Improving Sleep Quality Through Biomechanical Stimulation of Oral Musculature and Mucosa
Received Date: April 25, 2023 Accepted Date: May 25, 2023 Published Date: May 29, 2023
doi: 10.17303/jdoh.2023.10.103
Citation: T Telschow, R Stark, F Dudde, KO Henkel (2023) Improving Sleep Quality Through Biomechanical Stimulation of Oral Musculature and Mucosa. J Dent Oral Health 10: 1-7
Introduction
Sleep is an indispensable phase of rest and relaxation for humans. Disturbed sleep leads to an interruption of physiological reparative mechanisms in the human organism with the consequence of increased occurrence of diseases [1]. Primary snoring leads to disturbed sleep architecture. In particular, the number and length of deep sleep phases (REM sleep) are reduced. For example, Matthew et al. (2017) [2] demonstrated that 1% less REM sleep leads to a 9% higher risk of developing dementia. One explanation for this can be seen in the disruption of the glial lymphatic system. This system is controlled by glial cells and serves to remove harmful substances from the brain. In the awake state, the space between the glial cells is reduced, due to cell shrinkage during sleep. Thus, the outflow of harmful substances is increased during sleep.
In this study it is investigated whether it is possible to alleviate primary snoring and to achieve physiological vital parameters by a biomechanical stimulation of the oral mucosa as well as the palatal and tongue muscles.
Materials and Methods
Within the framework of a prospective study, 40 patients were asked about their subjective perception with regard to snoring volume by using a visual analogue scale with 10 fields . from 1 to 10. This was done at the beginning of the study and after 1 month of use. Subsequently, the change between the two measured values from the beginning and after one month was considered. After one month of use, it was also asked whether there was still any snoring noise at all. A little change was defined if the change was less than three fields. A significant change was defined as more than three fields of improvement.
Ten of these subjects were additionally examined in a sleep laboratory. The apnea-hypopnea index (AHI), the oxygen desaturation, the acceleration of the heart rate during sleep and the snoring index were determined by means of polygraphy before using the training device and after one month. The Somnotouch recording device from Somnomedics,Germany, was used for this purpose.
The average age of the patients was 40 years (33-50 years). The body mass index (BMI) was 28.3 (25.1-32.1). Statistical analysis was performed using the Dixon and Mood sign test [3].
The pharyngeal muscle trainer Gaumfit® from NSH GmbH, Germany was used (Figure 1). Gaumfit® is made of a medical plastic (USP Class VI). The training device should be worn for 30 minutes throughout the day. It is not intended to be used at night.
The rear edge of the exercise device touches the soft palate, the lateral horizontal plate touches the inside of the cheek or upper lip. The rostral slit is used for transversal adaptation to the individual anatomy of the upper jaw. While wearing the exercise device, the tongue scans this gap. This trains the genioglossus muscle in particular.
Results
Subjective questioning of the 40 subjects revealed no change in snoring volume in 6 subjects. Seven subjects stated that they no longer snored (see Table 1). Thus, the subjective success rate of the biomechanical stimulation of the intraoral soft tissue structures was 85% related to primary snoring. This finding is highly significant with a two sided probability of error of α= 1%.
The objective results are shown in table 2. The apnea-hypopnea index (AHI), oxygen desaturation and snoring index improved in 8 of 10 subjects.
A reduction in heart rate acceleration was registered in 9 of 10 patients (Diagram 2).
Statistical analysis of the objective analysis in the sleep laboratory showed significance at an error probability of α= 5% for the apnea-hypopnea index (AHI), oxygen desaturation,and snoring index. Heart rate acceleration improved significantly with a probability of error of α= 1%.
Figure 2 shows an example of the graphical polygraphy findings of a patient before therapy with Gaumfit®.Figure 3 shows the same patient after one month of application of the biomechanical training device. The snoring events have decreased in frequency and intensity. A green line represents a heavy snoring event and a gray line represents a light snoring event. No dash in the somnogram proves that snoring had not occurred. Heart rate shows significantly less fluctuation after one month and has decreased.The number of SpO2 events (red bars) has also decreased from 4.2 to 0.6. Sleep is now more restful.
Discussion
Physiologic quiet breathing (eupnea) during sleep is nearly silent. The American Sleep Disorders Association defines snoring as a loud, predominantly inspiratory upper airway breathing sound coupled to sleep, without apnea or hypoventilation, resulting from oscillations of the dorsal portions of the soft palate and lateral pharyngeal walls [4].
Novel biomechanical therapy of muscle development using isometric contraction in the soft palate and palatal arches was used to approximate this condition. After four weeks, apnea-hypopnea index (AHI), oxygen desaturation,and snoring index improved in 8 of 10 subjects, and cardiac acceleration improved in 9 of 10 patients. The findings were statistically significant. These results indicate that the subjects' sleep becomes more restful with this therapy.Thus, it is expected that, among other things, the cleansing function of the glialymphatic system is strengthened. As a result, certain neurological diseases, such as dementia, will not occur until a later age or will be reduced in severity.
Patients with primary snoring or sleep apnea syndrome additionally suffer from a disturbance of the function of the nerves in the area of the soft palate. Thereby, the atrophy of the nerve fibers and the muscle fibers correlates with the severity of Primary Snoring and Sleep Apnea Syndrome. Nerve function is more impaired in more severe snoring/sleep apnea syndrome (Patel J.A. et al. 2018) [5].Therefore, therapy for primary snoring and sleep apnea syndrome should always include stimulation of the cranial nerves involved. The pharyngeal muscle trainer Gaumfit® stimulates the following cranial nerves in a biomechanical way: the trigeminal nerve, facial nerve, glossopharyngeal nerve, vagus nerve and hypoglossal nerve. As early as the 1970s, Castillo Moralis was able to show, with his exercise plate limited only to the hard palate, that tongue and swallowing function can be improved by stimulating the nerves.This statement was confirmed by Limbrock et al.(1991) [6].They showed that especially the tongue position and the tension in the lower and upper lip improved after wearing the Castillo-Moralis palatal plate limited only to the upper jaw.
This has been demonstrated in particular in patients with Down syndrome. The biomechanical oral training device Gaumfit® additionally involves the soft palate in its functional range and stimulates the tongue, through the anterior cleft, to take action. This additional tongue action increases the tone in the genioglossus muscle. Thus, the tongue comes into a more rostral position creating an opening in the hypopharyngeal area. This effect also leads to further reduction of snoring volume and improvement of vital parameters during sleep.
The study proves that Gaumfit® has a positive effect on the sleep health of the test persons. Among other things, it is expected to delay the onset of dementia. Since the glialymphatic system can work more effectively during sleep.
The study presented here is limited due to the small number of subjects. Therefore, a continuation with more test persons is necessary in order to then also record special features with regard to gender, age and body mass index.
- J Fischer, G Mayer, JH Peter et al. (2002) Nicht-erholsamer Schlaf. Leitlinie „S2“ der Deutschen Gesellschaft für Schlafforschung und Schlafmedizin DGSM, Berlin/Wien:Blackwell Wissenschafts-Verlag.
- lt;span style='font-weight:bold'>2. Matthew P Pase, Jayandra J Himali, Natalie A Grima, Alexa S Beiser,Claudia L Satizabal, (2017) Sleep architecture and the risk of incident dementia in the community.
- lt;span style='font-weight:bold'>3. B Ramm, G Hoffmann (1982) Lehrbuch der Biomathematik und medizinische Statistik, Stuttgart 195-7
- Schäfer J, Pirsig W (1990) Leitsymptom Schnarchen:Vom fakultativen Schnarchen bis zum obstruktiven Schlafapnoe-Syndrom. In: H. Ganz & W. Schätzle (Hg.) HNO-Praxis heute, 10. Auflage, Berlin: Springer 37-8
- Patel JA, Ray BJ, Fernandez-Salvator C, Gouveia C, Zaghi S, Camacho M (2018) Neuromuscular fubction of the soft palate and uvula in snoring and obstructive sleep apnea: A systematic review Am J. Otolaryngol.
- Limbrock GJ, Fischer-Brandies H, Avalle C (1991) Castillo-Morales`Oriofacial Therapy. Treatment of 67 Children with Down Syndrome Development Medicine & Child Neurology.
FIGURE 1

Figure 1: The throat muscle trainer Gaumfit®
FIGURE 2
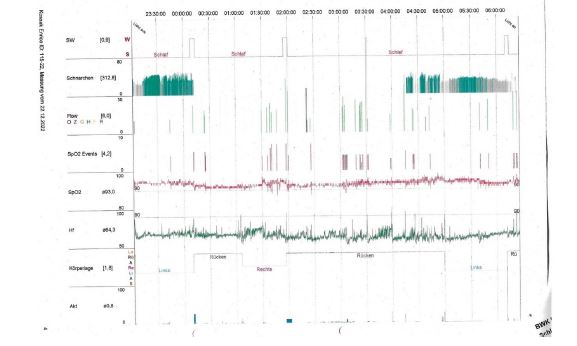
Figure 2: Somnogram before application of Gaumfit® (Schlaf = Sleep; Schnarchen = Snoring)
FIGURE 3
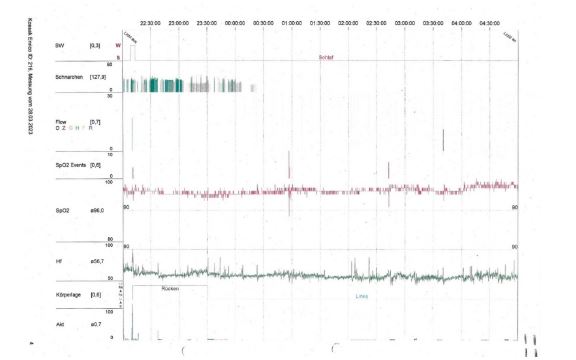
Figure 3: Somnogram after 1 month of application of Gaumfit® (Schlaf = Sleep; Schnarchen = Snoring)
Diagram 1
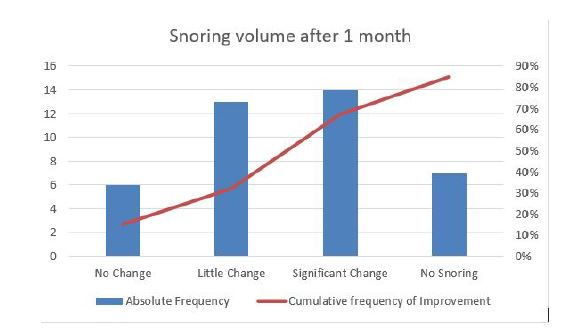
Diagram 1: Change in subjectively perceived snoring volume after 1 month
Diagram 2
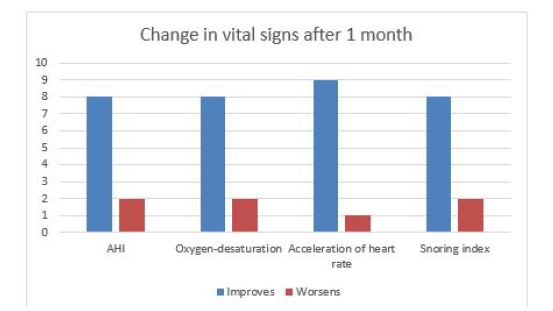
Diagram 2: Change in vital signs after 1 month
Tables at a glance
Figures at a glance