Impacted Twin Molars, A Rare Anomaly: A Case Report
Received Date: May 16, 2025 Accepted Date: June 16, 2025 Published Date: June 19, 2025
doi:10.17303/jdoh.2025.12.202
Citation: Dr Geeta Singh, Dr Saniya Zia, Dr Rangeet Bhadra, Dr Krishna Vasaiya (2025) Impacted Twin Molars, A Rare Anomaly: A Case Report. J Dent Oral Health 12: 1-7
Abstract
Symmetrically identical impacted third molars are rare, and this paper reports the case of a young female patient who reported to our department with the chief complaint of pain in the right lower back tooth region since a week and on investigation two identical fused impacted third molars were identified which were surgically extracted. Impacted third molars are a common entity, but the anatomical variations reported in such teeth are a rare phenomenon.
Keywords: Twin Molars; Anatomical Positioning; Prophylactic, Orthodontic; Mandibular Molars
Introduction
Third molars exhibit considerable variability in their anatomical positioning and angulation, often resulting in a high incidence of impaction and its surgical extraction is frequently indicated for prophylactic, orthodontic, or prosthetic considerations, as well as for the evaluation and management of associated pathological conditions. Consequently, the removal of third molars represents one of the most routinely performed dentoalveolar surgical procedures in the field of oral and maxillofacial surgery [1].
Indications for the extraction of third molars include acute or chronic pericoronitis, the presence of cystic or neoplastic lesions, periodontal disease, and carious involvement of the second or third mandibular molars [2].
Supernumerary teeth are the additional teeth beyond the normal complement and may develop in any region of the dental arch, though they are more frequently observed in the maxilla than in the mandible.
They have been named according to location where they are found such as mesiomolars, paramolars, parapremolars and distomolars. Regarding their shapes these can be, eumorphic, rudimentary, dysmorphic, tuberculous and conical.
Fusion is the union of two developing dental germs resulting in a single large dental structure. If this union occurs precociously, the crowns will be together with separate roots resulting in a big dental structure. If the union happens after the crown formation, the roots will probably be together.
This paper reports a case of a young female patient reported to the department of Oral and Maxillofacial Surgery, Faculty of Dental Sciences, King George’s Medical University, Lucknow, with the chief complaint of pain in the right lower back tooth region since a week and on investigating, two anatomically identical fused mandibular molar were identified and by surgical intervention the teeth were extracted in toto.
Case Report
A 15-year-old female reported to the author’s department with the chief complain of pain over the right lower back tooth region since a week. On clinical examination, no significant finding was present except tenderness at the right lower third molar region.
On further investigation, the orthopantomography revealed the presence of two fused right mandibular third molars completely embedded in the bone. A Cone Beam Computed Tomography (CBCT) was further done to identify the exact anatomy and location of the two teeth and to rule out any other suspected pathology and amount of bone around the teeth for further planning of the surgical intervention.
3 D imaging provides a myriad of information and hence aids in proper surgical planning by minimizing the chances of risk too.
The thorough investigation revealed the complete fusion of the two teeth and their location from the second molar and the inferior alveolar canal.
The patient was explained regarding the surgery and the possible consequences, and an informed signed consent was obtained.
Prior to the surgery, the extra oral and intra oral asepsis was obtained with povidone iodine.
The local anesthesia containing 2% Lignocaine with 1:200000 Adrenaline was administered to the Inferior Alveolar, Buccal and Lingual Nerve employing the three-point technique.
Following anesthesia, an envelope incision starting from the mesial aspect of the right second molar tooth was performed to expose the bone and using the Stainless-steel bur 704A, bone over and around the teeth was guttered to expose the teeth.
The two teeth were extracted in-toto followed by curettage of the socket and closure.
The patient was discharged same day under antibiotics coverage and follow up was done on 3rd, 5th ,7th day showed that the healing was uneventful.
Discussion
Dental malformation might be classified as gemination, twinning, concrescence, and fusion [3].
Fusion is the union between two individual developing teeth via dentin and/or enamel [4] and is believed to be related to physical forces or pressure that provokes close contact between developing teeth. However, its exact aetiology is unknown [5]. There is an equal preponderance amongst males and females [6]. The prevalence of fused teeth in the permanent dentition is 0.2% (unilateral) and 0.05% (bilateral) [7]. Noteworthy is that fusion commonly affects incisors, particularly the maxillary central incisors (3.6%) and then the mandibular third molars (0.9%) [8].
In this case, a rare phenomenon of eumorphic supernumerary tooth fused with mandibular third molars have been reported. Most of these are asymptomatic and rarely present with pain but are an incidental finding on the routine checkup.
Though periapical, occlusal and panoramic radiography helps in treatment planning, the use of CBCT to aid in surgical planning has been reported in the literature [10].
The most common impacted are mandibular third molars and maxillary third molars because of the lack of space in the dental or due to pathological change that may obstruct the normal eruption of the third molar [11,12].
The anomaly associated with such impacted teeth is also a rare entity and is usually an incidental finding on the routine radiograph finding without any associated symptoms.
Extraction of impacted teeth with anomaly becomes an integral part of the surgery because the impacted teeth have a higher incidence of dentigerous cysts than unicystic ameloblastoma and odontogenic keratocyst. These cysts' dental remnants surround the fully impacted teeth as well-defined peri coronal radiolucency on x-ray [13,14].
The teeth should be extracted without delay to minimize the risk of any complications as in a study by Bilodeau and Daniel it was stated that the postoperative complications increase with patient age. Hence, it is recommended that the immediate extraction of the impacted mandibular third molar, once a decision has been made, should be done well before the age of 25 years especially for women as they had significantly more problems with alveolitis, infections, and paresthesia than men. No specific factor was identified to explain this difference between the sexes [15].
Impacted mandibular molars are a common presenting complain in the clinical practice but the ones with any anomaly is a rare entity. Though literature explains two treatment protocol where wait and watch has been recommended as one of the treatment protocol in the asymptomatic cases while surgical intervention as the second treatment protocol.
It is highly recommended to surgical intervene as soon as it is found to prevent any future risk or complications.
- Fuster Torres MA, Gargallo Albiol J, Berini Aytes L, Gay Escoda C (2008) Evaluation of the indication for surgical extraction of third molars according to the oral surgeon and the primary care dentist. Experience in the Master of Oral Surgery and Implantology at Barcelona University Dental School. Med Oral Patol Oral Cir Bucal. 13: E499-504.
- Chiapasco M, De Cicco L, Marrone G (1993) Side effects and complications associated with third molar surgery. Oral Surg Oral Med Oral Pathol. 76: 412–20.
- Levitas TC (1965) Gemination, Fusion, Twinning and Concrescence. ASDC J Dent Child, 32: 93–100.
- Lucey S, Heath N, Welbury RR, Wright G (2009) Case Report: Cone-Beam CT Imaging in the Management of a Double Tooth. European Archives of Paediatric Dentistry, 10: 49-53.
- Neville BW, Allen CM, Bouquet JE (2002) Oral and Maxillofacial Pathology. 2nd Edition, WB Saunders, Oxford.
- Hamasha AA, Al-Khateeb T (2004) Prevalence of Fused and Geminated Teeth in Jordanian Adults. Quintessence International, 35: 556-9.
- Morris, D.O. (1992) Fusion of Mandibular Third and Supernumerary Fourth Molars. Dental Update, 19: 177-8.
- Pace A, Sandler PJ, Murray A (2013) Macrodont Management. Dental Update, 40: 23-6
- Hamasha AA, Al-Khateeb T (2004) Prevalence of Fused and Geminated Teeth in Jordanian Adults. Quintessence International, 35: 556-9.
- Ferreira-Junior O, de Avila LD, Sampieri MB, Dias-Ribeiro E, Chen WL, Fan S (2009) Impacted Lower Third Molar Fused with a Supernumerary Tooth— Diagnosis and Treatment Planning Using Cone-Beam Computed Tomography. International Journal of Oral Science, 1: 224-8.
- Richardson ME (1977) The etiology and prediction of mandibular third molar impaction. Angle Orthod. 47: 165-72.
- Tolstunov L (2014) The quest for causes of inferior alveolar nerve injury after extraction of mandibular third molars. J Oral Maxillofac Surg. 72: 1644-6.
- Srikanth G, Kamath AT, Kudva A, Singh A, Smriti K, Carnelio S (2018) A linguoverted impacted tooth with orocutaneous fistula - a rare case report. Clujul Med. 91
- Tsukamoto G, Makino T, Kikuchi T, Kishimoto K, Nishiyama A, Sasaki A, Matsumura T (2002) A comparative study of odontogenic keratocysts associated with and not associated with an impacted mandibular third molar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 94: 272-5.
- Blondeau F, Daniel NG (2007) Extraction of impacted mandibular third molars: postoperative complications and their risk factors. J Can Dent Assoc. 73: 325.
FIGURE 1

Figure 1
FIGURE 2
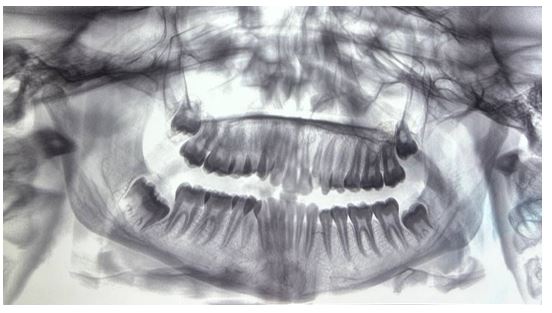
Figure 2
FIGURE 3

Figure 3
FIGURE 4

Figure 4
FIGURE 5

Figure 5
Figures at a glance