Aesthetic Rehabilitation of Severe Dental Attrition: Exploring the Long-Term Prognosis of Metal-Ceramic and All-Ceramic Fixed Dental Prostheses
Received Date: April 20, 2024 Accepted Date: May 20, 2024 Published Date: May 23, 2024
doi: 10.17303/jdoh.2024.11.102
Citation: Mahdi Nourbakhsh, John R. Calamia, Nicholas J. Giannuzzi, Maria D. Madonna, Fred A. Puccio, et al. (2024) Aesthetic Rehabilitation of Severe Dental Attrition: Exploring the Long-Term Prognosis of Metal-Ceramic and All-Ceramic Fixed Dental Prostheses. J Dent Oral Health 11: 1-16
Abstract
When fabricating fixed dental prostheses (FDP) opposing natural dentition, the type of material and quality of the restoration are critical factors in ensuring proper occlusal function and harmony. Violating the natural biology of a patient’s dentition can cause catastrophic long-term effects both aesthetically and functionally. This case highlights the severe incisal wear observed in the maxillary central and lateral incisors of a 65-year-old male patient, attributable to an overcontoured, 6-unit porcelain-fused-to-metal (PFM) bridge spanning teeth 22-27. The objective was to address the patient's chief complaint while considering his complex medical history and oral health status. A literature review comparing PFM and all-ceramic bridges was conducted to determine the best material choice for achieving long-term success. While all-ceramic bridges offer improved aesthetics, they tend to exhibit higher rates of technical complications like chipping and fracture compared to PFM bridges. Based on the available evidence, PFM bridges were recommended for this patient due to their demonstrated longevity and durability. The treatment plan involved periodontal therapy, tooth extractions, and prosthetic rehabilitation with full coverage crowns and veneers. Risk assessments were carefully considered given the patient's medical conditions to minimize potential adverse events during treatment. Emphasis was placed on patient education and maintenance protocols to optimize long-term outcomes. Assessment of the outcomes of care and prognosis revealed positive results with comprehensive reduction of risk factors and successful restoration of aesthetics and function. The patient's chief complaint was effectively addressed, and the prognosis of the delivered treatment is optimistic. Ongoing collaboration with medical providers and continued patient education will be essential to ensure sustained oral hygiene and overall health.
Keywords: All-Ceramic; Metal-Ceramic; Porcelain-Fused-to-Metal; Biological Complications; Fixed Dental Prostheses; Fixed Partial Denture; Success; Survival; Long-Term Prognosis
Introduction
The objective of this case report is to address the restorative treatment needs of a 65-yearold male patient presenting to the clinic with chief complaint “My top front teeth are all worn away.” He has a large PFM bridge spanning teeth 22-27 and exhibits neither a diminished vertical dimension of occlusion nor excessive wear facets relative to biological age in the posterior dentition. Clinical evaluation reveals the excessive height of the anterior teeth creates an uneven occlusal plane in relation to the posterior dentition, and in the facial aspect, the 6-unit bridge exhibits an over-- contoured emergence profile. In conjunction with the patient's parafunctional clenching habit, it is hypothesized that the attrition of the maxillary incisors is predominantly a consequence of the suboptimal design and fabrication of the original PFM bridge.
In order to address the patient’s chief complaint, we must first perform a comprehensive examination, eliminate any underlying disease processes, establish a healthy periodontium, and determine the optimal choice of material for the final prosthesis. Therefore, a literature review was conducted to compare the long-term prognosis and durability of porcelain-fused-to-metal and all-ceramic bridges. An interdisciplinary approach was taken in formulating a comprehensive treatment plan with emphasis being placed on minimizing potential adverse events given the patient's medical conditions. Overall, this case underscores the significance of evidence-based decision-making in restorative dentistry, particularly in managing complex cases with a focus on optimal outcomes and patient satisfaction.
Literature Review
Clinical Question: In patients undergoing restorative treatment with fixed partial dentures, would a porcelain- fused-to-metal or an all-ceramic bridge lead to better long-term prognosis?
Population: Patients with fixed partial dentures
Intervention: Patients with a porcelain-fused-to-metal FPD
Comparison: Patients with an all-ceramic FPD
Outcome: Long term prognosis of the FPD
The literature search was done with PubMed, MEDLINE, and the Cochrane Database using various combinations of the keywords above which yielded 148 titles. This list was further narrowed down to 19 results by filtering for date of publication and systematic reviews. Reviewing the abstracts led to the final choice of the three following systematic reviews which were chosen for appraisal based off clinical relevance
Article 1: Survival of Zirconia- and Metal-Supported Fixed Dental Prostheses: A Systematic Review
The purpose of this paper was to compare the incidence of veneer chipping and core fractures of PFM fixed dental prosthesis as compared to zirconia FDPs. They conducted their search in March 2009 and looked at factors such as the type of veneering material used, the number of units in the FDP, and the location in the mouth. Inclusion criteria for the studies included in the systematic review were prospective clinical trials of at least two years that reported on dropouts, replacements, and technical failures of the FDPs such as framework fracture, chipping, or debonding. Articles that reported on biological failures such as periodontal disease and endodontic treatment were excluded. A grading scale of 1 to 3 was established for the severity of veneer chipping based on whether the chip could be polished off (grade 1), fixed with composite (grade 2), or it had to be replaced entirely (grade 3). The authors hypothesized that zirconia based FDPs chip more frequently than metal based FDPs, the frequency of chipping is higher for FDPs spanning more than three crowns or those with unsupported cusps, and that the frequency of chipping is not dependent upon the veneer material.
Fifteen studies were included in the systematic review with baseline data for 627 zirconia FDPs and 134 PFM FDPs, the majority of which were 3 units long. The mean age of subjects was based on 10 studies was 48.3 ± 5.8 years and an average 56% of the study population in 11 studies were women. There was a low dropout rate of approximately 5% in both the zirconia and PFM groups and the mean observation period was 3.3 ± 1 years for zirconia FDPs and 2.9 ± 0.3 years for PFM FDPs. However, the studies that had observation periods of 4 and 5 years only reported on zirconia FDPs.
The results showed less than 1% of the zirconia FDPs reported a core fracture whereas none of the PFM cores fractured. With regards to veneer chipping, they found that among both PFM and zirconia FDPs the majority of fractures were grade 1 and 2. However, the frequency of chipping was significantly higher for zirconia FDPs (P < .001) as compared to PFM. When including all types of chipping over an average 3-year observation period, the incidence of veneer chipping of zirconia FDPs was 90% as compared to 97% for PFM FDPs. This difference was statistically significant for all grades of chipping (P = .001), as well as for grade 3 chipping (P = .02) when the survival rates were adjusted for the study effect.
Of the four hypotheses introduced by the authors, only the first one (zirconia based FDPs chip more frequently than metal based FDPs) could be confirmed. Unfortunately, all of the studies that reported on PFM FDPs failed to meet the inclusion criteria. They fell short by not reporting dropouts, not specifying FDP type, not having systematic recalls, and not reporting detailed descriptions of technical failures. However, since the trials were conducted in the ‘70s and ‘80s we can attribute this to the low-quality level of clinical trials at that time. In contrast, the studies on zirconia FDPs included in the systematic review were of a much higher standard. Other limitations of the studies include discrepancies in chipping grades and high variability among the frequency of chipping reported. Also, some of the studies included lacked a control group, subject randomization, sample size assessment, and details on the FDPs which could all introduce confounding factors. This review concluded that since newly refined processing procedures of zirconia have started yielding improved results, new clinical studies should be done to confirm whether or not the chipping frequency of all ceramic FDPs can compare to that of PFM.
Article 2: A systematic Review of the Survival and Complication Rates of All-ceramic and Metal– Ceramic Reconstructions After an Observation Period of at least 3 years. Part II: Fixed Dental Prostheses
The objectives of this review were to measure long term survival rates and incidence of technical and biological complications of all-ceramic FDPs for a minimum 3-year observation period, and to compare those results with the gold standard metal-ceramic reconstructions. An extensive search was done using two databases over multiple languages with additional manual searches of related article bibliographies to find randomized control trials comparing all-ceramic and metal-ceramic FDP reconstructions. No randomized control trials were found so instead the included articles were selected based on the following criteria: prospective or retrospective cohort studies with an average 3 year or more follow-up time which reported details on the characteristics of the reconstructions. Studies with no detailed descriptions of the reconstruction or failures and no reporting of clinical recalls such those using follow-up data from patient records, interviews, and questionnaires were excluded.
Three independent reviewers selected 3,473 titles which were narrowed down to 39 full text articles, 9 of which (8 prospective, 1 retrospective) were ultimately selected for this review to report on all-ceramic FDPs. Two studies reported on glass-ceramic FDPs, four studies reported on glass-infiltrated ceramic FDPs (zirconia and InCeram Alumina), and the last three reported on FDPs made with zirconia frameworks. All the data on PFM FDP survival and complication rates were taken from a different systematic review (Pjetursson et al. 2007). 4 Patient age from all the studies ranged from 13 to 82 years old, and only 11 of the studies reported loss to follow up data which ranged from 0% to 40%.
The authors defined survival as “the FDP remaining in situ at the examination visit with or without modifications.” Technical complications encompassed framework fracture, veneer chipping, marginal gaps/discoloration, and loss of retention. Biological complications included caries, abutment tooth fracture, loss of pulpal vitality, and periodontal disease. The studies on all ceramic FDPs provided data for 343 total FDPs (9.6% lost) with an average follow-up time of 3.8 years, and the studies on metal-ceramic FDPs provided data for 1163 total FDPs (10.4% lost) with an average follow-up time of 8 years. The meta-analysis showed the 5-year survival rate of metal ceramic FDPs was significantly (P< 0.0001) higher at 94.4% [95% CI: 91.1-96.5%] compared to an all-ceramic FDP 5-year survival rate of 88.6% [95% CI: 78.3-94.2%]. Allceramic FDPs were found to have a 2.11 times higher annual failure rate [95% CI: 1.35–3.28%; P< 0.001] than metal ceramic FDPs.
With regards to biological and technical complications, the compared rates of all-ceramic and metal-ceramic FDPs for caries, abutment tooth fracture, loss of pulpal vitality, periodontal disease, marginal gaps/discoloration, and loss of retention were all found to be statistically not significant. However, the rate of veneer chipping for all-ceramic FDPs was significantly (P< 0.0001) higher at 13.6% [95% CI: 6.6-26.9] as compared to metal-ceramic FDPs with traditional feldspathic veneering ceramics which were only 2.9% [95% CI: 1.2-6.8%]. As for framework fracture, the 5-year complication rate for all-ceramic FDPs was also significantly (P< 0.0001) higher at 6.5% [95% CI: 3-13.8%] as compared to metal-ceramic FDPs with a rate of 1.6% [95% CI: 0.9-2.9%]. Having said that, it is important to note the annual rate of zirconia framework fracture was a rare complication ranging only between 0 and 0.48%. The majority of all-ceramic fractures occurred in either glass-ceramic or InCeram FDPs with an annual failure rate ranging between 1.88 and 4.24%.
Due to the lack of randomized clinical trials, only cohort studies were available for this review which exhibit a lower level of evidence. Also, since all-ceramic FDPs were a recent development at the time of this review, the estimated annual failure rates could only be partly extrapolated to the follow-up times of metal-ceramic FDPs which were twice as long (8 years compared to 3.8 years). Because of this, a clear limitation of this review is the assumption of a constant annual event rate however, the authors tried to reduce the impact of this bias by limiting the analysis to only a 5-year survival rate. Ultimately, it was concluded that all-ceramic FDPs have a significantly higher failure rate than metal-ceramic FDPs but if an all-ceramic FDP is to be used, a zirconia core should be chosen as the framework material. Although the result will be more aesthetic, it should be taken into consideration that these FDPs exhibit higher rates of veneer chipping as compared to PFM FDPs. As technology advances, these shortcomings of zirconia reconstructions will be overcome, but more research still needs to be done on the longterm survival rates of all-ceramic FDPs before that day comes.
Article 3: All-ceramic or Metal-Ceramic Tooth-Supported Fixed Dental Prostheses (FDPs)? A Systematic Review of the Survival and Complication Rates. Part II: Multiple-unit FDPs
The aim of this study was to update the previous systematic review with an additional literature search from 2006-2013 to evaluate the 5-year survival and biological/technical complication rates of tooth-supported FDPs over an average of 3 years. Articles were considered if they had human trials with a minimum 10 patients with FDPs, had at least on average a 3 year follow up time, had patients examined clinically, reported details of the study design, and were one of the following types of studies: randomized control trial, controlled clinical trial, prospective case series, cohort study, or retrospective study. In vitro and preclinical studies, reports based on questionnaires, interviews, and charts, or any article that did not meet the inclusion criteria were excluded. From an initial list of 580 titles, two independent reviewers selected a total of 40 studies to be included, 10 of which were taken from the previous iteration of this systematic review. The majority of articles included were prospective or retrospective studies, but there were also 4 randomized controlled trials.
Of the studies included, 29 reported on all-ceramic FDPs with a total of 1225 patients and a mean drop-out rate of 8%. There were 15 studies that reported on metal-ceramic FDPs with a total of 1669 patients and a mean dropout rate of 19%. For all studies, the patients ages ranged from 16 to 90 years old at the time of treatment. The 5-year survival rate of metal ceramic FDPs was 94.4% (95% CI: 91.2-96.5%) compared to 89.1% (95% CI: 80.4–94.0%) for reinforced glass ceramic FDPs, 86.2% (95% CI: 69.3–94.2%) for glass-infiltrated alumina FDPs and 90.4% (95% CI: 84.8–94.0%) for densely sintered zirconia FDPs. When comparing the 5-year survival rates of all-ceramic FDPs to that of metal-ceramic FDPs, only glass-infiltrated alumina FDPs showed a statistically significant difference (p=0.052) with a relative failure rate of 2.58 (0.99- 6.69).
Technical and biological complications discussed in this article were the same as in article 2 however, in this article metal-ceramic FDPs were used as a reference (complication rate = 1.00) to compare to three groups of all-ceramic FDPs. The only two statistically significant biological complication rates were for secondary caries on abutment teeth and loss of the FDP due to periodontal disease. Densely sintered zirconia FDPs were 2.75 (1.50-5.07) times as likely (p=0.001) to get caries and glass-infiltrated alumina FDPs and reinforced glass ceramic FDPs were 28.80 (9.45-87.74) and 10.8 (1.82-64.31) times as likely (p< 0.0001 & 0.009) to be lost to periodontal disease respectively as compared to metal-ceramic FDPs. As for technical complications, glassinfiltrated alumina FDPs and reinforced glass ceramic FDPs were 22.72 (5.13-100.69) and 13.81 (3.65-52.28) times more likely to be lost due to framework fracture respectively (p< 0.0001). Densely sintered zirconia showed much more resilience to framework fracture with a relative complication rate of only 3.23 (0.91-11.42) but this was not statistically significant (p=0.069). However, densely sintered zirconia suffered a significantly higher incidence of ceramic fractures (p=0.018) and loss of retention (p=0.028) as compared to all other types of FDPs.
Similar to the previous article, this review had to extrapolate the data for all-ceramic FDPs to produce 5-year survival rates which assumed a constant annual event rate throughout the study period. This was because the average follow-up time for metal-ceramic FDPs was 7 years while only 4.7 years for all-ceramic FDPs. Another limitation of this review is that the majority of studies were conducted at institutions or specialty clinics, therefore the outcomes observed cannot be generalized to private practice. The conclusions were that over an average 3-year period, metal-ceramic FDPs had lower failure rates than all-ceramic FDPs. Although it was shown that densely sintered zirconia is more stable than other all-ceramic FDPs with regards to resistance of framework fracture, it had more issues with discoloration, secondary caries, and loss of retention. This was attributed to the fabrication process which results in a more frequent semi-optimal fit as compared to other FDPs. More advancements and further refinements need to be made to all-ceramic FDPs before they can replace metal-ceramic FDPs as the new standard.
Conclusion and Recommendations
Due to a low quality of evidence, it cannot be definitively stated that metal-ceramic FDPs provide a better long-term prognosis for patients as compared to all-ceramic FDPs. There are more long-term studies on metal-ceramic FDP survival whereas only medium-term studies are currently available for all-ceramic FDPs. When extrapolating the data to account for this, the reviews show statistically significant evidences that metal-ceramic FDPs have a higher survival rate than all-ceramic FDPs. However, this introduces bias into the data since they are assuming a constant annual event rate, and while the authors try to limit this bias by only calculating 5-year survival rates, it is too short a length of time to be considered long-term. Additionally, the articles on metal ceramic FDPs are older and of a lower quality, not reporting as many clinical details and statistical data as the modern standard for research requires.
One major takeaway from these systematic reviews is that the difference in frequency of framework fracture is negligible between zirconia and metal cores however; all-ceramic FDPs exhibit a higher incidence of veneer chipping as compared to metal-ceramic FDPs. A critical issue concerning this observation has to do with the bonding strength of all-ceramic systems. Despite a more aesthetic result, the adhesion between zirconia frameworks and porcelain ceramic is still not up to the same standard as metal-ceramic bonding [2]. So until more advancement is made in the field of all-ceramic restorations, I would recommend using metal-ceramic FDPs especially in the posterior segment for their added strength and resistance to veneer chipping. Additionally, in the following case report I will demonstrate how an aesthetic result can be achieved using a special cutback technique for metal-ceramic FDPs.
Patient Description
A 65-year-old white male patient presents to the clinic with chief complaint “My top front teeth are all worn away.” He is retired and lives alone in his Manhattan apartment. Social history reveals he drinks less than daily only for social occasions, and smokes marijuana approximately once every couple of weeks. The patient’s medical history is significant for type 2 diabetes mellitus (HbA1c 6.4 mg/dL), stage III chronic kidney disease, hypertension, coronaryartery bypass grafting surgery, hypersensitivity lung disease, and GERD. Medications taken include Ezetimibe, Atorvastatin, Metformin, Clopidogrel, Metoprolol Succinate, Chlorthalidone, Nifedipine, Lisinopril, Doxazosin, and Omeprazole. His family history reveals a history of hypertension on his father’s side and type 2 diabetes mellitus on his mother’s side. Blood pressure monitoring shows an average reading of 133/82 P: 74 which classifies the patient as stage 1 hypertension.
The lower PFM bridge spanning teeth 22-27, fabricated in the 1980’s, violates the biologic principles of a healthy dentition. As shown in Figure 1, the FPD is notably overbuilt in both the incisal plane, contributing to a reverse curve of Spee, and in the facial plane, as indicated by the suboptimal emergence profile. While there is no evidence of a diminished vertical dimension nor excessive wear facets in the posterior dentition relative to biological age, the severe attrition is thought to be attributed to the mandibular fixed partial denture. Furthermore, the patient reports a parafunctional clenching habit, exacerbating the incisal wear over time.
Assessment of Treatment Decision
Clinical Question: In patients undergoing restorative treatment with fixed partial dentures, would a porcelain- fused-to-metal or an all-ceramic bridge lead to better long-term prognosis?
Resolving the patients chief concern and correcting the aesthetic appearance of the maxillary anterior teeth requires first addressing the root cause of the attrition. Therefore, replacement of the existing fixed partial denture is imperative to establish proper occlusion and ensure adequate interocclusal space for the new maxillary restorations. The mandibular arch form should be adjusted lingually to create ideal overjet and overbite. Following the extractions, the patient expressed he is not interested in replacing teeth #’s 2 and 31. As for site #28 he plans to get an implant there at a later time. Given the severe attrition, all four maxillary incisors need to be prepared for full coverage crowns. Whereas the maxillary canines only exhibit moderate wear, so they can instead be prepared for ¾ crowns to preserve the patients bite on natural tooth structure. Additionally, teeth #’s 5, 12, and 21 were treatment planned for facial veneers to enhance the overall aesthetics of the smile. Following completion of the case, an occlusal guard is fabricated to manage the parafunctional clenching habit and safeguard the integrity of all fixed prostheses.
Based off the appraised literature we know that PFM bridges have stood the test of time, whereas the newer all-ceramic counterpart has been demonstrating a higher incidence of chipping and fractures. Although more longterm research and advancements in ceramic FDPs need to be made, it was clear for the time being that a PFM bridge will yield a better long-term prognosis for my patient than an all-ceramic FPD. Considering this is an anterior restoration and aesthetics are a concern, we opted to implement the technique shown in Figure 8 for the fabrication of the mandibular FPD to eliminate the presence of a metal collar. This method of using a reduced metal framework with extended porcelain shoulder remains as the aesthetic standard for fixed partial dentures [4]. This process did not entail any additional cost to the patient and aligned with his treatment goals and expectations.
Risk Assessments
The patient’s medical risk is classified as an MCS-1A since his medical conditions are stable and under control. However, there are three main conditions of concern that can lead to adverse events in the dental chair. Due to the type 2 diabetes mellitus the patient could suffer a hypoglycemic event, so I make sure before each appointment that he has a snack with him or has eaten prior to treatment. To address the Stage III chronic kidney disease, I avoid giving any NSAIDs for pain. And lastly the hypertension could cause angina, stroke, or myocardial infarction. For this reason, vitals are taken at every appointment, the use of epinephrine is limited, stress-reducing techniques are used in the clinic, and I make sure the patient has taken his medications as prescribed. Due to the complex medical history and multiple medications being taken, a medical consultation was sent to the patient’s primary physician prior to the start of invasive treatment to assess his level of control. Additionally, at each appointment I confirm with the patient that his medical conditions are still under management and are being regularly monitored by his physician.
Caries risk assessment is based off the ADA classification system [1]. Disease indicators include one new carious lesion in the past 36 months and the risk factors are visible plaque, exposed root surfaces, recreational drug use, and two existing interproximal restorations. These factors classify the patient as moderate caries risk. Therefore, the patient would be managed with a 6-month clinical re-evaluation with appropriate bitewings and periapical radiographs as needed every 12 months. I make sure to reinforce oral hygiene at every visit and advise the patient to brush and floss twice a day, use fluoride mouthwash, and seek dietary counseling with a licensed nutritionist.
Periodontal risk assessment is based off the AAP Staging and Grading Classification [9]. The patient has generalized Stage I Grade B periodontitis because there is only 1-2 mm of clinical attachment loss, and the radiographic bone loss has only advanced to the coronal third of the roots. However, in the area of the upper right molars, the patient exhibits localized stage III Grade B periodontitis because he lost tooth #2 to periodontitis and the radiographic bone loss has extended to the middle third of the roots in this segment. Since the patient does not smoke cigarettes nor have an HbA1c above 7 mg/dL, he does not qualify for any grade modifiers. Following the periodontal treatment, the patient requires maintenance visits every 3 months.
Oral cancer risk is low for this patient because he does not have any of the associated risk factors. He has no history of oral cancer or presence of pre-cancerous lesions, no history of any other cancer, and he does not smoke or drink more than two drinks a day. He will continue to be monitored for any signs of malignancy or cancerous lesions at all future appointments.
The patients BMI is 38, his HbA1c is 6.4 mg/dL (prediabetes), and he has a moderate caries risk. Although there are no intra-oral nutrition risk indicators, his BMI places him in the obese category, leading to a high nutritional risk assessment, which the patient refused to address through nutritional counseling. Moreover, these risk factors also tie in with the patient’s obstructive sleep apnea risk assessment. Given his high blood pressure, wide neck, large tongue, and obesity he was made aware of his risk for sleep apnea and referred to get a sleep study done. The patient does not smoke tobacco and is not afraid of the dentist (answered 0 out of 10 for dental fear), so the tobacco risk assessment and dental fear assessments are both not applicable to this patient.
Discussion of Positive Findings
The head and neck exam revealed no signs of pathology such as asymmetry or palpable lymph nodes. There was however, clicking on the left TMJ, bilateral lingual tori, severe attrition of the maxillary incisors, and a parafunctional habit of clenching. Periodontally, the patient presented initially with clinical attachment loss (CAL) ranging from 3 to 10 mm in the posterior dentition with the most severely affected area being the upper right molars. The plaque score was 70 % and there was bleeding on probing noted on the maxillary and mandibular molars. Tooth #2 had class 2 mobility and tooth #28 had class 3 mobility.
As for the dentition, tooth #3 had recurrent decay under the previous MOL restoration and the OL amalgam restoration on tooth #14 was slightly roughened but the margins were still intact. Tooth #28 was found to have idiopathic root resorption which falls within reason based off the class 3 mobility and radiographic appearance. The patient has canine guidance, but the occlusion is classified as pathologic because of the severe wear of the maxillary incisors. Due to a lack of wear on the posterior dentition and in accordance with the patient’s personal recollection, the pre-existing 6-unit mandibular bridge was too bulky and resulted in excessive occlusal forces on the anterior teeth. Even the radiographs in figure 2 show the short, blunted roots of the maxillary incisors which is a sign of occlusal trauma. This prompted a consultation with the endodontist who concluded that all of the maxillary incisors were vital.
Since tooth #2 was periodontally compromised and tooth #28 had idiopathic root resorption, the prognosis for these two teeth was hopeless. The remaining dentition had a fair prognosis: posteriorly due to periodontitis and anteriorly because of severe attrition. Overall, the problem list includes:
- ● Chief complaint: “My top front teeth are all worn away.”
- ● Medical history:Type 2 diabetes mellitus,stage III chronic kidney disease, hypertension, coronary artery bypass grafting surgery, hypersen- sitivity lung disease, and GERD
- ● Generalized Stage I Grade B Periodontitis,Localized Stage III Grade B Periodontitis
- ● #3 MOL Recurrent decay, #28 Idiopathic root resorption
- ● Severe attrition of maxillary incisors
Description of the Treatment Plan
Due to the generalized Stage I Grade B and localized Stage III Grade B periodontitis the patient will need four quadrants of scaling and root planning followed by a periodontal outcome of care visit. The health promotion plan will encompass 3-month periodontal maintenance and 6- month clinical re-evaluations. Since the caries risk is moderate, he will need to undergo radiographic re-evaluation every 12 months with reinforcement of oral hygiene instruction at every visit. He was offered nutritional counseling due to the BMI and caries risk but refused. However, the importance of nutrition and its role in the caries process should still be reinforced during his recall appointments. Given his complex medical history, the patient should regularly see his physician and maintain a healthy diet and exercise to help control the hypertension and diabetes.
The sequence of treatment will be first to gather all the diagnostic information such as a complete medical history, diagnostic casts, radiographs, and discuss oral hygiene instruction. Next, we will control any active disease and eliminate any source of infection by performing the four quadrants of scaling and root planning, extracting teeth #2 and #28, and doing the restoration on #3 MOL. Subsequently, the preparation and delivery of comprehensive prosthodontic care will encompass the fabrication and placement of crowns and veneers. Finally, the last phase will be maintenance and re-care.
The rationale for the treatment plan stems from stopping further disease progression and eliminating sources of infection. #3 MOL has recurrent decay and needs to be treated to prevent potential damage to the pulp or sources of pain for the patient. Based off the evidence from Newman and Carranza’s Clinical Periodontology the best initial course of treatment for my patient’s periodontitis is four quadrants of scaling and root planning and the extraction of any hopeless teeth such as #2 and #28 [5]. If following the outcome of care appointment, the patient still has persistent pocketing and CAL then a referral would be made to PG Periodontics for more comprehensive treatment.
With regards to the prosthodontic treatment plan, the rational for remaking the existing bridge is to create space for the maxillary restorations without having to open the vertical dimension of occlusion. Since the 6-unit mandibular bridge rises above the posterior plane of occlusion, we would need to either crown all the posterior teeth to match the vertical dimension set by the bridge or remake the bridge to return the patient to his physiologic position. Given that the mandibular posterior teeth were all in good condition, remaking the bridge was the most conservative option. As for the material selection, the literature review brought us to the conclusion that PFM yields a greater longterm prognosis as opposed to all-ceramic FPDs [3,7,8].
Assessment of the Sequence of Care
The sequence of care followed the initial treatment plan, but the timeline of care was delayed due to the large financial cost of the final restorations. Therefore, after all the data was gathered and the treatment plan approved, all disease processes were stopped first. Two arches of scaling and root planning with appropriate follow ups, the extraction of #28, and #3 MOL were done. Despite the hopeless prognosis of tooth #2, the patient wanted to wait until after sufficient time had passed from the scaling and root planning was completed to see if the tooth would show any signs of improvement. Unfortunately, the tooth did not respond well to the SRP and given the severe bone loss and class 2 mobility it was eventually extracted. Once the periodontium was stabilized and the patient was financially prepared, the final crowns were initiated and delivered.
Assessment of the Outcomes of Care and Prognosis
Patient care at each visit was comprehensive, cohesive, and executed in a timely manner. He was very satisfied with the treatment outcomes and felt that his chief complaint was adequately addressed. The patients risk factors were also reduced in multiple aspects. He did not have any additional carious lesions during the course of our treatment which lasted over a year, therefore he can now be classified as low caries risk instead of moderate. Periodontally, the probing depths, CAL, plaque score, and bleeding on probing were all reduced as a result of the periodontal treatment and continued maintenance visits. Overall, the care provided turned out as well as expected. You can see in figure 9 the significant change it made in the patient’s appearance and self-confidence.
One aspect I would have preferred to approach differently is the enhancement of interdisciplinary collaboration with sleep medicine specialists to optimize the management of sleep-related disorders. The patient has a large tongue, a very wide neck, and screened positively for obstructive sleep apnea. Incorporating a sleep study into the treatment plan would have allowed for the final night guard to be modified to accommodate any necessary oral appliances. When we discussed this with the patient, he mentioned he had previously undergone a sleep study but was unable to fall asleep with the device, making him reluctant to repeat the process. We informed him about newer, more comfortable devices and encouraged him to undergo another sleep study. Although the existing study confirmed a diagnosis of sleep apnea, its outdated nature and questionable accuracy prevented us from making any treatment plan alterations based on its results.
The long-term prognosis for the delivered treatment is optimistic, given the comprehensive interdisciplinary approach to addressing periodontal disease, tooth extractions, and prosthodontic rehabilitation. The final choice of materials for the replacement of the existing mandibular bridge aligned with evidence-based findings for better longterm durability and success. The patient has returned for two postoperative visits to check occlusion and evaluate the new restorations, both of which required minimal adjustment. He was advised on proper oral hygiene practices, including brushing twice daily and flossing once daily using a crossmovement pattern to clean underneath the bridge. Since obstructive sleep apnea has been linked to bruxism and other adverse health effects the importance of wearing his night guard and undergoing another sleep study was emphasized. Moving forward, the patient will need to attend regular 3-month periodontal maintenance visits, 6-month clinical re-evaluations, and radiographic re-evaluations every 24-36 months, given his new low caries risk classification.
Final Summary and Conclusions
In this case report, a comprehensive treatment plan was successfully executed for a 65- year-old male patient presenting with severe wear on his maxillary incisors and requiring replacement of an existing PFM bridge. The primary objective was to address the patient's chief complaint while considering his complex medical history and oral health status. A comparison of PFM and all-ceramic bridges was undertaken to determine the best material choice for achieving long-term success. The literature review highlighted that while all-ceramic bridges have certain advantages, such as improved aesthetics, they tend to exhibit higher rates of technical complications like chipping and fracture compared to PFM bridges. Based on the available evidence, PFM bridges were recommended for this patient due to their demonstrated longevity and durability, aligning with the goal of achieving a stable and predictable longterm prognosis.
The treatment plan involved a staged approach including periodontal therapy, tooth extractions, and prosthetic rehabilitation with full coverage crowns and veneers. Risk assessments were carefully considered given the patient's medical conditions, aiming to minimize potential adverse events during treatment. Emphasis was placed on patient education and maintenance protocols to optimize long-term outcomes.
Assessment of the outcomes of care and prognosis revealed positive results with comprehensive reduction of risk factors and successful restoration of aesthetics and function. The patient's chief complaint was effectively addressed, and the long-term prognosis of the delivered treatment is optimistic. The decision to opt for PFM bridges over all-ceramic bridges was validated by the patient's satisfaction and clinical outcomes. Moving forward, the patient was provided with instructions for long-term care, including proper oral hygiene practices, use of an occlusal guard to manage Para functional habits, and regular follow-up visits for periodontal maintenance and evaluation. Ongoing collaboration with medical providers and continued patient education will be essential to ensure sustained oral hygiene and overall health.
In conclusion, this case report underscores the importance of evidence-based decisionmaking in restorative dentistry, particularly when managing complex cases involving patients with significant medical histories. By incorporating a systematic approach and integrating current literature findings, the treatment plan was tailored to achieve optimal outcomes and provide a foundation for long-term oral health and patient satisfaction.
- American Dental Association (2024) Caries Risk Assessment Form (Age >6).
- Diniz C, Nascimento RM, Souza JC, Henriques BB, Carreiro AF (2014) Fracture and shear bond strength analyses of different dental veneering ceramics to zirconia. Mater Sci Eng C Mater Biol Appl. 38: 79-84.
- Heintze SD, Rousson V (2010) Survival of zirconiaand metal-supported fixed dental prostheses: a systematic review. Int J Prosthodont. 23: 493-502.
- Magne P, Magne M, Belser U (1999) The esthetic width in fixed prosthodontics. J Prosthodont. 8: 106-18.
- Newman MG, Takei HH, Klokkevold PR, Carranza FA (2019) Newman and Carranza’s clinical periodontology.
- Pjetursson BE, Brägger U, Lang NP, Zwahlen M (2007) Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant supported FDPs and single crowns (SCs). Clinical Oral Implants Research, 18: 97-113.
- Pjetursson BE, Sailer I, Makarov NA, Zwahlen M, Thoma DS (2015) All-ceramic or metalceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part II: Multiple-unit FDPs. Dent Mater. 31: 624-39.
- Sailer I, Pjetursson BE, Zwahlen M, Hämmerle CH (2007) A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin Oral Implants Res. 3: 86-96.
- Tonetti MS, Greenwell H, Kornman KS (2018) Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol. 89: S159-72.
FIGURE 1

Figure 1: Initial Clinical Photographs
FIGURE 2
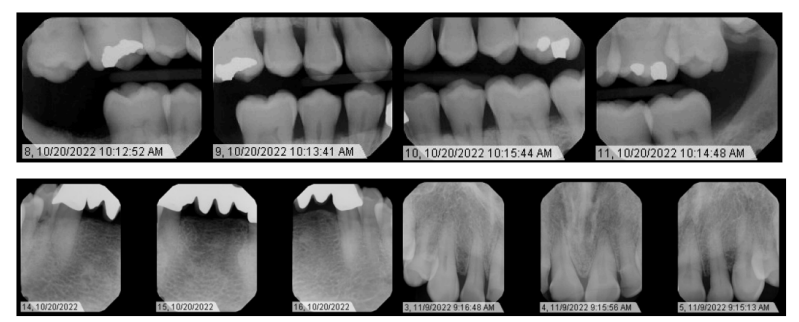
Figure 2: Initial Radiographs ‑ 10/20/2022 & 11/09/2022
FIGURE 3
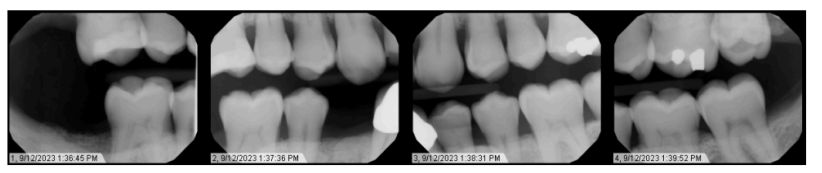
Figure 3: Most Recent Bitewing Radiographs ‑ 9/12/2023
FIGURE 4
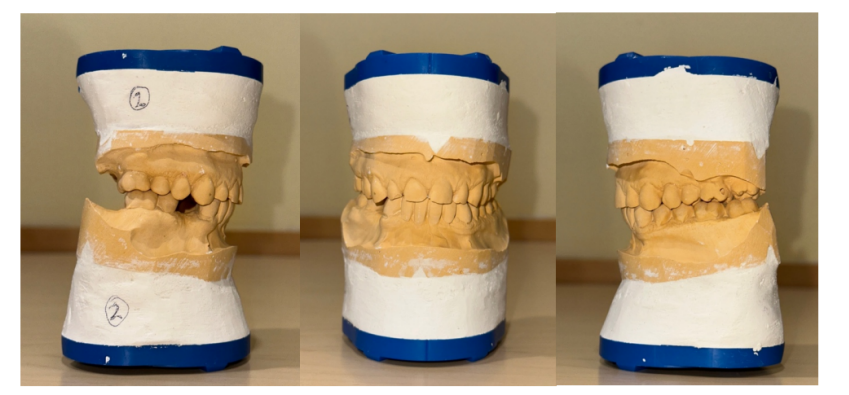
Figure 4: Study Models
FIGURE 5

Figure 5: Crown Preparations
FIGURE 6

Figure 6: Waxed Up Models
FIGURE 7

Figure 7: Temporary Restorations
FIGURE 8
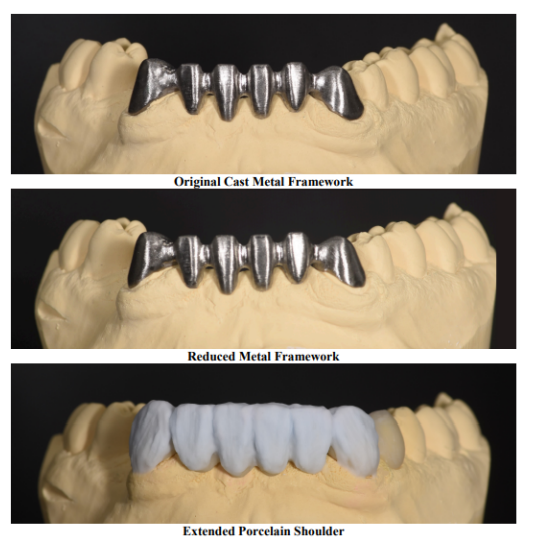
Figure 8: Images courtesy of New-Dent Aesthetics Lab
FIGURE 9

Figure 9: Final Restorations
FIGURE 10

Figure 10: Comparison of pre-operative photos (left) and post operative photos (right)
Tables at a glance
Figures at a glance