Am J Surg. 143: 611-3.
- Kawalec P, Mikrut A, Wiśniewska N, Pilc A (2013) Tumor necrosis factor-α antibodies (infliximab, adalimumab and certolizumab) in Crohn's disease: systematic review and meta-analysis. Arch Med Sci. 9: 765-79.
- Young-Fadok TM, Wolff BG, Meagher A, Benn PL, Dozois RR (1997) Surgical management of ileosigmoid fistulas in Crohn's disease. Dis Colon Rectum. 40: 558-61.
- Popivanov G, Stoyanova D, Konaktchieva M, Cirocchi R, Penchev D, Kjossev K, Tonchev P, Mutafchiyski V (2020) Crohn's Disease Complicated by Ileosigmoid Fistula - Synchronous Resection or Primary Sigmoid Repair, One or Two-stage Procedure? A systematic review of the literature and prospective case series. Folia Med (Plovdiv). 62: 703-11.
- Heimann T, Greenstein AJ, Aufses AH Jr (1979) Surgical management of ileosigmoid fistula in Crohn's disease. Am J Gastroenterol. 72: 21-4.
- Michelassi F, Stella M, Balestracci T, Giuliante F, Marogna P, Block GE (1993) Incidence, diagnosis, and treatment of enteric and colorectal fistulae in patients with Crohn's disease. Ann Surg. 218: 660-6.
- Lightner AL, Vogel JD, Carmichael JC, Keller DS, Shah SA, et al. (2020) The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Surgical Management of Crohn's Disease. Dis Colon Rectum. 63: 1028-52.
- Bernell O, Lapidus A, Hellers G (2000) Risk factors for surgery and postoperative recurrence in Crohn's disease. Ann Surg. 231: 38-45.
- Toh JW, Stewart P, Rickard M J, Leong R, Wang N, Young CJ (2016) Indications and surgical options for small bowel, large bowel and perianal Crohn's disease. World J Gastroenterol. 22: 8892-904.
- Goldstone RN, Steinhagen RM (2019) Abdominal emergencies in inflammatory bowel disease. Surg Clin North Am. 99: 1141-50.
- Ford MM (2021) Crohn's Disease Obstructions. Clin Colon Rectal Surg. 34: 227-32.
- Campbell L, Ambe R, Weaver J, Marcus S M, Cagir B (2012) Comparison of conventional and nonconventional strictureplasties in Crohn's disease: a systematic review and meta-analysis. Dis Colon Rectum. 55: 714-26.
- Landerholm K, Reali C, Mortensen NJ, Travis S PL, Guy RJ, George BD (2020) Short- and long-term outcomes of strictureplasty for obstructive Crohn's disease. Colorectal Dis. 22: 1159-68.
- Popivanov G, Stoyanova D, Konaktchieva M, Cirocchi R, Penchev D, et al. (2020) Crohn's Disease Complicated by Ileosigmoid Fistula - Synchronous Resection or Primary Sigmoid Repair, One or Two-stage Procedure? A syste- matic review of the literature and prospective case series. Folia Med (Plovdiv). 62: 703-11.
FIGURE 1

Figure 1: Cross-sectional view of the CT abdomen and pelvis shows multiple dilated small bowel loop, with air fluid levels, a stenotic segment representing the transitional zone (red arrow) and fluid in the abdomen (yellow arrow)
FIGURE 2
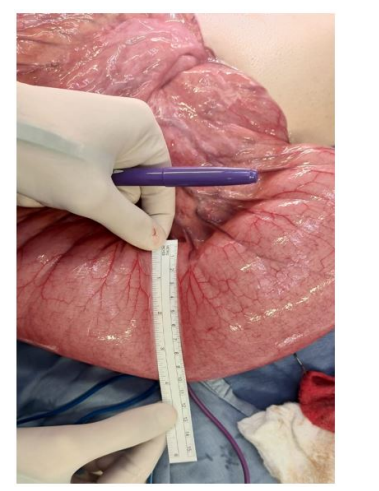
Figure 2: Intraoperative findings: remarkable small bowel distension reaching up to 10cm in diameter
FIGURE 3
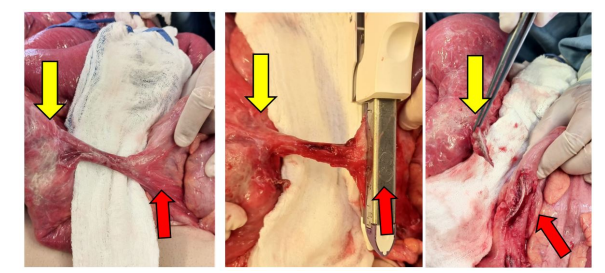
Figure 3: Intraoperative findings: fistulectomy at the sigmoidal end. Red arrow represents the sigmoidal end of the fistula and yellow arrow represents the ileal end
FIGURE 4
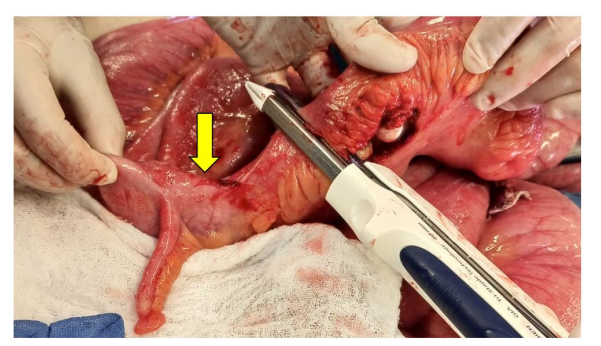
Figure 4: Intraoperative findings: enterectomy 3cm proximal to the ileocecal valve (yellow arrow)
FIGURE 5
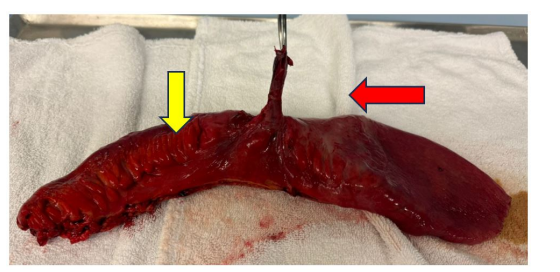
Figure 5: The resected ileal sigmoid which includes the stenosed ileum (yellow arrow) and fistula (red arrow)
Figures at a glance