Multidisciplinary Approach for Treatment of a Missing Tooth - Periodontal Therapy, Orthodontic Treatment and Implant Placement: A Case Report
Received Date: August 07, 2024 Accepted Date: September 07, 2024 Published Date: September 10, 2024
doi: 10.17303/jdoh.2024.11.103
Citation: Junyi Ge, Qianjia Pan, Chenyang Shi, Peipei Wang, Min Gu (2024) Multidisciplinary Approach for Treatment of a Missing Tooth - Periodontal Therapy, Orthodontic Treatment and Implant Placement: A Case Report. J Dent Oral Health 11: 1-8
Abstract
Background: Missing teeth are a common phenomenon in the population and can lead to a number of harmful effects, such as reduced chewing efficiency, aesthetic impact on the face and damage to the integrity of the dental row. We describe a case of a multidisciplinary approach using periodontal, orthodontic and implant treatment to restore the function of a missing tooth for a patient
Case presentation: A twenty-nine-year-old male patient who had his right mandibular first molar extracted five years ago due to decay. Because of the difficulty in chewing, the patient wanted to restore the missing tooth with an implant denture. The patient was in poor periodontal condition, with red and swollen gums and bleeding on probing. Chronic tooth loss has caused the adjacent teeth to tilt, the opposing teeth to elongate and loss of restorative space. In order to meet the patient's requirements and achieve a therapeutic outcome, we decided to use a combined multidisciplinary treatment, including full mouth periodontal treatment, partial orthodontic treatment, implant placement and final crown restoration.
Conclusion: Combined multidisciplinary treatment allows patients to receive the most minimally invasive, simple and comfortable, fast and efficient treatment. The combined periodontic-orthodontic-implant treatment of a missing tooth restores the patient's chewing function on both sides, avoiding discomfort and muscle swelling in the joint area and the skewed facial shape caused by long-term unilateral chewing. It comforts to the concept that “craniofacial-articular-maxillofacial-dental” is a whole.
Keywords: Multidisciplinary Treatments; Implant; Orthodontic Treatment; Periodontal Therapy
Introduction
Nearly half of the world's population suffers from oral disease, and the loss of teeth due to oral disease can lead to functional impairment, for example, chewing and aesthetic impairment, which, depending on where the teeth are lost, can ultimately affect quality of life [1,2]. Severe tooth loss affects about 2% of the world 's population [3] and has been shown to be linked to many diseases. Kyungdo et al. [4] found that tooth loss was associated with end-stage renal disease through a cohort study. Pablo et al. [5] found that the lower the number of teeth, the greater the risk of cognitive decline. Xu et al. [6] found a relationship between tooth loss and accelerated aging. Therefore, it is imperative to repair the missing teeth in time. Common options for restoring missing teeth include fixed partial dentures, removable partial dentures and implant dentures. Fixed partial dentures have traditionally been the gold standard for the treatment of partially missing teeth. However, its treatment is not advisable when there are no abutments distal to the edentulous area or when the edentulous area spans a long distance [7]. Treatment with removable partial dentures is a non-invasive and low-cost solution for the restorative rehabilitation of patients with functional or aesthetic needs for posterior tooth replacement, however there is a risk of localized damage to the remaining teeth and their supporting tissues [8]. Therefore, implant dentures seem to be the most suitable restorative option. With a survival rate of over 90%, implant dentures are becoming a popular choice and the global oral implant market is expected to grow to $13.01 billion by 2023 [9]. However, the choice of implant prosthesis for the restoration of missing teeth must meet the following conditions: the bone on the labial, buccal and lingual-palatal side of the implant should be healthy and not less than 1.5 mm thick, the distance between the implants should not be less than 3 mm and the distance between the implant and the natural neighboring teeth should not be less than 2 mm. The root of the implant should not be less than 2 mm from the upper edge of the mandibular canal[10]. The patient in this case was unable to meet the conditions for implant surgery due to a reduction in the restorative space caused by chronic tooth loss. The patient also had poor oral hygiene and red and swollen gums, which did not allow for a healthy gingival bond with the implant once it was placed, affecting the long-term outcome. We therefore decided to use combined multidisciplinary treatment to improve the patient's periodontal situation, widen the restorative space and finally place the implant for crown restoration to restore the patient's masticatory function and dental row integrity.
Methods and Results
A 35-year-old Chinese man visited our hospital with the complaint of a dental implant denture restoration in the right mandible. The patient had his right mandibular first molar extracted 5 years ago due to tooth decay, which affected his chewing. An intraoral examination revealed left molar neutral to submedial relationship, bilateral cuspids all neutral to submedial relationship, I°deep overjet deep overbite, upper and lower arch crowding, gaps in lower arch, 12, 22, 33, 43 torsion, 32, 35, 42 lingual inclination, 31, 32, 33, 41, 42, 43 crowding, 46 gaps, 47, 48 submedial inclination, 14, 15, 16, 17, 24, 26, 27 sulcus caries, 48 interrupted teeth, upper and lower arch incongruity, lower arch median right 1 mm, alveolar process full, intraoral periodontal condition poor, gingiva mildly red and swollen, local bleeding on probing (Figure 1). X-rays showed the lower right second molar and lower right third molar were tilted proximally to the centre and the lower right first molar had a small restorative space (Figure 2). Measurement of the patient's intraoral plaster model with a straightedge showed a restorative gap of only about 1 cm (Figure 3). Orthodontic treatment can help widen the gap between missing teeth, allowing patients who would otherwise not be eligible for implant restorations to regain access to dental implant [11]. Luo et al. [12] found that bracketless invisible appliance can correct inclined teeth faster than traditional straight wire appliance. However, bracketless invisible braces are expensive and have a long treatment period. The patient was reluctant to undergo up to two years of full mouth orthodontic treatment to widen the gap for implant restoration. Local orthodontics compared to full orthodontic treatment time is shorter, reducing the occurrence of root resorption, can be carried out as early as possible in the later implant treatment, and through local orthodontics to realign and organise the teeth, in order to solve the occlusal disorders, repair the gap between the missing teeth at the same time, but also to solve the jawbone and the buccal surface of the problem of incongruity [13].
Therefore, we decided to adopt a relatively short treatment time of partial micro-orthodontics to straighten the lower right second molar and then performed the implant surgery once sufficient implant space had been created. The peri-implant mucosa may influence the aesthetic outcome, patient satisfaction, biological and clinical stability, which are key factors for a good long-term prognosis [14]. So before orthodontic treatment, it was essential to restore the patient's periodontal tissues to health. Firstly, the periodontist performed a full periodontal scaling and subgingival scaling, after which the patient's bleeding gums improved significantly.Afterwards, a 10*2mm temporary anchorage devices (Ormco corporation, USA) was implanted in the region of the right mandibular ascending branch, and the buccal tubes of 47 and 48 were cemented (Ormco corporation, USA). A close spring was used to connect the temporary anchorage devices and buccal tube to make 47 upright. At the same time, a fixed cast ring aligner (Jin Guan Qian corporation, China) consisting of 4 orthodontic bands and 1 lingual arch was bonded in the patient's mouth to reinforced anchorage. A lingual spring with double loop was welded to the orthodontic band of the 45 for uprighting the tilted 47 (Figure 4).
After a period of approximately two months, the patient could observe at the follow-up consultation that the right mandibular second molar was gradually becoming upright and the implant space in the right mandibular first molar was beginning to increase (Figure 5). After another three months of orthodontic maintenance treatment, the right mandibular first molar had sufficient proximal and distal mesial restoration space and began to enter the space maintenance phase (Figure 6). After two months, the partial orthodontic appliance was removed and an implant (Institut Straumann, Waldenburg, Switzerland) was placed in the right mandibular first molar, but the temporary anchorage devices was temporarily retained in the right mandibular ascending area to prevent gap reduction (Figure 7).
Three months after implant placement, the patient's temporary anchorage devices were removed and an all-ceramic crown restoration was performed on the upper part of the implant, and a mandibular compression retainer was fabricated and entered the retention phase (Figure 8). Follow-up three months after crown restoration: stable bilateral occlusion, no significant inflammation around the implant, good joint and periodontal condition (Figure 9). One year and three months after the completion of the multidisciplinary treatment, the patient was followed up in the hospital. The clinical examination showed a stable occlusion in the posterior region, a healthy temporomandibular joint and good peri-implant osseointegration (Figure 10). Three years and five months of follow-up showed that the implant denture was stable and the soft and hard tissues around the implant were in good condition (Figure 11).
Discussion and Conclusion
The use of implant dentures to replace missing teeth has gradually become mainstream. It has the advantages of not needing to grind the hard tissue of the tooth and being more comfortable than removable partial dentures [15]. However, the implementation of implant surgery also needs to meet the corresponding conditions. For example, in this case, the adjacent teeth were inclined so that the repair gap was narrowed and the implant could not be placed. At this time, it is undoubtedly a good choice to cooperate with other departments for multidisciplinary comprehensive treatment. A core element of a multidisciplinary team is to bring together of specialists from different therapeutic areas to form teams to plan and design the patient's treatment [16]. Peri-implantitis is an important cause of implant failure, which affects the formation of good osseointegration between the implant and surrounding components, resulting in the loss of supporting bone [17]. While bacterial infection plays a major role in peri-implantitis, and it has been reported in the literature that the bacterial flora causing periodontitis and peri-implantitis are similar [18].
Therefore, the first step of treatment was to have a periodontist performing a thorough periodontal scaling on the patient to remove plaque, soft scale and supragingival and subgingival calculus, restored the health of the periodontal tissue, prevented the occurrence of peri-implantitis, and ensured implantation success. After improving the patient's periodontal condition, the second step in the treatment is to extend the reduced implant space. When a tooth is missing, the three-dimensional dynamic equilibrium of the dentition is disrupted and the tooth will tilt or move into the missing space until a new equilibrium is achieved, which may result in the destruction of periodontal tissue and disruption of the bite [19]. Commonly used orthodontic methods to make the mandibular molars upright include cantilever springs, helical upright springs, etc. [20]. In addition, some scholars use implants as anchorage to make molar upright [21]. Due to the bone anchorage system can achieve efficient orthodontic movement with low morbidities [22], the orthodontist used temporary anchorage devices in conjunction with orthodontic partial appliance to obtain sufficient space for implant. Finally, the implant was placed by the implantologist and the crown restoration was completed afterwards. However, this case also has some limitations. Although we have solved the patient 's complaint of missing teeth, the patient still has some problems such as deep overbite, deep overjet, and crowded dentition. These problems cannot be solved by partial orthodontic treatment so we cannot achieve the best treatment results.In addition, managing peri-implant mucositis is the primary prevention of peri-implantitis [23]. The patient had gingivitis before repair, and the reason for his missing teeth was caries, which proved that the patient 's oral health management ability was poor. Therefore, after the completion of implant denture repair, whether the patient can maintain good oral cleaning measures was our concern. Fortunately, in several follow-up visits, the implant denture area was in good condition. But further observation was needed.
All in all, the treatment group achieved the goal of repairing patients' missing teeth in a short period of time through multidisciplinary combined treatment of periodontal, orthodontic and implant. The patient was satisfied with the whole treatment process, and was pleased that he did not need to receive full mouth orthodontic treatment and the good experience of implant denture use. When a patient has insufficient implant space and does not wish to undergo full mouth orthodontic treatment, a combined multidisciplinary approach can be used to restore the integrity of the dental row and establish a correct occlusal relationship. This case demonstrates the close and orderly cooperation between the periodontist, orthodontist and implantologist, suggesting that combined multidisciplinary treatment is one of the most minimally invasive, simple, comfortable, fast and efficient treatments for the patient.
Acknowledgements
Authors have no conflict of interest related to the report.
Authors’ Contributions
JG obtained the medical records and contributed to manuscript writing.PW performed orthodontic procedure. LZ performed implant surgery.MG performed peridental treatment and contributed to manuscript writing. All authors read and approved the final manuscript.
Funding
The design of the study and collection, analysis, and interpretation of data, and the manuscript writing was supported by funding from Top Talent of Changzhou "14th Five-Year Plan" High-level Health Personnel Training Project (2022260), 2023 Soochow University Graduate Education Reform Achievement Award Cultivation Project (KY20231517), Young Project of Changzhou Health Commission (Grant No. QN202310) and National Key R&D Program of China (2022YFA0807300).
Availability of Data and Materials
The corresponding author can provide the datasets used and/or analyzed during the current study upon reasonable request.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing Interests
The authors declare that they have no competing interests.
- Singh A, Peres MA, Watt RG (2019) The Relationship between Income and Oral Health: A Critical Review. J Dent Res, 98: 853-60.
- Gerritsen AE, Allen PF, Witter DJ, et al. (2010) Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. J Health Qual Life Outcomes, 8: 126.
- Kassebaum NJ, Bernabe E, Dahiya M, et al. (2014) Global Burden of Severe Tooth Loss: A Systematic Review and Meta-analysis. J Dent Res, 93: 20S-8.
- Han K, Park JB (2021) Tooth loss and risk of end-stage renal disease: A nationwide cohort study. J Periodontol, 92: 371-7.
- Galindo-Moreno P, Lopez-Chaichio L, Padial-Molina M, et al. (2022) The impact of tooth loss on cognitive function. J Clin Oral Investig, 26: 3493-500.
- Xu KH, Li L, Jia SL, et al. (2023) Association of Tooth Loss and Diet Quality with Acceleration of Aging: Evidence from NHANES. Am J Med, 136: 773-9 e4.
- Kim JJ (2019) Revisiting the Removable Partial Denture. J Dent Clin North Am, 63: 263-78.
- Budtz-Jorgensen E, Bochet G (1998) Alternate framework designs for removable partial dentures. J Prosthet Dent, 80: 58-66.
- Alghamdi HS, Jansen JA (2020) The development and future of dental implants. J Dent Mater J, 39: 167-72.
- Zhang ZY (2020) Oral and maxillofacial surgery 8th edition [M].
- Zhang LQ (2014) Combined application of oral implant and orthodontics [J]. Gansu Science and Technology Information, 43: 1156-91.
- Luo ZQ, Yang LP, Cheng L (2024) Bracketless Invisible Orthodontic Treatment Combined with Implant Restoration in the Treatment of Malocclusion with Dentition Defect and Its Effects on Masticatory Function. J Chinese Journal of Aesthetic Medicine, 33: 124-8.
- Yang KQ (2017) Clinical outcome of local orthodontics combined with implantation in the treatment of longterm loss of first molars. J The World Clinical Medicine, 11: 138-41.
- Chackartchi T, Romanos GE, Sculean A (2000) Soft tissue-related complications and management around dental implants. J Periodontol. 81: 124-38.
- Smielak B, Andruch I (2018) Multistage implantology-orthodontic-prosthetic treatment: A case report. J Am Dent Assoc, 149: 787-93 e3.
- Taberna M, Gil Moncayo F, Jane-Salas E, et al. (2020) The Multidisciplinary Team (MDT) Approach and Quality of Care. J Front Oncol, 10: 85.
- Dutta SR, Passi D, Singh P, et al. (2020) Risks and complications associated with dental implant failure: Critical update. Natl J Maxillofac Surg, 11: 14-9.
- Prathapachandran J, Suresh N (2012) Management of peri-implantitis. Dent Res J (Isfahan), 9: 516-21.
- Liu XQ, Yang Y, Zhou JF, et al. (2021) Three-dimensional movement of posterior teeth after losing the interproximal and occlusal contacts in adults. 53: 594-7.
- Magkavali-Trikka P, Emmanouilidis G, Papadopoulos MA (2018) Mandibular molar uprighting using orthodontic miniscrew implants: a systematic review. J Prog Orthod, 19: 1.
- Shellhart WC, Moawad M, Lake P (1996) Case report: implants as anchorage for molar uprighting and intrusion. J Angle Orthod, 66: 169-72.
- Tsui WK, Chua HD, Cheung LK (2012) Bone anchor systems for orthodontic application: a systematic review. Int J Oral Maxillofac Surg, 41: 1427-38.
- Jepsen S, Berglundh T, Genco R, et al. (2015) Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol, 42: S152-7.
FIGURE 1

Figure 1: Pretreatment intraoral photographs showing intraoral plaque and soft tartar build-up, red and swollen gums and missing right lower jaw first molar
FIGURE 2

Figure 2: Pretreatment panoramic radiograph showing a severe inclination of the lower right second molar and third molar proximally
FIGURE 3

Figure 3: Pretreatment measurement of the patient's intraoral plaster model showing a lack of adequate restoration space
FIGURE 4

Figure 4: Insertion of a temporary anchorage devices and bonding of a fixed cast ring aligner
FIGURE 5

Figure 5: The implant gap gradually increased after about two months of orthodontic treatment
FIGURE 6

Figure 6: Intraoral photographs showing sufficient space for implant restoration
FIGURE 7

Figure 7: Radiographs showing implant placed in the right mandibular first molar region
FIGURE 8
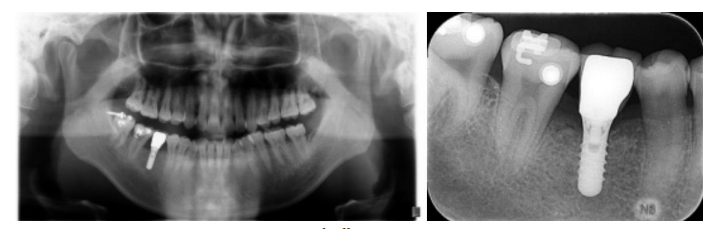
Figure 8: Patients with all-ceramic crown restorations
FIGURE 9

Figure 9: Intraoral photographs and radiographs showed that the implant denture was functioning well in the mouth
FIGURE 10

Figure 10: One year and three months after the end of the patient's multidisciplinary combined treatment
FIGURE 11

Figure 11: Three year and five months after the end of the patient's multidisciplinary combined treatment
Figures at a glance