Evaluating the Effects of Orthodontic Banding on Gingival Health: A Six-Months Study
Received Date: April 30, 2025 Accepted Date: May 30, 2025 Published Date: June 02, 2025
doi:10.17303/jdoh.2025.12.201
Citation: Jose Maria Suárez Quintanilla, David Suárez Quintanilla, Mahmoud N. Almughany (2025) Evaluating the Effects of Orthodontic Banding on Gingival Health: A Six-Months Study. J Dent Oral Health 12: 1-12
Abstract
Objective: To evaluate the effect of orthodontic banding on gingival health parameters in patients receiving fixed orthodontic treatment, from the time of band cementation up to six months post-treatment.
Material and Methodology: The study was conducted on 30 participants, aged between 12 – 35 years from both genders needed fixed orthodontic treatment. The upper first molar was banded. Participants received instructions for proper oral hygiene and balanced dietary habits. The gingival parameters including Gingival Margin, probing depth, Gingival Index, bleeding on probing and Plaque Index were assessed and examined from the time of band cementation up to six months post-treatment.
Results: Statistical analysis Repeated measure ANOVA (Paired Sample Test) was used to analyze the data. Indicated that, there are significant differences when using cemented bands on gingival health parameters with duration.
Conclusion: The use of cemented bands for molar teeth during fixed orthodontic treatment has significant differences on gingival health parameters as it can influence these parameters at short rang.
Keywords: Fixed Orthodontics; Gingival Parameters; Cemented Bands; Molar
Introduction
Orthodontic banding, a crucial step in fixed orthodontic appliance treatment, ensures proper retention and resistance of the appliance against orthodontic forces. This is particularly important for molars, which endure significant forces during treatment. In orthodontics, attachments can be either banded as orthodontic bands or bonded as orthodontic tubes. Orthodontic appliances form a network in the dentition, which might exacerbate food stagnation [1]. The use of bands in fixed orthodontic equipment has grown in popularity due to the necessity for stability when using functional and orthopedic appliances such as headgear or facemasks, as well as lingual attachments like the transpalatal arch. Molar banding is a tried-and-true orthodontic technique that ensures proper retention and resistance to orthodontic forces. While advancements in adhesive solutions have made bonding attachments to molars commonplace, reducing clinical care time and improving oral hygiene [2]. Many orthodontists still prefer molar bands. This preference is driven by the belief that molar bands have lower failure rates and offer greater reliability [3]. With advancements in band design (mechanical retention mechanisms, micro-etching). Gingival health may be negatively impacted by the positioning of orthodontic bands, which are required to cover a significant portion of the tooth's surface and pierce deeply into the gingival sulcus to increase retention. Plaque buildup might result from using fixed equipment while disregarding appropriate dental hygiene guidelines. Gingivitis develops as a result of the detrimental alterations in microbiota caused by the plaque buildup accelerated by orthodontic appliances [4]. If inadequately managed, it may progress to periodontitis. Several factors can exacerbate gingival irritation when using orthodontic bands. Mechanical irritation of the gingival tissues, chemical irritation from the cement used, increased food impaction risk, and patients' tendency to clean anterior teeth more thoroughly than posterior teeth all play a role. Orthodontic treatment is a dual-action procedure affecting periodontal tissues, which can significantly enhance periodontal health or, conversely, lead to various periodontal disorders [5]. Atack et al., 1996 describes four reasons for increasing gingival inflammation with orthodontic bands [6]. These reasons come from irritation to gingival tissues, from cement used to band placement as it is cemented near to gingiva, increase risk of food stagnation and ability for participants to clean their anterior teeth better than posteriors.
This study aimed to evaluate the effect of orthodontic banding on gingival health parameters in patients receiving fixed orthodontic treatment, from the time of band cementation up to six months post-treatment
Material and Methodology
Selection of Patients came to our clinic from 05.03.2024 to 04.05.2024 which they 30 participants aged between 12 to 35 years, 11 adolescent and 19 adults from both genders 8 male and 22 female who had just commenced orthodontic treatment with fixed appliances. This study was conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Palestinian Health Research Council and the Ethics Committee approved the protocol of PHRC/HC/1169/24. And all participants provided written informed consent prior to their inclusion in the study. The Participants chosen according to the eligibility criteria, patients who are currently free of periodontitis, have not previously undergone orthodontic treatment, without underlying systemic diseases, non-pregnant females, and fall within the age range of 12 to 35 years old are included in the sample. Conversely, patients with missing maxillary first molars, those needing arch expansion or molar distalization, and individuals with systemic diseases are excluded from participation. Prior to cementing the molar band to one upper first molar, an assessment was conducted to evaluate gingival health parameters. This evaluation included measurements of the gingival margin, gingival index, plaque index and probing depth. This initial assessment was denoted as "T0." Subsequently, fixed orthodontic appliances were conventionally bonded using American orthodontic brackets, extending from the second premolar to the opposing second premolar. The upper first molar was fitted with a 3M-style metal band and cemented by Riva self-cure glass ionomer luting cement (SDI trademark). Participants were provided with comprehensive instructions emphasizing proper oral hygiene practices and maintaining a balanced diet with reduced sugar consumption to ensure a consistent environment during the study. After three months from the initial assessment (T0), a follow-up assessment of gingival parameters for the upper first molar was conducted and denoted as "T3." Similarly, the same assessment was repeated six months from the start of treatment, denoted as "T6." The using of bands especially molars are to strengthen the anchorage, bands wrap around the tooth so it’s hard to come off under masticatory forces compared to bonds, on the other hand, bands is suitable for auxiliaries attachments as arch wire, headgear and face mask and also sometimes bands used due to difficulty for molar bonding especially with partially erupted molars.
Clinical Evaluation
Gingival parameters were assessed through clinical examinations. A calibrated examiner conducted the assessments using a University of Michigan O probe with William’s markings. International indices were utilized for measurement, and a standardized periodontal diagnostic chart was employed to document the data.
Scoring Criteria
The following indexes used to measure the gingival parameters [7].
Results: Gingival parameters attributed to duration for cemented bands
Gingival margin index: Repeated Measure ANOVA
- Miller’s classification for gingival recession and Millers and Damm classification for gingival enlargement was used to measure the gingival margin, in case of gingival recession used (–) before the number and in case of gingival enlargement used (+) before the number.
- The Loe & Silness (1963) scheme was used to measure gingival index and Silness & Loe (1964) scheme was employed to measure the Plaque index.
- Probing depth was measured using The University of Michigan O probe with Williams markings, recording the distance from the gingival margin to the deepest part of the sulcus. Six readings were taken per tooth at specific locations.
From the previous table, the significance level value (P = 0.326 > 0.05) indicates that there are no statistically significant differences in the level of Gingival margin according to the duration of cemented bands using T0, T3 and T6 months.
From the previous table, there is no statistically significant differences regarding Gingival Margin as (P = 0.326 > 0.05).
Plaque index: Repeated Measure ANOVA
From the previous table, the significances level value (P = 0.000 < 0.05) indicated that there is statistically significant differences in the level of Plaque index according to the duration of cemented bands using T0, T3 and T6 months therfore, In order to identify the source of the differences, the compare means paired-samples T Test was used.
From the previous table, there is statistically significant differences regarding plaque index between T0 – T3 and T6 for the cemented bands. Mean that the best stage where the plaque is minimum at level T0 which is the best because the difference in plaque index from T0 till T6 = (1.1667-0.8333= 0.3334) as the plaque increased with time for the six months study period.
Gingival index: Repeated Measure ANOVA
From previous table, the significance level value (P = 0.000 < 0.05) indicated that there is statistically significant differences in the level of Gingival index according to the duration of cemented bands using T0, T3 and T6 months therefore, in order to identify the source of the differences, the compare means paired-samples T Test was used.
From the previous table, there is statistically significant differences regarding gingival index between T0 – T3 and between T0 and T6 for the cemented bands. means that the best stage where the gingival index minimum at level T0 and after that the gingival index changed with time for around six months because in the middle 3 months between T3 – T6 there is no significant difference between the values. Therefore, the clear difference needs around 6 months to be noticed.
Bleeding on probing: using Chi-square Test
From previous table, there is statistically significant differences regarding Bleeding on probing between T0, T3 and T6 for the cemented bands, means that there is bleeding on probing changes for different stages of study duration.
Probing Depths: Repeated Measure ANOVA
All the measured 6 points for probing depths were calculated for an average and a Mean was used for the analysis for T0, T3 and T6.
From previous table. There is statistically significant difference regarding probing depth in the (p= 0.000<0.05) between T0-T3 -T6 for the cemented bands. to know the differences, compare means paired-samples T Test was used.
From previous table, there is statistically significant change in the average of probing depths between T0-T3 and T6. That mean the probing depth for the cemented bands changed from the beginning of the treatment and increased as the duration increased. The mean change in the noticeable between T0 and T6 around (2.3667-1.4333= 0.9334) which is high difference between the two values for a 6 months period.
Discussion
This study aimed to test the effects of using molar bands on gingival health during fixed orthodontic treatment, focusing on gingival margin, plaque index, gingival index, Bleeding on Probing and probing depth.
The findings indicated that, there is statistically significant differences of using cemented bands on molar teeth during fixed orthodontic treatment for all studied gingival parameters except gingival margin.
The gingival margin p value > 0.05 so that means gingival margin has not any significant change during the 6 months period. So, it’s not clear if this can change with increasing study period or not. May can do this in future study.
The study results are matching with a previous study done on 2023, by Amir et Al. to test the effect of orthodontic banding on gingival health of first permanent molars. The findings were Orthodontic banding can adversely affect gingival health in patients receiving fixed appliance treatment. Lack of proper oral hygiene maintenance further aggravates poor gingival health [8]. His study tested the palque index and gingival index only but this study tests other 3 gingival parameters and have the same results that using molar bands adversely affect molar gingival health. Another matching study done on June 2016 to by Shrestha to study the oral health status in patients with fixed orthodontic appliances with molar bands and bonded tubes for Nepalese orthodontic patients, the study found that the use of molar bands and molar tubes can cause progression of gingivitis and there is no significant change in periodontal health parameters in using cemented bands or bonded tubes when oral hygiene is controlled [9]. In 2018, a systematic review and meta-analysis study was done by Papageorgiou et al. to test the effect of orthodontic treatment of periodontal clinical attachments, the findings showed that from longitudinal clinical studies, orthodontic treatment with fixed appliances has little to no clinically relevant effect on periodontal clinical attachments levels and this is not matching with the research results [10]. Another study was done in November 2015, by Al Anezi et al. to test the effect of orthodontic bands or tubes upon periodontal status during the initial phase of orthodontic treatment. The findings of the study showed that molar bands are associated with greater periodontal inflammation compared to molar bonds in the first three months of treatment [11]. These results are matching with research results that gingival bands can affect gingival molar health. Al-Anezi study, the participants were twenty-four in mean age 12.6 years, that’s mean the majority of the participants were adolescent young ages, but in this research the sample was thirty patients and the majority of the participants were adults above 18 years, and this approve that this gingival change can occur with any age and associated with orthodontic bands, even this age the participants be cooperative and not careless regarding oral hygiene instructions.
In 2003, Al Hamdany, published an article about changes in gingiva with orthodontically banded and bonded teeth. The results indicated that orthodontic bands would provoke more periodontal changes than brackets. And this also matched with research results, with significant differences in the gingival health parameters with orthodontic bands [12]. Even that, Al Hamdany studied different teeth areas, bands were cemented to upper and lower first molars and rest of teeth bonded by composite. Teeth included in her study were upper right and lower left central incisors and upper left and lower right first molars. The teeth used in her study were in different areas that may alter her results as anterior area where central incisors present is a cleansable area while molars in the posterior area which is less cleansable area. but when we look to molar results we will find it matching with ours.
Conclusion
The use of cemented bands for molar teeth during fixed orthodontic treatment has significant differences on gingival health parameters as it can influence these parameters at short rang.
So, the orthodontists should make more concern on the gingival health and ensure that patients receive thorough oral hygiene instructions before and during treatment and using fluoride mouth rinses, interdental brushes. Regular periodontal evaluations should be integrated into orthodontic follow-up visits, especially for patients with pre-existing gingival conditions.
Declarations
Ethics Approval and Consent to Participate
This study was conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Palestinian Health Research Council and the Ethics Committee approved the protocol of PHRC/HC/1169/24. And all participants provided written informed consent prior to their inclusion in the study.
Consent for Publication
Not applicable
Funding
Not applicable
Authors' Contributions
Not applicable
- Lu H, Tang H, Zhou T, Kang N (2018) Assessment of the periodontal health status in patients undergoing orthodontic treatment with fixed appliances and Invisalign system: A meta-analysis. Med. 97: e0248.
- Flores-Mir C (2011) Bonded molar tubes associated with higher failure rate than molar bands. Evid Based Dent. 12: 84.
- Clark JR, Ireland AJ, Sherriff M (2003) An in vivo and ex vivo study to evaluate the use of a glasspolyphosphonate cement in orthodontic banding. Eur J Orthod. 25: 319–23.
- Huser MC, Baehni PC, Lang R (1990) Effects of orthodontic bands on microbiologic and clinical parameters. Am J Orthod Dentofac Orthop. 97: 213-8.
- Kapoor A, Singhal L, Kapoor S, Kapoor A (2016) Ortho-perio Interrelationships: An Overview. International Journal of Preventive and Clinical Dental Research, 3: 206–12.
- E Atack, JR Sandy, M Addy (1996) “Periodontal and microbiological changes associated with the placement of orthodontic appliances. A review.,” J Periodontol, 67: 78–85.
- S Reddy (2011) Essentials of Clinical Periodontology and Periodontics.
- Mashal Amir, Ayesha Iqbal, Farooq Maqsood, Ujala Saif, Mahnoor Parvez, Tariq Ali Khan (2023) The effect of orthodontic banding on gingival health of first permanent molars. The Professional Medical Journal, 30: 546–50.
- S Shrestha, A Sharma, B Lamichhane (2016) “Oral Health Status in Patients with Fixed Orthodontic Appliance with Molar Bands and Bonded Tubes,” Orthodontic Journal of Nepal, 6: 27.
- Papageorgiou SN, Papadelli AA, Eliades T (2018) Effect of orthodontic treatment of periodontal clinical attachment: A systematic review and meta-analysis. In European Journal of Orthodontics. 40: 176–84.
- Al-Anezi SA (2015) The effect of orthodontic bands or tubes upon periodontal status during the initial phase of orthodontic treatment. Saudi Dental Journal, 27: 120–4.
- al-Hamdani, A Kh (2003) Changes in gingiva with orthodontically banded and bonded teeth. University of Mosul College of Dentistry, 3: 39–43.
FIGURE 1
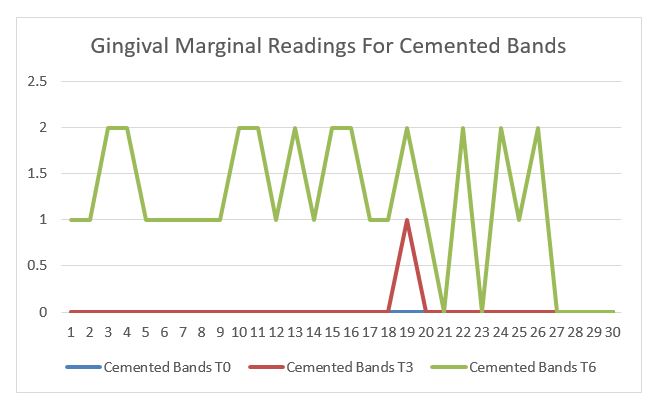
Figure 1: Descriptive statistics for Gingival marginal readings for cemented bands from T0 – T6
FIGURE 2
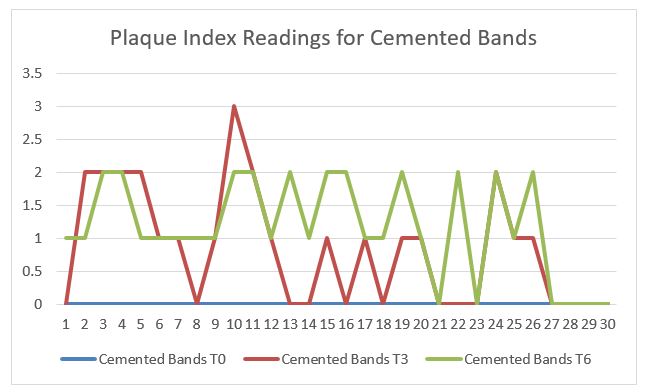
Figure 2: Descriptive statistics for Plaque Index readings for cemented bands from T0 – T6
FIGURE 3
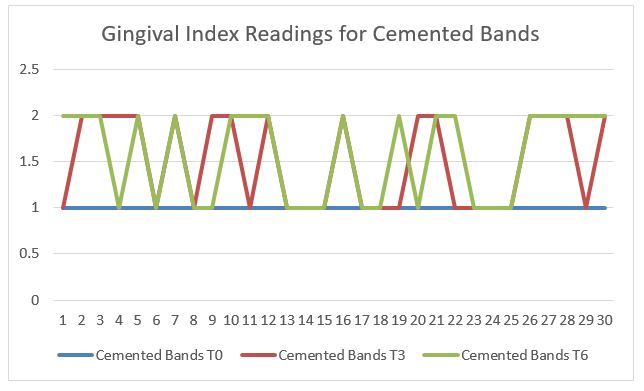
Figure 3: Descriptive statistics for Gingival Index readings for cemented bands from T0 – T6
FIGURE 4
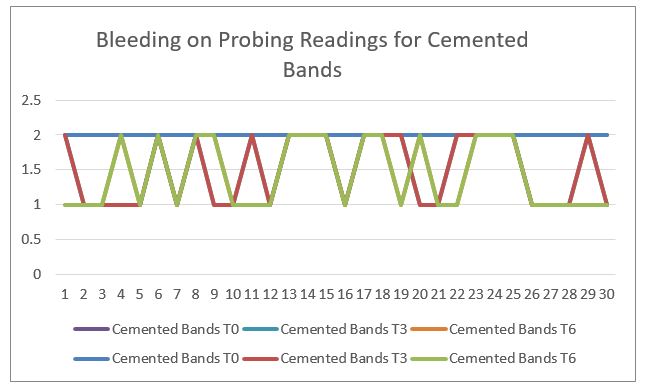
Figure 4: Descriptive statistics for Bleeding on Probing readings for cemented bands from T0 – T6 as 1 means bleeding, 2 means no bleeding
FIGURE 5
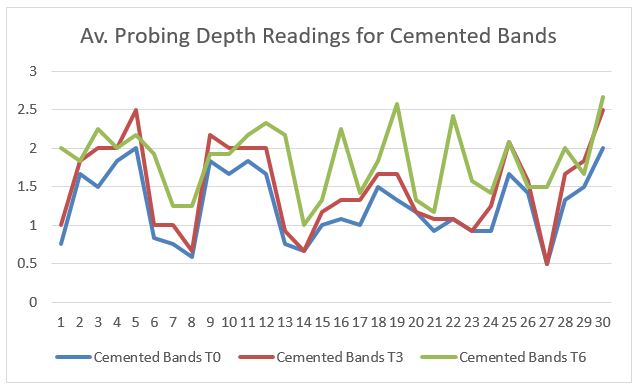
Figure 5: Descriptive statistics for Av. Probing Depths readings for cemented bands from T0 – T6
Tables at a glance
Figures at a glance