Retrieval of Separated Instrument using Modified Loop Masserann Technique in Re-RCT Case of 11year Old Girl: Case Report
Received Date: August 05, 2023 Accepted Date: September 05, 2023 Published Date: September 09, 2023
doi: 10.17303/jdoh.2023.10.202
Citation: Pramila Amaltass, Roli Agrawal, Mrinali Shukla, Sowmya NR, Srinandan Pradhan et al. (2023) Retrieval of Separated Instrument using Modified Loop Masserann Technique in Re-RCT Case of 11year Old Girl: Case Report. J Dent Oral Health 10: 1-7
Abstract
Over the years, innumerable advancements have been employed in endodontic file designs and dimensions. In spite of that, file separation has been the most common exasperating event for the clinicians questioning the overall treatment prognosis. Managing such clinical mishaps can be even more stress that may result in further unfavourable outcomes. Therefore, considering all the possibilities, retrieval of separated instrument using MasseranTM Endodontic Kit have been attempted through this case scenario.
Keywords: Instrument Retrieval; Instrument Separation; Modified Loop Technique
Introduction
A successful accomplishment of an endodontic treatment depends upon the complete removal of causative microorganisms from root canal complex. Owing to this fact, studies have demonstrated the high success rate after the elimination of endodontic pathogens before obturation which was found to be as high as 94% [1,2]. At the same time another study showed incomplete removal of bacteria could be the reason for treatment failure [1].
However, microbial cause is not the only deciding factor for good prognosis. Clinician can come across the various other procedural difficulties such as formation of ledges, strip perforations, or separation of instruments in the canals [3]. Among these, Intracanal separation of endodontic instruments is one of the most commonly encountered procedural errors with the incidence of 0.5-5% [4]. A retained separated endodontic file can present as hinderance to adequate biomechanical shaping of root canal system. Further, it may lead to irritation of periapical tissues, if part of retained file protrudes out through apex. It has been revealed that intra radicular instrument separation lower the success rate by 14% on contrary to those with no instrument separation [5]. Therefore, it becomes utmost necessity to either bypass or retrieve the separated instrument.
Over the years, various techniques have been advocated for the removal of separated instruments such as MasseranTM Endodontic Kit, Ultrasonic device the Cancellier IRSTM and the Ruddle IRSTM [6]. As per the current research, the use of piezoelectric ultra sonics tips have demarcated the better outcomes in both straight and curved canals [7]. Overall success rate for retrieval of separated instruments has been found to be 55-79% [8].
The following case report illustrate the usage of MasseranTMEndodontic Kit for retrieval of separated instrument during retreatment of maxillary central incisor.
Case Report
A 11 year old female patient reported to department of Pediatric and preventive dentistry with chief complaint of pain in upper front tooth region for past 1 week. On intraoral examination, swelling was found on palatal aspect i.r.t 11.
Radiographic examination further revealed the over obturationas well as periapical radiolucency with respect to same tooth. Finally, after thorough clinical and radio graphical investigations, definitive diagnosis was made as phoenix abscess i.r.t 11 (figure1).Accordingly, Re RCT was planned. In the course of retreatment, while removing the gutta percha, a #30 barbed broach got separated in the canal.
On radiographic examination, separation of file at apical third of canal was found (figure2).
Since it was retreatment case with periapical infection, file retrieval was decided upon using, MasserannTM Endodontic Kit rather than going for conventional procedures.
Initially, the remaining part of the separated instrument was evaluated. The distance from the tip of the fractured file to D16 (6 mm) was measured and this value was subtracted from the original length, 16 mm, of the file. This gave us the length of the separated remaining fragment in the canal (10 mm).
Further, coronal end of the fragment was accessed by funneling the root canal with sequential use of GatesGlidden drills with modified flat end tips. After achieving the straight line access to coronal end of fragment, preselected trephan bur of diameter 1.2mm was centered into the canal to create trough around coronal end of fragment. Thereafter, extractor tube of same diameter was glided onto the trough to reach the fragment. Adequate placement of extractor tube over the fragment was ensured radio graphically. Following this, plunger rod was slid manually inside the extractor tube in clockwise direction to hold the fragment against its wall. However, all the attempts to get the hold of file fragment went futile as fragment was much more engaged towards distal wall. Therefore, through the plunger rod, loop of 0.14-mm wire was placed around the upper free part of fragment plunger rod. Once the tight grip was secured via tactile sense, the whole assembly was rotated in anticlockwise direction so as to unwind fragment from dentin. Finally, the whole assembly was withdrawn in same manner with retrieved instrument (figure3& 4).
Although these are other alternative techniques such as Endosicherheits system, Braiding technique, Ultrasonics, Combined technique, wire loop technique, Endo-extractor technique [10].
In the above mentioned cases the use of modified loop masserann technique was planned for this procedure. Patient experience relief of pain complete removal of gutta percha and was satisfied with the treatment outcome follow of the patient was done every three months and after six months follow up clinical and radiographic examination revealed that patient was asymptomatic and with no sign of infection and bone healing was seen
“The dentist who has not fractured the tip of a reamer, file or broach has not treated many root canals. Who has not felt the pang, the anguish, the mortification caused by the breaking of an instrument? That moment of remorse lives on for days until it is faded out by time”, quoted by Grossman. Instrument separation not only creates the hurdle for access to apical foramen but also impedes the operator’s skill in providing the effective treatment. Such endodontic cases often creates state of perplexity regarding the prognosis. Before any clinical decision making, one should assess the condition of the root canal (vital or nonvital), tooth (symptomatic or asymptomatic, with or without periapical pathology), level of cleaning and shaping at the time of separation, the level of separation in the canal [11].
A wide range ofendodontic instruments such as Gates-Glidden burs, carbon steel or stainless steel (SS) (K-- files, Hedström files, barbed broaches, reamers), nickel-titanium (NiTi) rotary instruments, lateral spreaders, peeso reamers, spiral fillers and irrigation needle have been reported to fracture within root canals [12-15]. However, many studies have claimed higher prevalence of fracture among SS files and NiTi rotary files as compared to other instruments [16-18]. Iqbal and co-workers conducted a retrospective study and found that among 81 separated files, the majority were NiTi rotary instruments and probability of having file separation in the apical third is 33 times higher than the coronal third and 6 times higher compared to the middle third pertaining to its small diameter & curvature [19].
On the contrary, bulk of literature reported the similar range of incidence of fracture among SS & NiTi instruments which was 0.4-5% [20-22]. Numerous factors can be attributed towards separation of instruments which includes operator experience, rotation speed, degree of canal curvature, instrument design and technique, torque, manufacturing process, and absence of a well-established glide path [23].
File retrieval cases can be managed by both surgical as well as non-surgical approach. In our case scenario, non-surgical (ortho grade retrieval) method seemed to be appropriate. The ortho grade retrieval depends on cross-sectional diameter, length, curvature of the canal; dentin thickness and morphology of the root; composition, cutting action (clockwise or counter-clockwise) of the instrument; length, location, and amount of binding or impaction of the fragment in the canal [24]. Additionally, There are several patient factors such as extent of mouth opening, time constraints, anxiety level, and motivation to retain teeth which need to be taken into consideration [25].
In this case, MasserannTM Endodontic Kit has emerged as quantum leap among all the stated techniques & procedures for removal of intra canal obstructions such as silver points and fragments of endodontic instruments [25]. The Masserann Kit (Micro-Mega, Besancon, France) is most widely used instrument for the removal of separated instruments [27-29] It consists of an assorted series of color coded trephan burs with diameter ranging from 1.1 to 2.4 mm along with the extractor tube which are available in two sizes (1.2 and 1.5 mm in outer diameter) and other accessories. The trephan burs are latch type instruments that rotates in counter-clockwise direction to create a suitable space for the extractor tubes by cutting the surrounding dentin around the coronal end of the fragment. An extractor with a plunger rod (stylet) is used to grip and dislodge the fragment from canals [29,30].
Inspite of all the above advantages of using MasseranTM kit , it has its own limitations such as time consuming procedure , technique sensitive as difficulty in engaging loop with block instrument.
Conclusion
Although this case report has outlined the file retrieval procedure successfully, still this process has its own setbacks. Removal of considerable amount of radicular dentin while retrieval may lead to iatrogenic error like perforation thereby, weakening the overall tooth structure. And as it has been rightly said “An ounce of prevention is better than pound of cure”. Therefore, clinician should always act in accordance to certain principles which can prevent this troublesome incident to much extent.
- Sjogren U et al. (1997) “Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis.” International Endodontic Journal 30: 297-306.
- Moller AKE JR et al. (1981) “Influence on periapical tissues of indigenous oral bacteria and necrotic pulp tissue in monkeys.” European Journal of Oral Sciences 89: 475-84.
- Souter NJ, Messer HH (2005) Complications associated with fractured file removal using an ultrasonic technique. J Endod 31: 450.
- Gandevivala A, Parekh B, Poplai G, Sayed A (2014) Surgical Removal of Fractured Endodontic Instrument in the Periapex of Mandibular First Molar. J Int Oral Health 6: 85-8.
- Yousuf, Waqas, Moiz Khan, Hasan Mehdi (2015) “Endodontic procedural errors: frequency, type of error, and the most frequently treated tooth.” International Journal of Dentistry 1-7.
- Uzun İ, Güler B, Özyürek T (2018) Sewing needle in a root canal: A case report. Oral Biol Dent 2: 11.
- Nagai O, Tani N, Kayaba Y, Kodama S, Osada T (1986) Ultrasonic removal of broken instruments in root canals. Int Endod J 19: 298-304.
- Andrabi SM, Kumar A, Iftekhar H, Alam S (2013) Retrieval of a separated nickel titanium instrument using a modified 18-guage needle and cyanoacrylate glue: A case report. Restor Dent Endod 38: 93-7.
- Hülsmann M, Schinkel I (1999) Influence of several factors on the success or failure of removal of fractured instruments from the root canal. Endod Dent Traumatol 15: 252-8.
- Lohar J, Sood H, Gosai P, Shekh TM (2011) 3P's in Retreatment Endodontics-An Often Forgotten Virtue. J Pharm Bioallied Sci 11: 76-80.
- Thirumalai AK, Sekar M, Mylswamy S (2008) Retrieval of a separated instrument using Masserann technique. J Conserv Dent 11: 42-5.
- Arcangelo CM, Varvara G, Fazio PD (2000) Broken instrument removal two cases. J Endod 26: 568-70.
- Fors UGH, Berg JO (1986) Endodontic treatment of root canals obstructed by foreign objects. Int Endod J 32: 2-10.
- Chenail BL, Teplitsky PE (1987) Orthograde ultrasonic retrieval of root canal obstructions. J Endod 13: 186-90.
- Parashos P, Messer HH (2006) Rotary NiTi instrument fracture and its consequences. J Endod 32: 1031-43.
- Cheung GS (2009) Instrument fracture: mechanisms, removal of fragments, and clinical outcomes. Endod Topics 16: 1-26.
- Bergenholtz G, Lekholm U, Milthon R, Heden G, Ödesjö B, Engström B (1979) Retreatment of Endodontic fillings. Scand J Dent Res 87: 217-24.
- Kerekes K, Tronstad L (1979) Long-term results of endodontic treatment performed with a standardized technique. J Endod 5: 83-90.
- Sjögren U, Hagglund B, Sunqvist G, Wing K (1990) Factors 37 affecting the long-term results of endodontic treatment. J Endod 16: 498-504.
- Iqbal MK, Meetu R, Kohli, Kim JS (2006) A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate programme: a PennEndo database study. J Endod 32: 1048-2
- Pettiette MT, Connor D, Trope M (2002) Procedural errors with the use of nickel-titanium rotary instruments in undergraduate endodontics. J Endod 28: 259.
- Ruddle CJ (2004) Nonsurgical retreatment. J Endod 30: 827-45.
- Ramirez-Salomen M, Soler-Bientz R, de la Garza-- Gonzalez R, Palacios-Garza CM (1997) Incidence of 44. Lightspeed separation and potential for bypassing. J Endod 23: 586-7.
- Roda RS, Gettleman BH (2006) Nonsurgical retreatment. In: Roda RS, Gettleman BH, editors. Pathways of the Pulp. 9th ed. St. Louis: CV Mosby 982-90.
- Hulsmann M (1993) Methods for removing metal obstruction from the root canal. Endod Dent Traumatol 9: 223-37.
- Vyavahare N, Kulkarni M, Desai N (2018) Retrieval of a separated nickel–titanium instrument and a stainless steel H-file using a novel tube, loop and file technique. J Int Clin Dent Res Organ 10: 88-92.
- Ruddle CJ (2001) Nonsurgical endodontic retreatment. In: Cohen S, Burns RC, editors. Pathways of the Pulp. 8th ed. St Louis, Mo: Mosby 875-929.
- Gencoglu N, Helvacioglu D (2009) Comparison of the different techniques to remove fractured endodontic instruments from root canal systems. Eur J Dent 3: 90-5
- Brito-Junior M, Normanha JA, Camilo CC, Faria-e-Silva AL, Saquy PC, Ferraz MA et al. (2015) Alternative techniques to remove fractured instrument fragments from the apical third of root canals: report of two cases. Braz Dent J 26: 79-85.
- Masserann J (1971) "Entfernen metallischer Fragmente aus Wurzelkanalen" (Removal of metal fragments from the root canal). J Br Endod Soc 5: 55-9.
FIGURE 1
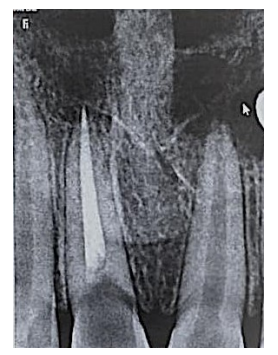
Figure 1: Pre-Operative radiograph
FIGURE 2
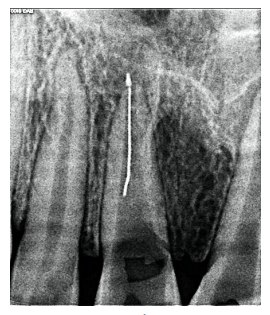
Figure 2: Broach separation
FIGURE 3

Figure 3: Broach engagement radiograph
FIGURE 4
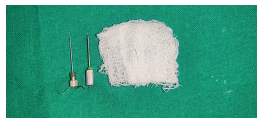
Figure 4: Retrieved broach
FIGURE 5

Figure 5: Post-Operative radiograph (After 6 months)
Figures at a glance