Evaluation of the Accuracy of Transferring Copings for Dental Implants Using Different Impression Techniques
Received Date: June 30, 2023 Accepted Date: July 31, 2023 Published Date: August 03, 2023
doi: 10.17303/jdoh.2023.10.201
Citation: Omar Alageel, Omar Alsadon (2023) Evaluation of the Accuracy of Transferring Copings for Dental Implants Using Different Impression Techniques. J Dent Oral Health 10: 1-8
Abstract
Objective: The accuracy of implant-supported prostheses is influenced by the technique used to record and transfer implant impressions. This study aimed to measure and compare the accuracy of the direct impressions of splinted, non-splinted, and adhesive-coated copings.
Methods: An acrylic master model with four fixtures on the right and left sides of the maxillary arch at sites (1): 13, (2): 15,(3): 23, and (4): 25. Fifteen impressions were made using all three direct techniques: (Group I), non-splinting; (Group II),splinting with auto-polymerizing acrylic resin; and (Group III), coating with an adhesive. The horizontal distances between fixture sites 1-2 and 3-4 were measured using a traveling microscope. Differences in distance between groups were analyzed using one-way ANOVA. Results: Group I showed the lowest accuracy of all the techniques (p≤0.05). There was no significant difference in the accuracy between groups II and III (p≥0.05). Groups II and III showed higher accuracy than Group I.
Conclusion: The impression technique with copings coated with auto-polymerizing acrylic resin and adhesive was more accurate than that with non-splinted copings.
Keywords: Impressions Techniques; Multiple Implants; Accuracy; Horizontal Distance; Splinting Technique
Introduction
A dental impression is a negative imprint of the tooth structure and soft oral tissues, which produces a positive replica of the oral structure. It can be used as a record for fabricating dental prostheses in dental laboratories [1].In implant-supported prostheses, implant positions are transferred to a stone cast with implant analogs using impression materials and copings [2]. Transferring the position of dental implants correctly in relation to adjacent implants or teeth is crucial for the fitting and success of implant- supported prostheses [2,3]. Therefore, it is important to consider the accuracy of transfer systems when fabricating implant-supported prostheses.
The accuracy of implant-supported prostheses is influenced by several factors, such as the type, depth, number, and angulation of the dental implant, as well as the impression material and technique [1,3-5]. An inaccurate fit between prostheses and implants can be associated with biological complications, such as soft tissue inflammation,plaque accumulation, and marginal bone loss, and therefore, the possibility of implant loss [1,5-7]. In addition, misfitting the implant-supported prosthesis can cause mechanical complications, including fracture and screw loosening, wear of the implant components, and chipping or cracking of the ceramic veneer [2,5,7].
Several impression techniques have been suggested for accurate passive fitting of prostheses on multiple dental implants [6,8]. Two basic traditional impression techniques,indirect (closed tray) and direct (open tray), can be used to transfer implant positions from the patient’s mouth to the working cast [1,3,8]. In the indirect or closed tray technique, impression-transfer copings are retained on the implants for impression, and then repositioned into the impression after polymerization [8]. This technique is easy to apply in the clinical setting and does not require individual trays. However, the main disadvantage of the indirect impression technique is the inaccuracy of repositioning the copings to their original positions [6,8].
In direct and open-tray techniques, impression transfer copings are attached to the impression, and the window should be sufficient to accommodate the transfer copings [6,8]. The main drawback is the possible fracture of the cast during its separation from the impression [3,6]. The direct or open tray technique is the most popular technique for multiple-implant prostheses [5].
In the direct technique, transfer copings of the implant can be non-splinted or splinted, with splinting preventing coping movements inside the impression [3,6,8].Several methods have been suggested to enhance the accuracy of multiple implant impressions, such as splitting the impression copings with an acrylic resin material to maintain the correct relationship between the impression copings [5,9]. Nevertheless, splinting impression copings can be time-consuming, uncomfortable for the patient, and difficult to apply in the posterior region [5]. Another simple procedure for enhancing the implant impression accuracy is the application of an adhesive coating to the surface of the coping. This creates a strong connection between the coping and the impression material. This technique can decrease the number of micromovements of the coping inside the impression material [10].
Conflicting outcomes have been reported regarding the accuracy of both non-splinted and direct-splinted impression techniques [1,2,5,11-13]. Therefore, this study was designed to evaluate the dimensional accuracy of stone casts in relation to an acrylic master multiimplant model obtained using different direct impression techniques. This study aimed to measure and compare the accuracy of direct impressions of splinted, non-splinted, and adhesive-coated copings. The null hypothesis of this study was that splinting, non-splinting, and adhesive-coated copings would not affect impression accuracy.
Material and Method
The flowchart of the study procedure is shown in Figure 1. A maxillary dental study model with four implants replacing the canine and second premolars on each side was used as the master model. A silicon duplicate material (Adisil;Siladent, Munich, Germany) was used to duplicate the master model with self-cured acrylic resin. A master acrylic model representing an edentulous mandibular arch was fabricated,with four implant fixtures fixed to the model (ITI Dental Implant System; Straumann AG, Basel, Switzerland),which was selected because it is one of the commonly used dental implants by investor institutions (Figure 2).The milling machine contained a low-speed straight handpiece drill mounted on a holder that was used to drill four implant sites on the acrylic model. The four implant fixtures were then fixed in holes using cement.
Three different groups of impression techniques,represented by Groups I, II, and III, with a total of 15 impressions (N=15), were made with 5 for each technique.The first group (Group I) used a direct transfer impression technique with non-splinted copings. The second group (Group II) used a direct transfer impression technique with copings splinted with an acrylic splint. An acrylic splint was made one day before the impression procedure and then divided into three pieces. The pieces were rejoined using an autopolymerizing resin. The third group (Group III) used a direct transfer impression technique with copings splinted and coated with a polyether tray adhesive (Impregum, 3MESPE, Seefeld, Germany).
The custom trays (N=15) were made from auto-polymerizing acrylic resin with four windows cut off from each tray in the implants placed to provide access for the pick-up and to expose the transfer copings. A brush was used to paint the impression surface with the manufacturer recommended adhesive and was allowed to dry for 15min before adding the impression material. The polyether based impression material (Impregum Penta Soft,3M EPSE, Seefeld, Germany) was mixed using an automatic mixing device, according to the manufacturer’s guidelines.These impression materials have been widely used because of their excellent deformation resistance and dimensional stability, and for precise detail capture [14]. The impression material was applied using a syringe over the tray and around the impression copings to achieve full coping coverage.The impression was left to set for five minutes following the manufacturer’s instructions, and then separated from the master model when the copings remained in the impression. The impressions were then rinsed with water for 10 s and air dried. Subsequently, implant analogs were attached to the transfer coping. Impressions were then left to set for 30 min before pouring using hard stone (ADA classification IV die stone) with a vacuum mixing unit. The impressions were left to set for one hour before screwing the transfer copings directly onto the implants.
A traveling microscope (measuring microscope 3800, Titan Tool Supply Co. Inc., Buffalo, NY, USA) was used to measure the distance between the reference points of the copings. All measurements were performed by a single well-trained examiner. The distance between the canine and second premolar on the right side was referred to as 1-2 while the distance between the canine and second premolar on the left side was referred to as 3-4. The distances between the reference points on the stone cast and acrylic master model were compared. The measurements were repeated three times for each distance for all the 15 samples. The mean of the three measurements was calculated and used for further statistical analyses.
The sample size was calculated using G*Power software (v.3.01; Kiel, Germany) based on a pilot study comparing two means with 80% power and an alpha of .08, with an estimated effect size of .05. Means and standard deviations (SD) were calculated, and the data were checked for normality using a histogram. A 1-way analysis of variance (ANOVA) was used to determine statistical significance between the groups following Tukey’s test for multiple comparisons conducted with Origin software (v.9.0; Origin Lab,Northampton, MA). Statistical significance was set at P<0.05.
Results
The mean and standard deviation of the distance between the copings for the different impression techniques are shown in table 1. The results exhibited that there was a statistically significant difference (p<0.05) in the distances between the dental implants with different impression techniques.However, the differences between the groups were statistically significant on the left side but not on the right side of the arch. The impression technique in which the implant copings were coated with an adhesive (group III) showed a smaller distance on the left side (37.26±.043) than groups I and II (37.74±.114, and 37.60±.242, respectively).
The mean and standard deviation of the change in distance (μm) between the copings in the master model and the casts for the different groups are presented in Figure 3 and Table 2. The results showed that the accuracy of the impression technique compared to that of the master model varied among the different techniques. Groups II and III,which were splinted and coated with adhesive, were more accurate (p≤0.05) than the non-splinted group (Group I).However, there was no significant difference in accuracy between Groups I and II (p≥0.05), and the accuracy was similar.
Discussion
In this study, the most accurate impression technique was the impression technique with copings splinted with acrylic resin and coated with adhesive; thus, the null hypothesis of the study was rejected. Significant differences were found between splinted and non-splinted impression techniques. The results of this study suggest that the accuracy of the impression technique directly affects the passive fit of implant-supported prostheses, and that splinting reduces the movement of impression copings within the impression material. Splinted impressions also led to significantly fewer errors in the master cast, which is essential for prosthesis fabrication. Overall, these findings suggest that splinted impressions or adhesive coatings should be used to ensure a more accurate fit of the prosthesis.
Conflicting results have been previously reported.For example, Vigolo et al. and Richi et al. suggested that direct splinted transfer impression techniques are more accurate than direct non-splinted transfer impression techniques [10,13]. In contrast, Serrano et al. found that the direct non-splinted technique was more accurate than the direct-splinted technique. Furthermore, Burn et al., Tarib etal., Herbest et al. Naconecy et al., and Daoudi et al. found there are no significant differences between splinted and non-splinted techniques [4,6,12,15,16]. Flugge et al. suggested that the available data regarding implant impression accuracy have low evidence and do not provide sufficient information [2].
The results of this study agreed with those of several previous studies conducted by Vigolo et al. and Richi etal., which showed that direct splinted transfer impression techniques were more accurate than direct non-splinted transfer impression techniques [10,13,14]. It was also found that there were no significant differences between splinted impression techniques splinted with acrylic resin and adhesive coating [4,14-16]. The degree of micromovement of impression copings inside the impression material is reduced by the chemical bonding generated by the adhesive coating of the copings, which might minimize the possibility of rotating the coping inside the impression [14]. This may explain the high accuracy of adhesive coating techniques [14].
Different methods for splinting implant copings with acrylic resin can be performed, including using prefabricated acrylic resin bars, using acrylic splints, or by using dental floss as a scaffold, then polymerizing with autopolymerizing acrylic resin. An autopolymerizing acrylic resin splint requires sectioning into pieces and rejoining them with resin. The small shrinkage of the acrylic resin pattern used for the initial splinting or joining could be the reason for the inaccuracies [17]. The small shrinkage of the acrylic resin pattern used in the splinting method (Group II) could be the reason for Group II inaccuracies [17]. In this group,the acrylic resin splint was sectioned between the copings and then returned. Thus, the amount of resin used for the initial splinting or joining of the sections could have influenced the accuracy [17]. Prefabricated acrylic resin bars can be used to minimize shrinkage and splint formation using the same acrylic material [18,19].
Dental prostheses, including implant-supported prostheses, require the highest precision and accuracy in all steps and procedures [10,19]. Impression is sensitive to several factors. For instance, impression material shape, size, and angulation of copings [10]. Currently, dental implant manufacturers provide standardized procurers using either conventional or digital methods; however, it is important for dental clinicians and laboratory technicians to know the factors that influence prosthetic success. Therefore, it is critical to determine potential errors when fabricating a prosthesis.They should ensure that the impression is made accurately and that the prosthesis is made to the correct specifications.
A previous study concluded that the most accurate transferring coping technique for implants is the open technique with splinted squared transfer copings, as well as the optical intraoral system with powder [20]. Despite the revolution in digital technology, traditional methods are still accurate and widely used. However, the inaccuracy of digital impressions depends on the scanner’s capability, scan protocol,and operator’s experience [2]. The clinical implications for traditional and digital methods cannot be determined based on the presented data.
A limitation of this study is that the methods only allow for the evaluation of horizontal distortion in transfer copings. Additional investigations are required to determine the clinical applicability of three-dimensional impression coping movements. In addition, the results of this study were limited to four implants, which might not represent clinical cases with higher or lower numbers of dental implants. Future research is necessary to determine the accuracy of transferring copings using various coping shapes (number, length, width, and indentation depth), as well as different implant types and impression materials. Further studies are needed to assess the in vivo use of the digital method for dental impressions and compare them with the manual methods.
Conclusion
With the limitations of this study, the following conclusions were drawn:
- The impression technique with nonsplinted copings showed the lowest accuracy compared to splinted copings.
- The impression technique with adhesivecoated copings was the most accurate compared with non-splinted copings.
- The impression technique for splinting with acrylic resin or coating with adhesive showed no significant difference in the dimensional accuracy.
Acknowledgments
The authors extend their appreciation to the Researchers Supporting Project (no. RSPD2023R634), King Saud University, Riyadh, Saudi Arabia, for supporting this study. Also, they would like to thank Prof. Mohamed Hashim for technical support to perform this study.
Data Availability
The data used to support the findings of this study will be available from the corresponding author upon request.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethics approval statement
Ethics approval is not required for this in-vitro study
- Ismail IA, MN Alhajj (2020)Accuracy of different impression techniques for multiunit implant restoration: A qualitative in vitro study. J Prosthet Dent 124: e1-729.
- Flügge T et al. (2018) The accuracy of different dental impression techniques for implant-supported dental prostheses:A systematic review and meta‐analysis. Clin Oral Implants Res 29: 374-92.
- De Avila ED et al. (2014) Effect of splinting in accuracy of two implant impression techniques. J Oral Implantol 40: 633-9.
- Herbst D et al. (2000) Evaluation of impression accuracy for osseointegrated implant supported superstructures. J Prosthet Dent 83: 555-61.
- Liu DY et al. (2019) Accuracy of different implant impression techniques: Evaluation of new tray design concept. J Prosthodont 28: e682-e7.
- Tarib N et al. (2012) Evaluation of splinting implant impression techniques: two dimensional analyses. Eur J Prosthodont Restor Dent 20: 35.
- Abduo J RB Judge (2014) Implications of implant framework misfit: a systematic review of biomechanical sequelae. Int J Oral Maxillofac Implants 29: 608-21.
- YASAR MN et al. (2022) Implant Impression Techniques using Different Materials and Methods: A Review. J Clin Diagn Res 16.
- Papaspyridakos P et al. (2014) Accuracy of implant impressions for partially and completely edentulous patients: a systematic review. Int J Oral Maxillofac Implants 29.
- Vigolo P, Majzoub Z, Cordioli G (2003) Evaluation of the accuracy of three techniques used for multiple implant abutment impressions. J Prosthet Dent 89: 186-92.
- Serrano JG et al. (1998) An accuracy evaluation of four removable die systems. J Prosthet Dent 80: 575-86.
- Burns J et al. (2003) Accuracy of open tray implant impressions: an in vitro comparison of stock versus custom trays. J Prosthet Dent 89: 250-5.
- Richi MW, S Kurtulmus-Yilmaz, O Ozan (2020) Comparison of the accuracy of different impression procedures in case of multiple and angulated implants. Head Face Med 16: 1-12.
- Lahori M, R Nagrath, P Agrawal (2014) An in vitro study to compare the accuracy of the master cast fabricated by four different transfer impression techniques for single--tooth implant replacement. J Indian Prosthodont Soc 14: 78-84.
- Naconecy MM et al. (2004) Evaluation of the accuracy of 3 transfer techniques for implant-supported prostheses with multiple abutments. Int J Oral Maxillofac Implants 19.
- Daoudi MF, DJ Setchell, LJ Searson (2004) An evaluation of three implant level impression techniques for single tooth implant. Eur J Prosthodont Restor Dent 12: 9-14.
- Selvaraj S et al. (2016) Comparison of implant cast accuracy of multiple implant impression technique with different splinting materials: An in vitro study. J Indian Prosthodont Soc 16: 167.
- Ghanem RA et al. (2016) Dimensional accuracy of different techniques used for complete-arch multi-implant impressions. J Investig Clin Dent 7: 225-31.
- Lahori, Mahesh, Lanka Mahesh, Rahul Nagrath, Shweta Singh (2012) An evaluation of the accuracy of multiple implant impression techniques: an in vitro study. J Implant Adv Clin Dent 57-69
- António HJ Moreira et al. (2015) Accuracy Comparison of Implant Impression Techniques: A Systematic Review. Clin Implant Dent and related Res.
FIGURE 1
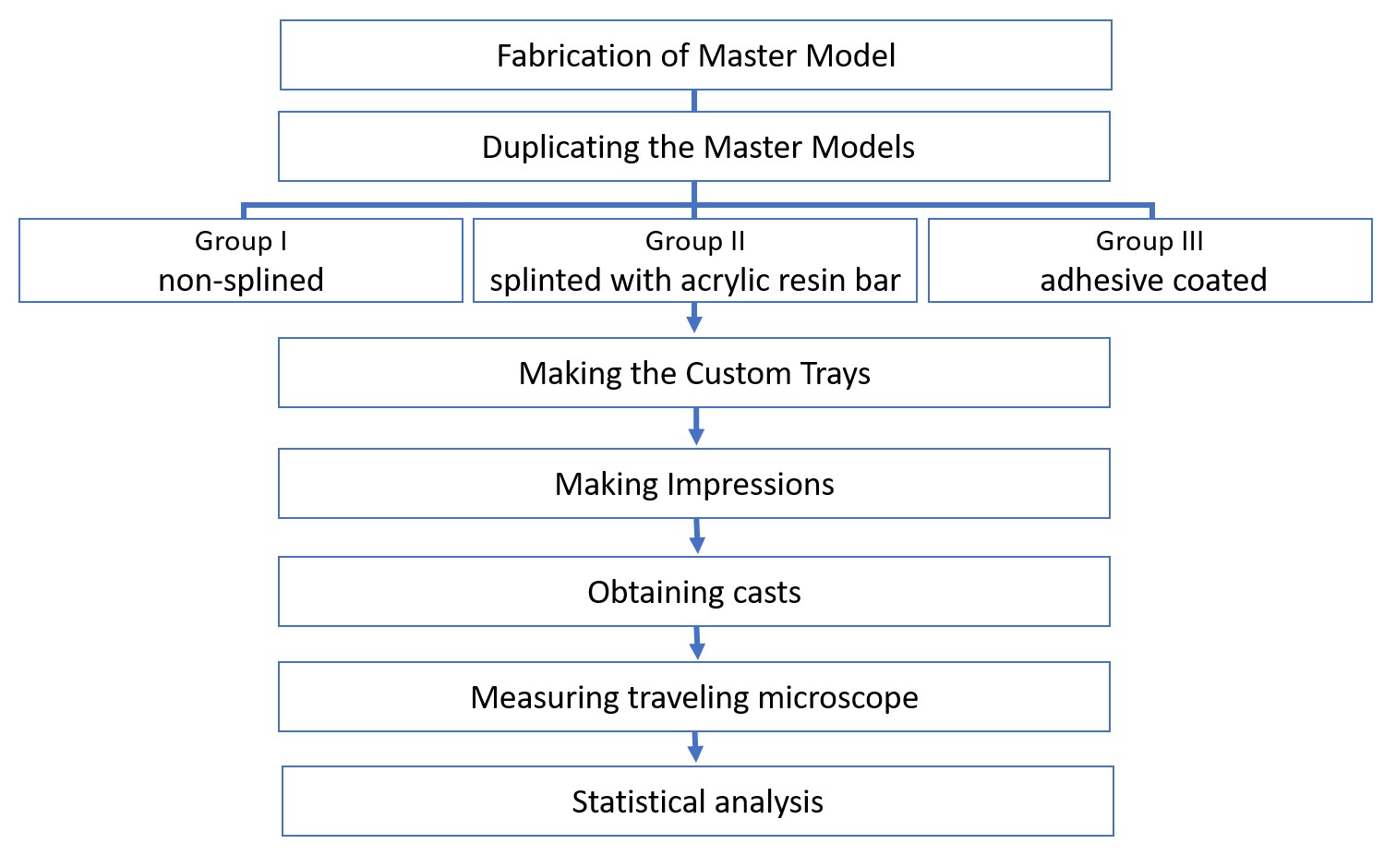
Figure 1: Flow chart of the procedure used in the study
FIGURE 2

Figure 2: Photograph of the (A) acrylic resin master model, (B) master cast with the implant analogs
FIGURE 3
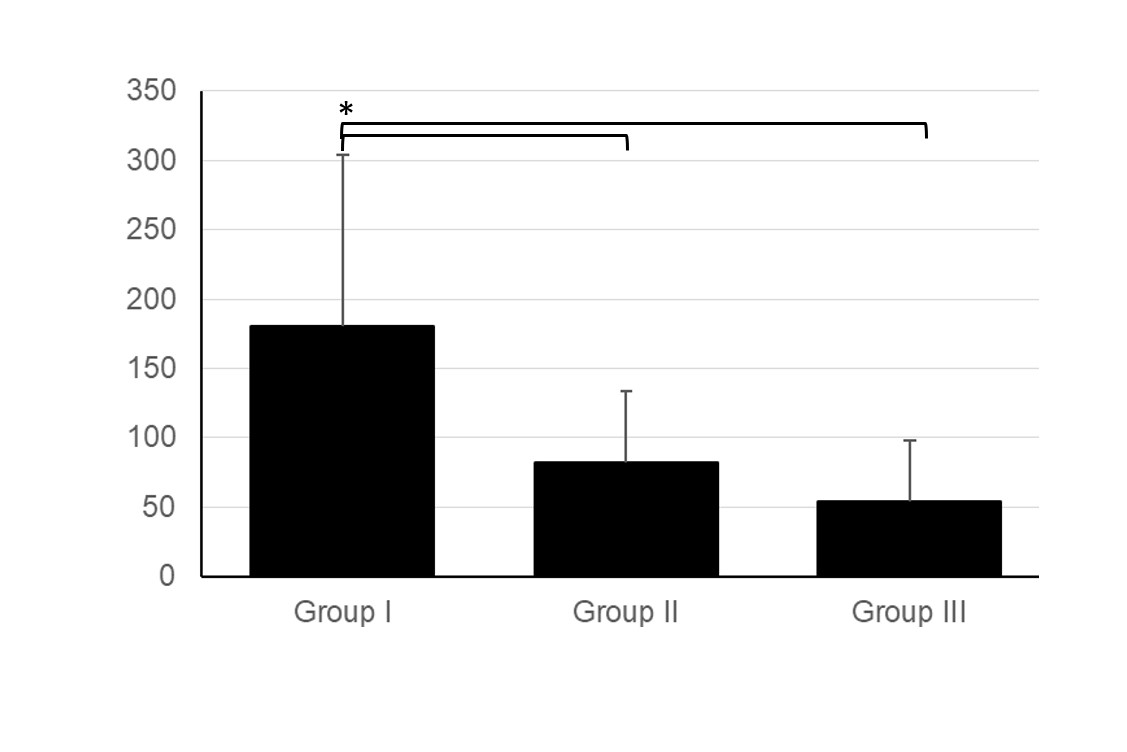
Figure 3: Chart showing the change in distance (μm) between the copings in the master model and casts for different groups (Group I: non-splinting; Group II: splinting with auto-polymerizing acrylic resin; and Group III: coating with an adhesive). * indicate significant difference (p≤0.05) between groups
Tables at a glance
Figures at a glance