Laser-welded Infrastructure for Immediate Loading Protocols in the Mandible: Case Report
Received Date: September 23, 2024 Accepted Date: October 23, 2024 Published Date: October 26, 2024
doi: 10.17303/jdoh.2024.11.105
Citation: Pedro Giorgetti MONTAGNER, Antonio Marcos MONTAGNER, Maria Cristina PEDRAZINI, Rafael Leonardo Xediek CONSANI (2024) Laser-welded Infrastructure for Immediate Loading Protocols in the Mandible: Case Report. J Dent Oral Health 11: 1-8
Abstract
The rehabilitation of edentulous patients with immediate loading implants has become a safe procedure that guarantees aesthetic, psychological, social, and functional aspects. Several immediate functional loading protocols have been proposed to treat total edentulism. One of the key points in the construction of dentures is the method of getting passivity, which is infrastructure construction. This study aims to present a clinical case report that describes the oral rehabilitation by lower jaw fixed implants-supported prosthesis with a laser-welded framework using titanium bar TIG (Tungsten Inert Gas) welded and upper jaw complete denture explaining the limitations and step-by-step procedure. This technique proved a viable alternative for oral rehabilitation of jaw edentulism among all limitations based on the clinical and follow-up observed results.
Keywords: Dental Implants; Dental Prosthesis; Laser Welded Titanium; Edentulous Patients; Tungsten Inert Gas
Introduction
Implant dentistry has adopted various techniques for rehabilitating totally or partially edentulous patients. Among these techniques, functional activation with immediate loading on dental implants stands out [1,2]. This approach is valued for its rapid esthetic and functional recovery, as well as for improving the psychological and social aspects of the patients. However, the success of this technique requires an understanding of biomechanical principles and a detailed assessment of the patient's clinical profile [3]. A well-structured treatment plan is essential for the method's efficacy, and various protocols have been proposed and successfully applied. It is considered a viable alternative to traditional methods that require a longer healing period before prosthesis placement [4].
The use of TIG (Tungsten Inert Gas) welded titanium bars is a technique that offers an effective solution for infrastructure fabrication to implant‐supported rehabilitation. TIG welding is considered to be a precise and resistant technique that allows for rigid metal structures, which are essential for the success of immediate loading. This method has satisfactory clinical results and is biocompatible and superior to conventional techniques due to the bars' fabrication employing the casting process [5]. However, like all laboratory work, failures may occur during the process, especially with regard to the depth of the weld, generating voids and incomplete welds [6].
Passive adaptation of the infrastructure and primary stability of the implants are fundamental factors in the long-term success of dental rehabilitation [3]. Lack of passivity can lead to serious complications such as bone resorption around the implants and fracture of the prosthetic abutments and/or screws. Conventional casting techniques can cause inaccuracies due to faulty manufacturing processes or improper material handling. On the other hand, TIG welding of titanium bars offers an alternative with the potential to minimize these risks, allowing precise customization and passive fit of the prosthesis [7,8].
Determining factors for choosing immediate activation of osseointegrated implants that represent the greatest advantage are the speed of the rehabilitation process and mechanical precision [9,10]. Patients who have undergone multiple extractions and implant placement can benefit from a rapid functional and aesthetic recovery, often on the same day as surgery. This approach aligns with patients' expectations for prompt and effective solutions, which can help reduce the morbidity associated with treatment and improve patients' quality of life [11].
In TIG welding, the arc is created between a non-- consumable electrode and the metal workpiece, with a flow of inert gas surrounding the electrode to minimize oxidation during the process. This technique is commonly used in manufacturing and industrial maintenance for welding thin plates (0.2 to 8 mm) of materials such as carbon steel, stainless steel, aluminum and its alloys, copper and its alloys, titanium, zirconium, nickel and its alloys, and tungsten. Since TIG welding equipment is less expensive than laser welding, it offers a potential cost reduction in oral rehabilitation procedures. Assessing the impact of TIG welding on the properties of titanium, such as tensile and flexural strength, is crucial to exploring its viability as a more affordable alternative to laser welding in the production of implant-supported prostheses [12].
TIG welding for titanium bars is an important example of how dentistry needs to use engineering concepts to clinically address bone and tissue biology, [13] promoting favorable healing, well-being, self-esteem, and the quality of the procedures performed. In this way, immediate functional loading using TIG-welded titanium bars is considered a significant development, enabling fast, safe, and effective solutions [14].
This study aimed to report a clinical case involving conventional maxillary and mandibular implant‐supported rehabilitation using TIG welding to make metal bars for Branemark protocols.
Case Report
Diagnosis and Treatment PlanPatient SR (57-year-old female) wearing maxillary complete dentures and unsatisfactory mandibular removable dentures (Figures 1A and 1B). Radiographic examination revealed a retaining abutment of the mandibular removable prosthesis with a periapical lesion (Figure 1C) and level III mobility due to advanced periodontal disease assessed during clinical examination. The patient was offered maxillary complete conventional dentures, extraction of the remaining mandibular teeth, and subsequent installation of osseointegratable implants for implant-supported fixed complete dentures according to the Branemark protocol, with activation by immediate loading.
Subsequent medical examinations and preoperative imaging tests were requested in addition to sodium alginate molds assembled for the study models. After the models had been composed using type III stone plaster, individual maxillary and mandibular trays were made along with provisional test bases with wax planes for maxillo-mandibular registration.
Surgical ProceduresSixty minutes before surgery, a prophylactic therapeutic protocol was carried out, including amoxicillin 1g, dexamethasone 4mg, and dipyrone sodium 500mg. The mandibular alveolar nerve was blocked using bupivacaine hydrochloride with epinephrine 1:200,000 (Neocaine; Cristália Produtos Químicos e Farmacêuticos, Itapira, São Paulo, SP, Brazil) and infiltration anesthesia in the vestibular and lingual sulcus with 2% lidocaine with epinephrine 1:200,000 (Alphacaine 100; DFL Indústria e Comércio, Rio de Janeiro, RJ, Brazil). Next, an incision was made with a 15c blade (Solidor; Lamedid, Barueri, SP, Brazil) on the alveolar crest in the region of the first and second premolars and intrasulcularly on the incisors and canines, followed by a mucoperiosteal detachment of the flap to locate the mental foramen. Teeth 22 to 27 were extracted, the ridge regularized and the surgical site prepared for subsequent milling.
After formalizing the mandibular alveolar ridge, the milling sequence was started following the milling cutter manufacturer's protocol (Conexão Sistemas de Prótese, Arujá, SP, Brazil) and 4 cylindrical osseointegrated implants with an external hexagon junction were installed. The distal implants (21 and 28) were milled 11.0 mm deep and 3.5 mm in diameter to install a 3.75x 10 mm implant. The mesial implants (23 and 26) were milled 9.0 mm deep and 3.5 mm in diameter to install an implant measuring 3.75 x 9 mm. All implants had satisfactory primary locking of around 32 N/cm2 for immediate activation, positioned three-dimensionally and perpendicular to the long axis of the teeth while the distal implants were positioned slightly inclined. The titanium mini pillars were installed with the 20 N torque recommended by the manufacturer, followed by the impression transfers for open trays.
Simple suturing was carried out using 4-0 monofilament nylon thread (Tecnofio, Goiânia, GO, Brazil). The impression transfers were bonded with acrylic resin (Pattern; GC América, São Paulo, SP, Brazil) and molded with condensation silicones of regular and heavy consistencies. The long screws were then released and the impression was taken. The transfers were relieved with sculpting wax, the analogs were positioned and the special plaster was poured into the mold to obtain the working model and make the metal infrastructure for the mandibular dentures complete.
The titanium cylinders specifically designed for laser welding were positioned on the minipillar analogs. The set was then sent to the prosthetics laboratory to create the titanium bar obtained by TIG welding. The models were assembled in a semi-adjustable joint from the maxillo-- mandibular registration made on the test base and maxillary wax plane.
The level of immediate postoperative satisfaction for patients was high, following all therapeutic recommendations and without pain according to several clinical studies and literature reviews. The seven-day postoperative follow-up was free of pain. This type of oral rehabilitation offers instant significant aesthetic, functional, and psychosocial benefits to the patient as witnessed in postoperative.
Dental ProsthesisAfter partially removing the gingiva around the welded metal bar, a 10 N/cm2 torque was applied to the mini pillar screws, and the screw access ducts were closed with Teflon tape (Veda Rosca; Tigre, Joinville, SC, Brazil) and temporary restorative material (Clip F; Voco, Germany). When the prostheses were delivered, the first occlusal adjustment was made with carbon paper for articulation (40µm Arti-check; Baush, Cologne, Germany), eliminating premature contacts in centric relation and checking for maximum habitual intercuspation, right and left laterality and protrusion, respecting the principle of balanced bilateral occlusion. In the follow-up session, fine occlusal adjustment was performed with a diamond drill (3118; KG Sorensen, Serra, ES, Brazil) and polished with rubbers and aluminum oxide brushes (DhPro; Paranaguá, PR, Brazil).
The patient was instructed to hygiene the area using a soft or extra soft tooth-brush and mouthwash with 0.12% chlorhexidine digluconate solution (Periogard; Colgate, São Paulo, SP, Brazil) three times a day for 15 days (Figure 2A).
Post-operative control was carried out 3, 5, and 7 days after the procedure. After 7 days, the suture was removed to allow healing, with no bleeding, inflammatory exudate, pain, or edema and considerable patient satisfaction. After 14 days, occlusal adjustments were made to the prostheses, verifying the presence of good tissue repair. Once again, the patient was instructed to brush with soft bristles. After 30 days, the patient was examined with radiographs to check the adaptation of the intermediate abutments and prosthesis cylinders (Figure 2B).
Discussion
The immediate activation of implant technique in dental prosthetic rehabilitation is widely recognized in literature, achieving osseointegration and biomechanical passivity while eliminating the need for a second gingival surgery to adapt the analogs, guaranteeing the patient's comfort. Previous studies [2,4,15] have shown that immediate activation protocols are consistent with traditional methodologies, with similar success rates. This case report was considered as an option for the rapid fabrication of metal frameworks and the construction of conventional or implant-supported complete dentures, emphasizing the importance of adaptation and control of the rehabilitation process in order to achieve the expected clinical results in the treatment of totally edentulous patients.
In this context, welding techniques have been widely used in the dental field to reduce the distortions generated by single-piece casting and machining techniques based on the lost wax method [13]. In this study, the metal bar was manufactured using the TIG welding technique on titanium cylinders for conventional mini pillars with 22º angulation adapted to implants installed on the same day after the procedure [5,14] to avoid possible distortion caused by conventional manufacturing. In addition, TIG welding was chosen due to the better mechanical properties of the metal bar and better biological properties for interaction with periodontal tissues [8].
The existence of misalignment in implant-supported prostheses results from the transfer of stress to the rehabilitation system, increasing the risk of biological and mechanical complications, such as loosening or fracture of retaining screws, compromising proper osseointegration [1]. This is due to the rigid connection between alveolar bone tissue and implants, preventing or hindering the adequate dissipation of tensions. Even in the absence of functional loads, misalignment can also induce stress in the implant-- supported system. Although misfit values of between 10 and 150 μm are considered clinically acceptable, it is important to note that these values have been established empirically. Therefore, it would be essential to obtain minimum misfit values for the manufacture of implant‐supported rehabilitation [13]. A significant fact to be considered is the positioning of the bar on the implant abutments, with the cylinder adaptation being measured using an exploratory probe or by means of a periapical radiographic examination using a radiographic film positioner during seating [9].
One limitation of this technique there is no consensus regarding the penetration depth of the laser beam. The literature indicates a penetration ranging from 1.5 mm to 2.5 mm, concluding that the metal thickness can vary from 3 mm to 5 mm. However, other authors suggest that the recommended metal thickness could range from 2.4 mm to 3 mm. It can bring failures on the approach of cylinder and titanium bar and consequently fracture of welding bridges during mastigatory and swallowing efforts [6].
Reducing the degree of maladjustment of implant-- supported prostheses is the goal of research and is still a condition to be achieved. Therefore, some misfit correction techniques are required to correct maladjustment after transfer molding and obtaining the working cast. Welding can prevent distortions that may be caused by molding materials, fabrication techniques, coating, and casting. In this clinical rehabilitation, it was possible to observe the operative sequence of the design and fabrication of the implant-- supported prosthetic infrastructure using the TIG welding technique and its clinical benefits. When well performed, it strengthens the prosthetic structure, improves the transmission of forces to the abutments, and allows for greater stability of the total prosthesis [2]. On the other hand, this technique also has some disadvantages, such as insufficient weld penetration in the metal bar and the presence of porosity in the welded area. For this reason, regular clinical and radiographic evaluation of the patient is required [13].
From the point of view of metallurgical engineering through metallographic analysis, it is essential that laboratory, casting and welding processes, maintain the continuity of the metal and the homogeneity of its physical, structural and mechanical properties, thus avoiding fractures, porosity and disadaptation. Any defects must be investigated and corrected. The joint between the metal parts must be free of defects at the bar-weld interface [6].
Over time, protocols for the construction of fixed total prostheses on implants have been developed to achieve passivity between the over-molded cylinders and the intermediate abutments to increase the success rate [7]. These protocols have been refined over time, with the underlying mechanical concept for correct installation remaining consistent. TIG welding for creating metal infrastructures has emerged as a viable and effective alternative [15], as evidenced by its application in the dental rehabilitation presented in this case.
The utilization of welded infrastructure for fixed total prostheses on osseointegrated implants has been demonstrated to achieve success rates of 98% in both the maxilla and mandible. Long-term implant stabilization and low rates of marginal bone resorption during bone remodeling have been demonstrated in studies that have followed patients for periods ranging from 6 to 11 years. These outcomes have been observed when the technical and biological concepts are respected. However, fracture of the acrylic base of the prosthesis has been identified as the most significant complication in the literature [16].
Laser welding is a technique used in dentistry that is capable of manufacturing high-quality weld joints with remarkable consistency. In this clinical case, the protocols used were like those employed in previous studies; however, it is necessary to continue monitoring the patient over an extended period.
Conclusion
The immediate functional loading protocol using TIG-welded titanium bars is a notable development in clinical dental practice, providing an efficient alternative for the rehabilitation of edentulous patients. The method is considered an approach that allows aesthetic and functional restoration with positive results, favoring a better quality of life for the patient.
Declarations
Ethics Approval
Not applicable.
Consent to Participate
Not applicable.
Availability of Data and Material
Data used in the discussion were found in peer-reviewed journals and previously published case reports. Appropriate citations and references are included in the article.
Competing Interests
The authors declare no competing interests.
Funding
This study did not receive funding.
Authors’ Contributions
PGM – conceptualization, dental procedure, bibliographical survey, review, writing of the initial and final version
AMM – dental procedure and researcher responsible for support in final article review.
MCP – researcher responsible for support in writing, figures and final article review.
RLXC – researcher responsible for support in final article review.
All authors have read and approved the final manuscript.
Acknowledgements
The authors would like to thank Ms. Thereza C. P. de Castilho for promptly volunteering to review this manuscript for its English language content.
- Ganeles J, Rosenberg MM, Holt RL, Reichman LH (2001) Immediate loading of implants with fixed restorations in the completely edentulous mandible: report of 27 patients from a private practice. Int J Oral Maxillofac Implants. 16: 418-26.
- Bousquet P, Carayon D, Durand JC (2021) Using the "One Shot" concept for immediate loading implant protocol in edentulous patient rehabilitation with a fixed prosthesis: A 6-year follow-up. Case Rep Dent. 2021: 8872277.
- Tarnow DP, Emtiaz S, Classi A (1997) Immediate loading of threaded implants at stage 1 surgery in edentulous arches: ten consecutive case reports with 1- to 5-year data. Int J Oral Maxillofac Implants. 12: 319-24.
- Hosoume JH, Costa MT, Silva MAR, Bellini DH (2011) Immediate load using bar titanium welding with TIG: case report. Innov Implant J, Biomater. Esthet. 6: 80-5.
- Cumbo E, Gallina G, Messina P, Bilello G, Isaqali Karobari M, Scardina GA (2024) Soldering in Dentistry: An Updated Technical Review. J Clin Med. 13: 809.
- Pedrazini MC, Oliveira RAF, Fabiano S, Montagner AM, Wassall T (2013) Evaluation of the laboratorial processes' quality applied to titanium prostheses: plasma casting and laser welding-metallographic analysis. Revista Gaúcha de Odontologia. 61: 221-6
- Longoni S, Sartori M, Ariello F, Anzani M, Baldoni M (2006) Passive definitive fit of bar-supported implant overdentures. Implant Dent. 15: 129-34.
- Watanabe I, Baba N, Chang J, Chiu Y (2006) Nd:YAG laser penetration into cast titanium and gold alloy with different surface preparations. J Oral Rehabil. 33: 443-6.
- Capelli M, Zuffetti F, Del Fabbro M, Testori T (2007) Immediate rehabilitation of the completely edentulous jaw with fixed prostheses supported by either upright or tilted implants: a multicenter clinical study. Int J Oral Maxillofac Implants. 22: 639-44.
- Yilmaz B, Ozcelik TB, McGlumphy E (2015) Using the "final-on-four" concept to deliver an immediate metal-resin implant-fixed complete dental prosthesis. J Prosthet Dent. 114: 161-6.
- Jackson BJ (2005) The use of laser-welded titanium framework technology: a case report for the totally edentulous patient. J Oral Implantol. 31: 294-300.
- Atoui JA, Felipucci DN, Pagnano VO, Orsi IA, Nóbilo MA, Bezzon OL (2013) Tensile and flexural strength of commercially pure titanium submitted to laser and tungsten inert gas welds. Braz Dent J. 24: 630-4.
- Rodrigues SA, Presotto AGC, Barão VAR, Consani RLX, Nóbilo MAA, Mesquita MF (2017) The role of welding techniques in the biomechanical behavior of implant-supported prostheses. Mater Sci Eng C Mater Biol Appl. 78: 435-42.
- Paleari AG, Presoto CD, Vasconcelos JA, Nunes Reis JM, Pinelli LA, Tavares da Silva RH, et al. (2015) An alternative technique for fabrication of frameworks in an immediate loading implant fixed mandibular prosthesis. Case Rep Dent. 2015: 102189.
- Lorenzi Poluha R, Lamartine de Moraes Melo Neto C, Sábio S (2015) Prosthetic rehabilitation using association of total and implant-supported total denture (Brånemark protocol) – case report. RSBO Revista Sul-Brasileira de Odontologia. 12: 239-45.
- Gaonkar SH, Aras MA, Chitre V, Mascarenhas K, Amin B, Rajagopal P (2021) Survival rates of axial and tilted implants in the rehabilitation of edentulous jaws using the All-on-four™ concept: A systematic review. J Indian Prosthodont Soc. 21: 3-10.
FIGURE 1
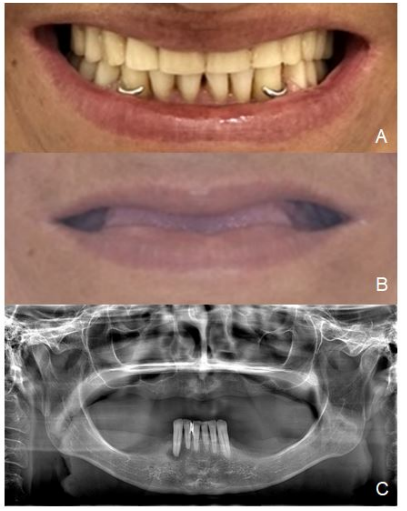
Figure 1A: Initial vestibular aspect. 1B - Initial vestibular aspect without dental prothesis. 1C - Initial panoramic radiograph
FIGURE 2
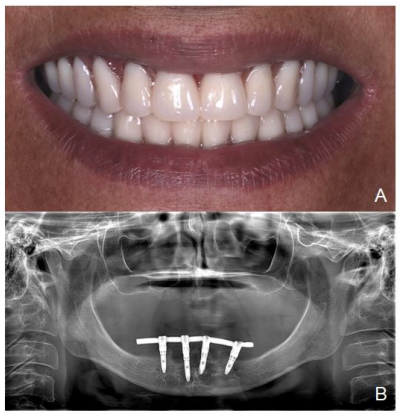
Figure 2A: Final vestibular aspect. 2B - Final panoramic radiograph
Figures at a glance