From Glucose to Gums: Exploring the Oral Side of Diabetes
Received Date: September 07, 2023 Accepted Date: October 07, 2023 Published Date: October 09, 2023
doi: 10.17303/jdoh.2023.10.203
Citation: Amit Kumar Dey, Anu Grover, Ashutosh Mishra, Shivanjali Kumar (2023) From Glucose to Gums: Exploring the Oral Side of Diabetes. J Dent Oral Health 10: 1-16
Abstract
This comprehensive review provides an in-depth exploration of the association between hyperglycemia and oral health, focusing on the significance of investigating hyperglycemia-induced oral complications. The overview of hyperglycemia and oral health highlights the growing awareness of their interconnection and the need for comprehensive patient care. Diabetes-related periodontal disease is examined in detail, elucidating the pathophysiology, clinical presentation, and treatment considerations. Similarly, the influence of hyperglycemia on dental caries development and risk assessment in hyperglycemic individuals are discussed, alongside preventive strategies and management options. The review also delves into oral thrush, dry mouth (xerostomia), and burning mouth syndrome, outlining their association with hyperglycemia and the corresponding management approaches. Moreover, the impact of hyperglycemia on immune function and its role in oral infections and complications are addressed, suggesting strategies for prevention and management in hyperglycemic patients. Integrating oral health into diabetes management and emphasizing the importance of screening and early detection of oral complications are explored as crucial clinical recommendations. Finally, future research directions, including advancements in understanding hyperglycemia-induced oral complications and emerging therapeutic and preventive approaches, are highlighted. This comprehensive analysis provides valuable insights for healthcare practitioners to improve patient care and outcomes for those experiencing oral health issues related to hyperglycemia.
Keywords: Diabetes; Oral manifestations; Hyperglycemia; Diabetologist; Dentist
Introduction
Elevated blood glucose levels, known as hyperglycemia, have substantial implications for oral health, leading to a range of oral complications. One notable effect is diabetes-related periodontal disease, where hyperglycemia weakens the immune system, making it less effective in fighting oral infections. Consequently, this leads to chronic inflammation of the gums and surrounding tissues, resulting in periodontal disease. Additionally, hyperglycemia worsens tooth decay, or dental caries [1,2]. Elevated sugar levels in saliva create favorable conditions for bacterial growth, notably Streptococcus mutans, which generates acids that harm tooth enamel and lead to cavities. In high-- sugar environments, Candida albicans, the fungus responsible for oral thrush, thrives, increasing the vulnerability of individuals with hyperglycemia to this infection. Additionally, dry mouth (xerostomia) is a frequent oral complication as elevated blood sugar levels can reduce salivary flow, causing discomfort and raising the risk of dental caries and oral infections [3-5]. Furthermore, hyperglycemia hinders the healing of wounds, affecting oral tissues following dental procedures or injuries. This delayed healing process can elevate the risk of oral infections. Additionally, nerve dysfunction due to persistently high blood sugar levels may contribute to the development of burning mouth syndrome [6,7]. The weakened immune system resulting from hyperglycemia heightens the susceptibility to various oral infections, such as abscesses, ulcers, and recurrent oral candidiasis. To avert these oral complications, individuals with hyperglycemia must prioritize maintaining optimal glycemic control and scheduling regular dental check-ups. By addressing these concerns, individuals can enhance their oral health, promote overall well-being, and prevent the advancement of these adverse effects associated with hyperglycemia [8,9].
Understanding the link between hyperglycemia and oral complications is vital due to the global rise in diabetes cases. Oral problems like periodontal disease, dental caries, and oral thrush cause discomfort and affect quality of life, putting pressure on healthcare resources and costs. By studying the clinical impact of hyperglycemia on oral health, healthcare professionals can create focused prevention and management methods, improving the well-being of those with diabetes [10-12].
Hyperglycemia-Linked Oral Complications: An Epidemiological Perspective
Global epidemiological data on oral complications resulting from hyperglycemia underscores the significant impact of elevated blood glucose levels on worldwide oral health. Diabetes, a primary contributor to hyperglycemia, currently affects an estimated 463 million adults globally, and this number is projected to reach 700 million by 2045. Extensive epidemiological research has revealed that individuals with diabetes face a substantially higher risk of developing oral complications compared to the general population [13,14]. One of the most prevalent oral complications among individuals with diabetes is diabetes-related periodontal disease, which affects approximately 20-50% of diabetic patients. Dental caries, attributed to increased salivary sugar content in hyperglycemic individuals, affects over 30% of the diabetic population. Additionally, oral thrush, a fungal infection linked to immune system dysfunction caused by hyperglycemia, is found in up to 30% of individuals with diabetes [15,16]. Dry mouth (xerostomia) is estimated to affect 20-60% of diabetic patients, increasing the risk of dental caries and oral infections. Furthermore, studies report a higher incidence of delayed wound healing in the oral cavity of hyperglycemic individuals, further contributing to oral health challenges. The global burden of oral complications resulting from hyperglycemia is substantial, significantly impacting the quality of life for those affected and imposing economic burdens on healthcare systems [17,18].
As the prevalence of diabetes continues to rise, particularly in low- and middle-income countries, the incidence of these oral complications is expected to increase. Addressing this public health issue necessitates comprehensive oral health programs integrated with diabetes management, aiming to prevent, identify, and manage oral complications associated with hyperglycemia on a global scale. Through early detection, education, and optimal glycemic control, a concerted effort can be made to reduce the prevalence and severity of these oral complications, ultimately promoting better oral health and overall well-being in hyperglycemic populations worldwide [19,20].
Diabetes and Oral manifestations: An Intricate Connection
Periodontal Disease
Diabetes-related periodontal disease has garnered significant attention in research literature due to complex interplay between diabetes and oral health. Numerous studies have highlighted the bidirectional relationship, with diabetes exacerbating periodontal disease and vice versa. The chronic inflammatory response triggered by hyperglycemia compromises the immune system, leading to increased vulnerability to periodontal pathogens [21,22]. Conversely, periodontal inflammation can negatively impact glycemic control, contributing to diabetic complications. Research has explored potential underlying mechanisms, such as altered host immune response, impaired collagen metabolism, and dysregulated cytokine levels [23,24].
Hyperglycemia can induce periodontal disease through various mechanisms (Figure 1). Firstly, increased bacterial growth occurs due to high blood sugar levels, providing a favorable environment for bacteria to thrive and form plaque, leading to gum irritation and inflammation. Secondly, people with diabetes may experience a decreased immune response, making it challenging to combat periodontal infections effectively [25,26]. Thirdly, chronic inflammation is common in diabetes, damaging oral tissues over time. Fourthly, poor blood flow in diabetes hinders wound healing and bacterial removal from the mouth. Lastly, hyperglycemia can damage collagen, making the gums more vulnerable to inflammation and infection. The combination of these factors contributes to the development of periodontal disease in individuals with diabetes, potentially leading to tooth loss [27,28].
Hyperglycemia-induced periodontal disease presents with various clinical signs. Gingivitis is the mildest form, marked by inflamed and bleeding gums. Periodontitis is more severe, causing pockets to form between gums and teeth, harboring bacteria and plaque, which leads to bone and tooth loss [29-31]. Diabetes elevates the risk of rapid tooth loss, recurring infections, bad breath, gum, teeth, and jaw pain, and loose teeth as the condition worsens. Recognizing these clinical signs is crucial for early detection and management, underscoring the importance of regular dental check-ups and optimal blood sugar control to halt the progression of hyperglycemia-induced periodontal disease and its impact on oral health [32,33]. Table 1 summarizes the type of oral lesions in a study done on 51 diabetes patients [34].
Individuals with hyperglycemia often exhibit a poorer response to periodontal treatment, hindered by the interference with the healing process [35,36]. Moreover, those with hyperglycemia and periodontal disease face an elevated risk of complications like tooth loss, heart disease, and stroke. To address these challenges, strict blood sugar control is crucial, reducing the risk of periodontal disease and enhancing treatment outcomes. Regular dental checkups and cleanings aid in early detection and management, while aggressive periodontal treatment, including scaling, root planning, antibiotic therapy, and surgery, may be necessary in some cases. [37,38]. Emphasizing good oral hygiene practices, such as brushing, flossing, and using fluoride mouthwash, can contribute to better periodontal health. Additionally, adopting a healthy diet, engaging in regular exercise, and quitting smoking can further safeguard periodontal health in individuals with diabetes.
Incorporating these treatment considerations and preventive measures can help those with hyperglycemia reduce their risk of periodontal disease and improve their overall oral and systemic well-being [39-42].
Dental Caries (Tooth Decay)
The association between diabetes and dental caries is complex and multifaceted. Dental caries, commonly known as cavities or tooth decay, primarily result from the demineralization of tooth enamel by acids produced by bacteria in the mouth. Figure 2 and 3 shows early childhood caries and Rampant caries affecting aesthetics [43].
Uncontrolled hyperglycemia may increase the risk of dental caries due to prolonged high blood glucose fostering oral microbial growth [44,45]. High glucose levels in saliva promote acid-producing bacteria, causing tooth enamel damage and cavities. Additionally, diabetes can compromise the immune response, reducing the body's ability to combat oral infections and contributing to an increased susceptibility to dental caries. This connection highlights the need for oral care in people with diabetes. Further research is needed to understand and address this issue [7,46].
Recent studies have delved into the connection between hyperglycemia and dental caries, with the goal of establishing evidence-based risk assessment protocols tailored to this particular group [47]. Researchers aim to pinpoint the factors contributing to heightened susceptibility to dental caries in individuals with elevated blood glucose levels through thorough oral health assessments, including an assessment of glycemic control, dietary habits, and oral hygiene practices [48]. The findings from such studies are instrumental in developing targeted preventive strategies and optimizing oral health management in hyperglycemic individuals, thereby potentially reducing the incidence and impact of dental caries in this at-risk group [49].
Preventing dental caries due to hyperglycemia is crucial for those with high blood sugar levels. Research aims to find effective interventions for this increased risk [50]. The relationship between antidiabetic medications and dental caries is a topic of interest in oral health research. Some studies have suggested a potential link between certain antidiabetic drugs and an increased risk of dental caries, while others have explored the protective effects of specific medications. It's important to note that the impact of antidiabetic drugs on dental caries can vary depending on factors such as drug type, dosage, and individual patient characteristics. For instance, some research has indicated that medications like metformin, which is commonly used to treat type 2 diabetes, may have a neutral or potentially beneficial effect on dental health. Metformin is known to improve insulin sensitivity and reduce inflammation, which could indirectly contribute to better oral health outcomes. On the other hand, there have been concerns raised about the potential side effects of certain antidiabetic medications, particularly those that contain sugars or sugar alcohols, as they may contribute to tooth decay if proper oral hygiene is not maintained. Overall, the relationship between antidiabetic medications and dental caries is a complex and evolving area of research. Individuals with diabetes are encouraged to work closely with their healthcare providers, including dentists, to manage their condition effectively and maintain good oral health through a combination of medication management, dietary choices, and oral hygiene practices. Comprehensive approaches aim to better understand the link between hyperglycemia and dental caries, improving preventive strategies and oral health outcomes [51].
Oral Thrush (Candidiasis)
Oral thrush, a fungal infection known as candidiasis, has a significant connection with diabetes due to its impact on the immune system and the oral environment. Research in oral health has revealed that hyperglycemia provides an ideal environment for Candida species, the causative agents of oral thrush, to flourish in the oral cavity [52,53]. Figure 4 illustrates the clinical presentation of this condition [54].
The surplus glucose in saliva and tissues serves as a rich nutrient source for these opportunistic fungi, leading to their overgrowth and colonization on the oral mucosal surfaces. Researchers are actively investigating the link between hyperglycemia and Candida colonization to develop preventive strategies [55]. Early detection and treatment of oral thrush, coupled with effective blood sugar control, are critical for oral health in individuals with hyperglycemia [56,57].
Excess glucose creates an ideal environment for Candida albicans to multiply within the body [58,59]. Additionally, hyperglycemia weakens the immune system's ability to control fungal growth, increasing the risk of candidiasis, especially in individuals with diabetes. Understanding this connection is vital for developing effective strategies to manage candidiasis in hyperglycemic patients [60,61]. Research extensively examines Candida albicans in hyperglycemia. Candidiasis can vary in its manifestations [62,63]. Diagnosis involves clinical assessment and lab tests. Timely diagnosis is vital to start the right treatment and manage blood sugar levels, reducing health risks in hyperglycemic individuals [64,65].
Various treatment options and control measures are explored concerning Candida albicans infections in the context of hyperglycemia. Effective management of candidiasis in hyperglycemic individuals involves both antifungal therapy and glycemic control. Antifungal medications, such as fluconazole, itraconazole, or topical agents, are commonly used to treat Candida infections. However, the recurrence of candidiasis is often associated with uncontrolled hyperglycemia. Therefore, optimizing glycemic levels through lifestyle modifications, insulin therapy, or other antidiabetic medications is crucial in preventing and managing candidiasis. Additionally, proper oral hygiene, including regular dental visits and maintenance of a balanced diet, plays a vital role in reducing the risk of Candida albicans infections in individuals with hyperglycemia.
While the impact of antidiabetic medications on oral thrush can vary, there have been concerns raised about certain medications, such as inhaled corticosteroids, potentially increasing the risk of oral thrush due to their immunosuppressive effects in the oral cavity.
In nutshell, to mitigate the risk of oral thrush, individuals with hyperglycemia, particularly those with diabetes, should prioritize good oral hygiene practices, including regular brushing and flossing. Additionally, it's essential to maintain optimal glycemic control to reduce the elevated blood sugar levels that can contribute to the growth of Candida in the oral cavity. Collaboration between healthcare providers, including dentists and endocrinologists, is crucial for managing hyperglycemia effectively and addressing any associated oral health concerns.
Dry Mouth (Xerostomia)
Hyperglycemia and dry mouth, clinically known as xerostomia, share a notable association, with elevated blood glucose levels playing a pivotal role in its development. Elevated blood glucose levels can reduce saliva production and alter its composition, leading to xerostomia in people with diabetes or poorly controlled blood sugar [66,67]. Xerostomia significantly impacts oral health as saliva helps maintain oral hygiene and guards against dental issues and infections. Figure 5 illustrates the clinical presentation of xerostomia [68].
Studies explore the causes of xerostomia in hyperglycemia, highlighting the importance of glycemic control, lifestyle changes, and oral care to alleviate dry mouth and prevent oral health problems [69,70]. Research also investigates salivary dysfunction in hyperglycemia. Elevated blood sugar can harm salivary glands, reducing saliva production and altering its composition. This dysfunction can lead to oral complications like dental caries, infections, and slow wound healing [71,72]. Understanding this connection informs targeted interventions and preventive measures to address salivary dysfunction and promote oral health in hyperglycemic individuals [73,74]. Moreover, research delves into the symptoms and oral health impact of salivary dysfunction in hyperglycemia. It can manifest as dry mouth, altered saliva consistency, and reduced saliva flow, affecting oral functions like eating, speaking, and taste perception. Reduced saliva properties may increase the risk of dental problems and infections [26,30]. Recognizing the profound impact of salivary dysfunction helps develop comprehensive management strategies, emphasizing glycemic control and specific oral care to improve oral health in hyperglycemic individuals [42,75,76].
Management strategies for xerostomia in hyperglycemia involve relieving symptoms and addressing the root cause. They include promoting hydration, using saliva substitutes, and sugar-free gum to stimulate saliva production. Proper oral hygiene and fluoride products help prevent dental issues. Managing hyperglycemia through lifestyle changes or medications is crucial for restoring salivary gland function [77,78]. Collaboration between dental professionals and healthcare providers is essential to create personalized management plans that ease xerostomia and enhance oral health in hyperglycemic individuals [79,80].
Burning Mouth Syndrome
Research has explored the link between Burning Mouth Syndrome (BMS) and hyperglycemia. BMS is characterized by a persistent burning sensation in the mouth, affecting areas like the tongue, lips, and oral mucosa. Hyperglycemia, especially in diabetes, may contribute to the development or worsening of BMS [81,82]. The exact mechanisms connecting hyperglycemia to BMS are not fully understood but likely involve altered nerve function, vascular changes, and inflammation. Recognizing this potential association is crucial in clinical practice for early diagnosis, appropriate management, and optimizing glycemic control to alleviate distressing symptoms. Further research is needed to better understand the condition's underlying causes and develop targeted treatments [83].
The literature highlights the clinical features and diagnostic challenges of hyperglycemia-induced Burning Mouth Syndrome (BMS). BMS presents as a distinctive burning mouth sensation, often accompanied by altered taste and dry mouth. In individuals with hyperglycemia, diagnosing BMS can be challenging due to overlapping symptoms with other oral complications of diabetes. Additionally, the multifaceted nature of BMS and the absence of specific biomarkers make definitive diagnosis difficult. Healthcare professionals must be vigilant in recognizing the potential link between hyperglycemia and BMS, considering patient history, conducting thorough clinical evaluations, and ruling out other possible causes to reach an accurate diagnosis. A better understanding of BMS's clinical presentation and diagnostic intricacies induced by hyperglycemia is crucial for timely intervention and improving affected individuals' quality of life. Further research is necessary to develop more precise diagnostic criteria and clarify the underlying mechanisms for targeted therapeutic strategies.
The literature also explores various approaches to managing Burning Mouth Syndrome (BMS) related to hyperglycemia. Treating BMS induced by hyperglycemia requires a comprehensive strategy addressing both the underlying hyperglycemia and BMS symptoms. Achieving optimal glycemic control through lifestyle adjustments, antidiabetic medications, or insulin therapy is crucial for effective management [26,74]. Symptomatic relief for BMS may involve using topical agents, saliva substitutes, and pain-relieving medications. Additionally, psychological support and counselling can be beneficial, considering BMS's significant impact on the patient's quality of life [30]. A multidisciplinary approach, involving collaboration between dental professionals, endocrinologists, and other healthcare providers, is vital in crafting personalized management plans that account for the complex nature of BMS induced by hyperglycemia. Further research is required to assess the effectiveness of various treatment methods and enhance outcomes for individuals affected by this condition [42,76].
Oral Infections and Immune Function
The relationship between oral infections and immune function is a complex area of research. The oral cavity is a primary entry point for numerous microorganisms, making it susceptible to infections that can significantly impact overall health. The immune system plays a vital role in defending against these pathogens while maintaining a delicate balance between protection and tolerance to the resident oral microbiota [77,78].
Dysregulation of immune function can increase susceptibility to oral infections like dental caries, periodontal disease, and oral thrush. Furthermore, oral infections can influence systemic immune responses, contributing to the development or worsening of various systemic conditions. Understanding the bidirectional interactions between oral infections and immune function is crucial for developing effective preventive and therapeutic strategies to promote oral health and overall well-being [83].
One aspect of this relationship involves exploring the impact of hyperglycemia on the immune response. Elevated blood glucose levels, as seen in conditions like diabetes, can lead to significant alterations in immune function, affecting both innate and adaptive immunity. Hyperglycemia can impair the activity of various immune cells, such as neutrophils, macrophages, and T cells, compromising their ability to combat infections and regulate inflammation [81]. Additionally, it may promote chronic low-grade inflammation, contributing to the development of immune-related disorders and complications. Understanding the detrimental effects of hyperglycemia on the immune response is crucial in addressing the increased susceptibility to infections and immune-related conditions in individuals with poorly controlled blood glucose levels, informing strategies to optimize glycemic control and enhance immune function [80].
Another facet involves investigating common oral infections and complications induced by hyperglycemia, especially in individuals with diabetes. Elevated blood glucose levels create a favorable environment for various oral pathogens, increasing the risk of dental caries, periodontal disease, and oral thrush [78,79]. Hyperglycemia can compromise the immune response, impairing the body's ability to defend against these infections. Moreover, poor glycemic control can exacerbate the severity of oral infections and delay wound healing, leading to more challenging treatment outcomes. Recognizing the link between hyperglycemia and oral infections is essential in promoting comprehensive oral health care and implementing preventive measures to reduce the occurrence and progression of oral complications in affected individuals [42,77].
To address these challenges, research delves into strategies for preventing and managing oral infections in hyperglycemic patients. Maintaining optimal glycemic control is fundamental in reducing the risk of oral infections since elevated blood glucose levels create a favorable environment for pathogenic microorganisms. Regular dental check-ups, meticulous oral hygiene practices, and a balanced diet low in sugary and acidic foods are crucial preventive measures [26,30]. Additionally, the use of fluoride products and antimicrobial mouth rinses can help minimize the risk of dental caries and periodontal disease [73].
Collaborative Approach in Patient Care: Diabetologists vs Dentists
In the management of diabetes-related oral complications, the collaboration between diabetologists and dentists plays a pivotal role in ensuring comprehensive care for patients. Recognizing the intricate connection between diabetes and oral health, healthcare professionals have increasingly realized that addressing these issues requires a multidisciplinary approach that combines the expertise of diabetologists and dentists. This collaborative model is essential for optimizing diabetes management, monitoring oral health closely, and implementing targeted interventions to address and prevent complications effectively. Ongoing research explores innovative strategies, including targeted therapies, to manage oral health complications in hyperglycemia.
One of the critical aspects of this collaborative approach is the early identification of oral manifestations of diabetes. Diabetologists and dentists work together to educate patients about the bidirectional relationship between diabetes and oral health. By raising awareness about the potential risks, such as periodontal disease, dental caries, and oral thrush, patients are empowered to take proactive measures to safeguard their oral health. Regular dental check-ups, meticulous oral hygiene practices, and glycemic control are emphasized as essential components of diabetes care.
When it comes to treatment, diabetologists and dentists collaborate to develop personalized management plans for patients dealing with both diabetes and oral health issues. Patients with uncontrolled diabetes may require adjustments to their insulin or hypoglycemic medications in response to dental procedures, orofacial infections, and surgery. Dentists consult with the patient's physicians to ensure that any modifications to medical therapy are carried out safely and effectively.
Drug interactions and considerations are also a focal point of this collaboration. Dentists are cautious about using large amounts of epinephrine, as it can antagonize the effects of insulin and lead to hyperglycemia. Similarly, the administration of systemic corticosteroids, even in small amounts, can severely worsen glycemic control. Patients taking oral hypoglycemic agents who are placed on steroid therapy may require short-term insulin therapy to maintain glycemic control. Diabetologists and dentists work in tandem to monitor and manage these interactions, ensuring that patients receive the most appropriate care.
In addition to treatment considerations, diabetologists and dentists collaborate on the regular monitoring of glycemic control. Both healthcare providers must have the facilities and resources to assess and track blood sugar levels effectively. This enables them to make informed decisions about treatment adjustments, especially in cases where dental procedures or infections may impact glycemic control.
Patients with diabetes, particularly those with a history of poor glycemic control and oral infections, require more frequent recall visits and fastidious attention to acute oral infections. Diabetologists and dentists coordinate these recall visits to ensure that patients receive consistent and comprehensive care. By doing so, they can effectively manage hyperglycemia-induced oral complications and improve the overall health and well-being of their patients.
In conclusion, a collaborative approach in patient care, involving diabetologists and dentists, is essential in addressing the complex interplay between diabetes and oral health. This collaboration focuses on early identification, personalized treatment, and careful monitoring to optimize glycemic control and prevent complications. By working together, diabetologists and dentists can provide the best possible care for patients dealing with both diabetes and oral health concerns, ultimately enhancing their quality of life and overall well-being.
Summary
Understanding the intricate two-way relationship between diabetes and its oral manifestations is of paramount importance for healthcare professionals tasked with treating either condition. In the realm of diabetes care, providing safe and effective oral medical care for patients with diabetes necessitates a deep understanding of the disease itself and a familiarity with its oral manifestations. Numerous studies have unequivocally demonstrated a significant association between diabetes and oral diseases, highlighting that microvascular and macrovascular complications of diabetes are notably higher among individuals with oral health issues. The implications are clear: the management of one condition profoundly impacts the other. One particularly significant finding is that diabetes significantly elevates the risk of developing oral ulcers. This heightened risk is attributed to chronic hyperglycemia, oxidative stress, and decreased blood flow to oral tissues, all mechanisms by which diabetes can lead to the formation of oral ulcers. However, there is a ray of hope – effective glycemic control emerges as a powerful preventive measure against the development of oral ulcers in individuals with diabetes. The overarching goal of therapy in this context is multifaceted. It seeks to promote oral health in patients with diabetes, aid in the early detection and diagnosis of diabetes in dental patients undergoing routine stomatological care, and ultimately enhance the quality of life for individuals afflicted with this incurable disease. This holistic approach underscores the integral role of healthcare providers in delivering comprehensive care and addressing the complex interplay between diabetes and its oral manifestations. Despite the compelling evidence underscoring the relationship between diabetes and oral health, knowledge of oral comorbidity among people with diabetes remains generally poor. This knowledge gap underscores the critical need for targeted health education and health promotion initiatives aimed at improving the oral health of diabetic patients. By raising awareness, disseminating information, and fostering collaboration between diabetologists and dentists, we can empower patients, reduce the burden of oral complications, and ultimately enhance the overall well-being of those dealing with this challenging disease. This comprehensive review has provided a detailed exploration of oral complications induced by hyperglycemia in individuals with diabetes, covering their causes, symptoms, and management. By continuously advancing our knowledge and implementing evidence-based approaches, we can work towards reducing the burden of oral complications induced by hyperglycemia in diabetic individuals, ultimately improving both oral and systemic health outcomes.
- Baima G, Romandini M, Citterio F, Romano F, Aimetti M (2022) Periodontitis and Accelerated Biological Aging: A Geroscience Approach. Journal of dental research 101: 125-32.
- Barros SP, Offenbacher S (2014) Modifiable risk factors in periodontal disease: epigenetic regulation of gene expression in the inflammatory response. Periodontology 64: 95-110.
- Bascones-Martínez A, Arias-Herrera S, Criado-Cámara E, Bascones-Ilundáin J, Bascones-Ilundain C (2012) Periodontal disease and diabetes. Advances in experimental medicine and biology 771: 76-87.
- Bascones-Martínez A, Munoz-Corcuera M, Bascones-Ilundain J (2015) [Diabetes and periodontitis: A bidirectional relationship]. Medicina clinica 145: 31-5.
- Bhattarai G, So HS, Kieu TTT, Kook SH, Lee JC, Jeon YM (2021) Astaxanthin Inhibits Diabetes-Triggered Periodontal Destruction, Ameliorates Oxidative Complications in STZ-Injected Mice, and Recovers Nrf2-Dependent Antioxidant System. Nutrients 13.
- Blasco-Baque V, Garidou L, Pomié C, et al. (2017) Periodontitis induced by Porphyromonas gingivalis drives periodontal microbiota dysbiosis and insulin resistance via an impaired adaptive immune response. Gut 66: 872-85.
- Borgnakke WS, Genco RJ, Eke PI, Taylor GW (2018) Oral Health and Diabetes. Diabetes in America. Cowie CC, Casagrande SS, Menke A, et al. (eds): National Institute of Diabetes and Digestive and Kidney Diseases (US), Bethesda (MD) of interest.
- Casillas Santana MA, Arreguín Cano JA, Dib Kanán A, et al. (2021) Should We Be Concerned about the Association of Diabetes Mellitus and Periodontal Disease in the Risk of Infection by SARS-CoV-2? A Systematic Review and Hypothesis. Medicina (Kaunas, Lithuania) 57.
- Chang JF, Yeh JC, Chiu YL, Liou JC, Hsiung JR, Tung TH (2017) Periodontal Pocket Depth, Hyperglycemia, and Progression of Chronic Kidney Disease: A Population-Based Longitudinal Study. The American journal of medicine 130: 61-9.
- Chapple ILC, Mealey BL, Van Dyke TE, et al. (2018) Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. Journal of periodontology 89: 74-84.
- Chapple ILC, Mealey BL, Van Dyke TE, et al. (2018) Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. Journal of clinical periodontology 45: 68-77.
- Chiu SY, Lai H, Yen AM, Fann JC, Chen LS, Chen HH (2015) Temporal sequence of the bidirectional relationship between hyperglycemia and periodontal disease: a community-based study of 5,885 Taiwanese aged 35-44 years (KCIS No. 32). Acta diabetologica 52: 123-31.
- de Oliveira P, Bonfante EA, Bergamo ETP, et al. (2020) Obesity/Metabolic Syndrome and Diabetes Mellitus on Peri-implantitis. Trends in endocrinology and metabolism: TEM 31: 596-610.
- Deshpande K, Jain A, Sharma R, Prashar S, Jain R (2010) Diabetes and periodontitis. Journal of Indian Society of Periodontology 14: 207-12.
- Gharamti A, Kanafani ZA (2018) Vascular Graft Infections: An update. Infectious disease clinics of North America 32: 789-809.
- Gomes SV, Rodrigues V, Nunes-Dos-Santos DL, Pereira ALA, Peres MA (2022) The relationship between periodontal status and hyperglycemia after kidney transplantation. Clinical oral investigations 26: 397-406.
- Graves DT, Ding Z, Yang Y (2020) The impact of diabetes on periodontal diseases. Periodontology 82: 214-24.
- Grossi SG, Genco RJ (1998) Periodontal disease and diabetes mellitus: a two-way relationship. Annals of periodontology 3: 51-61.
- Kiryowa HM, Munabi IG, Buwembo W, Rwenyonyi CM, Kaddumukasa M, Sabakaki EM (2022) Prevalence and factors associated with periodontal disease in patients with diabetes mellitus attending Kiruddu National Referral Hospital, Uganda. The Pan African medical journal 43: 202.
- Ko KI, Sculean A, Graves DT (2021) Diabetic wound healing in soft and hard oral tissues. Translational research: the journal of laboratory and clinical medicine 236: 72-86.
- Kocher T, König J, Borgnakke WS, Pink C, Meisel P (2018) Periodontal complications of hyperglycemia/diabetes mellitus: Epidemiologic complexity and clinical challenge. Periodontology 78: 59-97.
- Lalla E, Papapanou PN (2011) Diabetes mellitus and periodontitis: a tale of two common interrelated diseases. Nature reviews Endocrinology 7: 738-48.
- Lamster IB, Pagan M (2017) Periodontal disease and the metabolic syndrome. International dental journal 67: 67-77.
- Mathew JE, Jacob JJ, Kalra S (2021) Periodontitis management in diabetes care. JPMA The Journal of the Pakistan Medical Association 71: 2097-9.
- Matsha TE, Prince Y, Davids S, et al. (2020) Oral Microbiome Signatures in Diabetes Mellitus and Periodontal Disease. Journal of dental research 99: 658-65.
- Mauri-Obradors E, Estrugo-Devesa A, Jané-Salas E, Viñas M, López-López J (2017) Oral manifestations of Diabetes Mellitus. A systematic review. Medicina oral, patologia oral y cirugia bucal 22: 586-94.
- Monje A, Catena A, Borgnakke WS (2017) Association between diabetes mellitus/hyperglycaemia and peri-implant diseases: Systematic review and meta-analysis. Journal of clinical periodontology 44: 636-48.
- Nakahara Y, Ozaki K, Matsuura T (2017) Long-term Hyperglycemia Naturally Induces Dental Caries but Not Periodontal Disease in Type 1 and Type 2 Diabetic Rodents. Diabetes 66: 2868-74.
- Nascimento GG, Leite FRM, Vestergaard P, Scheutz F, López R (2018) Does diabetes increase the risk of periodon titis? A systematic review and meta-regression analysis of longitudinal prospective studies. Acta diabetologica 55: 653-67.
- Negrini TC, Carlos IZ, Duque C, Caiaffa KS, Arthur RA (2021) Interplay Among the Oral Microbiome, Oral Cavity Conditions, the Host Immune Response, Diabetes Mellitus, and Its Associated-Risk Factors-An Overview. Frontiers in oral health 2: 697428.
- Nibali L, Gkranias N, Mainas G, Di Pino A (2022) Periodontitis and implant complications in diabetes. Periodontology 90: 88-105.
- Nishimura F, Takahashi K, Kurihara M, Takashiba S, Murayama Y (1998) Periodontal disease as a complication of diabetes mellitus. Annals of periodontology 3: 20-9.
- Oberti L, Gabrione F, Nardone M, Di Girolamo M (2019) Two-way relationship between diabetes and periodontal disease: a reality or a paradigm? Journal of biological regulators and homeostatic agents 33: 153-9.
- Silva MF, Barbosa KG, Pereira JV, Bento PM, Godoy GP, Gomes DQ (2015) Prevalence of oral mucosal lesions among patients with diabetes mellitus types 1 and 2. Anais brasileiros de dermatologia 90: 49-53.
- Pedroso JF, Lotfollahi Z, Albattarni G, et al. (2019) Influence of Periodontal Disease on cardiovascular markers in Diabetes Mellitus patients. Scientific reports 9: 16138.
- Philips KH, Zhang S, Moss K, Ciarrocca K, Beck JD (2021) Periodontal disease, undiagnosed diabetes, and body mass index: Implications for diabetes screening by dentists. Journal of the American Dental Association (1939) 152: 25-35.
- Polak D, Sanui T, Nishimura F, Shapira L (2020) Diabetes as a risk factor for periodontal disease-plausible mechanisms. Periodontology 83: 46-58.
- Polak D, Shapira L (2018) An update on the evidence for pathogenic mechanisms that may link periodontitis and diabetes. Journal of clinical periodontology 45: 150-66.
- Preshaw PM, Alba AL, Herrera D, et al. (2012) Periodontitis and diabetes: a two-way relationship. Diabetologia 55: 21-31.
- Qi J, Zihang Z, Zhang J, et al. (2020) Periodontal Antibodies and All-Cause and Cardiovascular Disease Mortality. Journal of dental research 99: 51-9.
- Qin H, Li G, Xu X, et al. (2022) The role of oral microbiome in periodontitis under diabetes mellitus. Journal of oral microbiology 14: 2078031.
- Rohani B (2019) Oral manifestations in patients with diabetes mellitus. World journal of diabetes 10: 485-9.
- Bhayat A, Madiba T (2017) Is dental caries contagious? South African Dental Journal 72: 302-4.
- Ahmad R, Haque M (2021) Oral Health Messiers: Diabetes Mellitus Relevance. Diabetes, metabolic syndrome and obesity : targets and therapy 14: 3001-15.
- Andrade L, Lee KM, Sylvetsky AC, Kirkpatrick SI (2021) Low-calorie sweeteners and human health: a rapid review of systematic reviews. Nutrition reviews 79: 1145-64.
- Cao X, Wang D, Zhou J, Yuan H, Chen Z (2017) Relationship between dental caries and metabolic syndrome among 13 998 middle-aged urban Chinese. Journal of diabetes 9: 378-85.
- de Campaigno EP, Kebir I, Montastruc JL, et al. (2017) Drug-Induced Dental Caries: A Disproportionality Analysis Using Data from VigiBase. Drug safety 40: 1249-58.
- Grisi DC, Vieira IV, de Almeida Lima AK, et al. (2022) The Complex Interrelationship between Diabetes Mellitus, Oral Diseases and General Health. Current diabetes reviews 18: e220321192408.
- Janket SJ, Benwait J, Isaac P, Ackerson LK, Meurman JH (2019) Oral and Systemic Effects of Xylitol Consumption. Caries research 53: 491-501.
- Latti BR, Kalburge JV, Birajdar SB, Latti RG (2018) Evaluation of relationship between dental caries, diabetes mellitus and oral microbiota in diabetics. Journal of oral and maxillofacial pathology: JOMF 22: 282.
- Nakahara Y, Sano T, Kodama Y, Ozaki K, Matsuura T (2012) Alloxan-induced hyperglycemia causes rapid-onset and progressive dental caries and periodontitis in F344 rats.Histology and histopathology 27: 1297-306.
- Verspeelt J, Marynissen G, Gupta AK, De Doncker P (1999) Safety of itraconazole in diabetic patients. Dermatology (Basel, Switzerland) 198: 382-84.
- Vitkov L, Weitgasser R, Hannig M, Fuchs K, Krautgartner WD (2003) Candida-induced stomatopyrosis and its relation to diabetes mellitus. Journal of oral pathology & medicine: official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology 32: 46-50.
- Fusco A, Contaldo M, Savio V, et al. (2003) An Unconventional Oral Candidiasis in an Immunocompetent Patient. Journal of Fungi 9: 295.
- Vegas-Revenga N, Martín-Varillas JL, Calvo-Río V, et al. (2022) Intravenous methylprednisolone induces rapid improvement in non-infectious uveitis: a multicentre study of 112 patients. Clinical and experimental rheumatology. 2022, 40:142-149.
- Takasawa H, Takahashi Y, Abe M, et al. (2007) An elderly case of type 2 diabetes which developed in association with oral and esophageal candidiasis. Internal medicine (Tokyo, Japan) 46: 387-90.
- Unnikrishnan AG, Kalra S, Purandare V, Vasnawala H (2018) Genital Infections with Sodium Glucose Cotransporter-2 Inhibitors: Occurrence and Management in Patients with Type 2 Diabetes Mellitus. Indian journal of endocrinology and metabolism 22: 837-42.
- Roncoroni AJ, Abbate E, Figueroa Casas JC, et al. (1993) [Standards established by consensus for the treatment of bronchial asthma and its exacerbations]. Medicina 53: 249-59.
- Sato T, Kishi M, Suda M, et al. (2017) Prevalence of Candida albicans and non-albicans on the tongue dorsa of elderly people living in a post-disaster area: a cross-sectional survey. BMC oral health 17: 51.
- Paterson AJ, Lamey PJ, Lewis MA, Nolan A, Rademaker M (1993) Pemphigus vulgaris precipitated by glibenclamide therapy. Journal of oral pathology & medicine: official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology 22: 92-5.
- Ringdahl EN (2000) Treatment of recurrent vulvovaginal candidiasis. American family physician 61: 3306-12
- Negrato CA, Tarzia O (2010) Buccal alterations in diabetes mellitus. Diabetology & metabolic syndrome 2: 3.
- Nyirjesy P, Sobel JD (2013) Genital mycotic infections in patients with diabetes. Postgraduate medicine 125: 33-46.
- McComsey GA, Whalen CC, Mawhorter SD, et al. (2001) Placebo-controlled trial of prednisone in advanced HIV-1 infection. AIDS (London, England) 15: 321-7.
- Nakajima A, Doki K, Homma M, et al. (2009) [Investigation of glucocorticoid-induced side effects in patients with autoimmune diseases]. Yakugaku zasshi : Journal of the Pharmaceutical Society of Japan 129: 445-50.
- Allushi B, Bagavant H, Papinska J, Deshmukh US (2019) Hyperglycemia and Salivary Gland Dysfunction in the Non-obese Diabetic Mouse: Caveats for Preclinical Studies in Sjögren's Syndrome. Scientific reports 9: 17969.
- Bensch L, Braem M, Van Acker K, Willems G (2003) Orthodontic treatment considerations in patients with diabetes mellitus. American journal of orthodontics and dentofacial orthopedics: official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics 123: 74-8.
- Chaithra M, Vasudev I, Kashyap R, et al. (2018) Diabetes Mellitus and Xerostomia: An Obnoxious Co-Occurrence 2456-86.
- Binder A, Maddison PJ, Skinner P, Kurtz A, Isenberg DA (1989) Sjögren's syndrome: association with type-1 diabetes mellitus. British journal of rheumatology 28: 518-20.
- Bissong M, Azodo CC, Agbor MA, Nkuo-Akenji T, Fon PN (2015) Oral health status of diabetes mellitus patients in Southwest Cameroon. Odonto-stomatologie tropicale = Tropical dental journal 38:49-57.
- Cheraskin E, Ringsdorf WM, Jr. (1974) Letter: Dry mouth and dysglycemia. Jama 229: 523.
- Cheraskin E, Ringsdorf WM, Jr., White WL, Jr. (1964) DRY MOUTH AND CARBOHYDRATE METABOLISM. Journal of the American Geriatrics Society 12: 337-44.
- Malicka B, Kaczmarek U, Skośkiewicz-Malinowska K (2014) Prevalence of xerostomia and the salivary flow rate in diabetic patients. Advances in clinical and experimental medicine: official organ Wroclaw Medical University 23: 225-33.
- Matsumoto N, Omagari D, Ushikoshi-Nakayama R, Yamazaki T, Inoue H, Saito I (2021) Hyperglycemia Induces Generation of Reactive Oxygen Species and Accelerates Apoptotic Cell Death in Salivary Gland Cells. Pathobiology: journal of immunopathology, molecular and cellular biology 88: 234-41.
- Paurobally N, Kruger E, Tennant M (2021) Awareness About the Oral and Systemic Complications of Diabetes Among a Cohort of Diabetic Patients of the Republic of Mauritius. International dental journal 71: 438-48.
- Rai K, Hegde AM, Kamath A, Shetty S (2011) Dental caries and salivary alterations in Type I Diabetes. The Journal of clinical pediatric dentistry 36: 181-4.
- Sanjeeta N, Sivapathasundharam B, Nandini DB (2022) Oral lesions and periodontal status in diabetics and non-diabetics: A hospital-based study. Journal of oral and maxillofacial pathology: JOMFP 26: 419.
- Starostina SV, Statsenko YA, Svistushkin VM (2022) [Optimization of an integrated approach to voice correction for endocrinopathies (analytical review)]. Problem yendokrinologi 68: 48-55.
- Sundaram M, Manikandan S, Satheesh B, Srinivasan D, Jayapal D, Kumar D (2020) Comparative Evaluation of Xerostomia among Diabetic and Nondiabetic Subjects Wearing Complete Denture. Journal of pharmacy & bioallied sciences 12: 419-22.
- Tran SD, Kodama S, Lodde BM, et al. (2007) Reversal of Sjogren's-like syndrome in non-obese diabetic mice. Annals of the rheumatic diseases 66: 812-4.
- Vernillo AT (2001) Diabetes mellitus: Relevance to dental treatment. Oral surgery, oral medicine, oral pathology, oral radiology, and endodontics 91: 263-70.
- Yeh CK, Harris SE, Mohan S, et al. (2012) Hyperglycemia and xerostomia are key determinants of tooth decay in type 1 diabetic mice. Laboratory investigation; a journal of technical methods and pathology 92: 868-82.
- Zhang S, Li J, Nong X, et al. (2021) Artesunate Combined with Metformin Ameliorate on Diabetes-Induced Xerostomia by Mitigating Superior Salivatory Nucleus and Salivary Glands Injury in Type 2 Diabetic Rats via the PI3K/AKT Pathway. Frontiers in pharmacology 12: 774674.
FIGURE 1
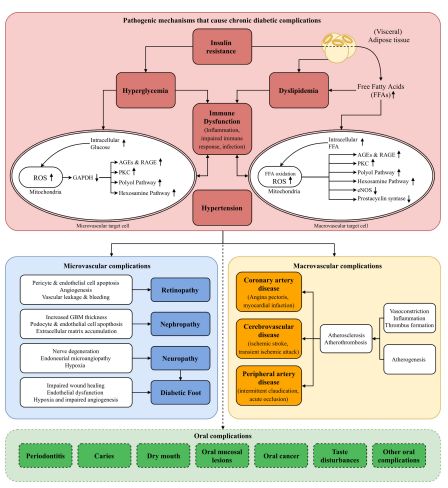
Figure 1: Schematic illustration of pathogenetic mechanisms that cause chronic diabetic complications
FIGURE 2

Figure 2 and 3: Early childhood caries and Rampant caries (We thank the authors for granting permission to use this figure)
FIGURE 4

Figure 4: Clinical presentation of Candidiasis
FIGURE 5
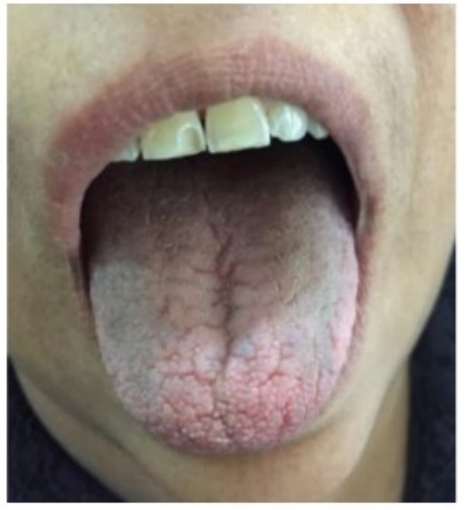
Figure 5: Clinical presentation of Xerostomia
Tables at a glance
Figures at a glance