Assessment of Exclusive Breast-Feeding Practices Among Human Immune Deficiency Virus Positive Mothers and Determinants in Health Facilities at Akaki-Kality Sub City, Addis Ababa, Ethiopia
Received Date: February 28, 2023 Accepted Date: March 28, 2023 Published Date: April 04, 2023
doi: 10.17303/jfn.2023.9.105
Citation: Leteslassie G tsaddik, Tilahun Bogale (2023) Assessment of Exclusive Breast-Feeding Practices Among Human Immune Deficiency Virus Positive Mothers and Determinants in Health Facilities at Akaki-Kality Sub City, Addis Ababa, Ethiopia. J Food Nutr 9: 1-13
Abstract
Background: Exclusive Breast feeding is low rise of Human Immunodeficiency Virus transmission and lifesaving in setting where diarrhea, pneumonia and under nutrition are common causes of morbidity and mortality among infants and young children. The rate of Exclusive Breast feeding practice in Ethiopia varies across region to region. Hence, this study was aimed to assess Exclusive Breast feeding practices and associated factors in health facilities at Akaki Kality sub city, Addis Ababa.
Objective: To asses Exclusive Breast Feeding practices among Human Immunodeficiency Virus positive mothers and its determinants in health facilities at Akaki Kality sub city, Addis Ababa, Ethiopia, 2021.
MethodsInstitution based cross sectional study design was employed in Akaki kality sub-city. From the total of 11 health facilities in the sub-city by simple random sampling method 4 health facilities were selected. Finally, 255 participants selected by systematic random sampling technique. The data were collected by trained data collectors and supervised by supervisor and investigators. Data were checked for completeness, cleaned and entered into Epi Data version 7 and then exported to SPSS version 25 for further analysis. The association between the dependent and independent variables was analyzed using bivariable and multivariable logistic regression. Finally, P value < 0.05 in multivariable logistic regression model was considered as statistically significant.
Results: The level of current exclusive breastfeeding practice among Human Immunodeficiency Virus positive was found to be 74.9% (95% CI; 69.2, 80.2). Having good knowledge about exclusive breast feeding [AOR = 7.227, 95% CI: (3.766, 13.869)], those with Antenatal care follow up [AOR = 4.828, 95% CI: (2.512, 9.280)] and Postnatal care follow up [AOR = 2.057, 95% CI: (1.085, 3.898)]. Hence, those factors were found to be the significant factors.
Conclusions and Recommendations: This study indicated that majority of the respondents 74.9% had good exclusive breast feeding practice, but still substantial number 25.1% of the respondents had poor exclusive breast feeding practice. On the other hand, knowledge of ANC and PNC follow up were significant factors.
Keywords: Breast Feeding; HIV; Addis Ababa
Abbreviations ANC-Anti Natal Care, ARV-Anti Retro Viral, BF-Brest Feeding, EDHS-Ethiopian Demographic and Health Survey, EBF-Exclusive Breast Feeding, HC-Health Center, HEIs-HIV Exposed Infants, HIV-Human Immunodeficiency Virus, PMTCT-Prevention of Mother to Child Transmission, SSA-Sub Saharan Africa, COR-Crud Odds Ratio, AOR-Adjusted Odds Ratio
Introduction
Breast milk as a source of nutrition is critical to protect newborns and infants against many illnesses and infectious diseases, including reducing the risk of diarrhea, lowering risk of gastrointestinal infections and respiratory infections such as pneumonia, meningitis, neonatal sepsis, ottitis media and allergies which are among the leading causes of infant mortality in low- and middle-income countries. Similarly, breast milk has immunological, psychological, and socioeconomic benefits, better visual acuity, speech and cognitive development and helps for a quicker recovery during illness can also protect the child from atopic eczema, the risk of allergy and asthma, leukemia and decreases the risk of chronic diseases later in life such as obesity and type II diabetes [3,4]. Especially in the first year of the infant’s life, while the absence of breastfeeding during the first 2 months of life is associated with a six-fold increase in child mortality in resource-poor countries due to infectious diseases [5]. In addition, BF contributes to the health and well-being of mothers; it helps to space children, reduces the risk of ovarian cancer and breast cancer, increases family and national resources, is a secure way of feeding and is safe for the environment [6].
In some settings of the sub-Saharan Africa(SSA), it is a customary way of feeding for new born babies and also there is a lower risk of Human Immunodeficiency Virus (HIV) transmission [1,7]. In addition, breastfeeding is lifesaving in settings where diarrhea, pneumonia and under nutrition are common causes of mortality among infants and young children. Along with antiretroviral drugs (ARVs), breastfeeding is part of the strategy for HIV-free survival of children exposed to HIV [8]. Moreover, EBF in the first 6 months of life is known to be the most complete nutrient for a newborn, in that it provides all the energy, vitamins and minerals the baby needs. EBF for up to 6 months is much more effective than mixed feeding at protecting against childhood illness. EBF is also effective in mitigating the burden of non-communicable diseases such as diabetes, asthma and cardiovascular disease in later years [9].
Contrary to the recommendations, different studies shown that the predominant type of breastfeeding for infants less than 6 months of age is mixed feeding [10]. Infants are also feed with other liquids (water 17%, nonmilk liquids 5%, other milk 5%) [11]. In general, the rate of EBF practice is not satisfactory and varies across setting due to enormous barriers and determinants and also low in SSA including Ethiopia [12].
The recommendation for breast feeding among HIV positive mothers has changed over time, according to the revised national Prevention of mother to child transmission of HIV (PMTCT) guideline, mothers known to be HIV should EBF their children for the first 6 month of life [13,14]. Mixed feeding may increase the risk of HIV transmission by 3-4 folds than EBF [15]. Rather than these recommendations, HIV positive mothers have faced the dilemma of either giving their children all the benefits of breast feeding but exposing them to the risk of HIV infection or avoiding all breast feeding and increasing the risk of death from diarrhea & malnutrition [16]. Identifying determinant factors of EBF among HIV positive mothers is important for targeting the education and counseling message to groups of women at risk for shorter BF which helps to increases HIV free survival [14].
Different Studies show that EBF affected by different maternal and child factors. The most and common prevalent factors to EBF includes are mother’s occupation, residence, knowledge on EBF practice, Anti natal care (ANC) service, counseling on EBF practice during ANC visit, insufficient breast milk, husband imposition, mother’s and chilled illness, income, maternal choice of feeding option, culture, family and social pressures, access to mass media [17,18]. Factors at health service level may have resulted in different delivery of feeding messages and support to women living with HIV compared with women not living with HIV [19].
Few studies have been conducted on EBF practice and their factors among HIV positive mothers in Addis Ababa and there is low prevalence of EBF (41.92%).
This study tries to add the knowledge on the observed gap in this area by assessing EBF practice and determinants factors among HIV positive mothers and to update the information
Methods
Study Design, Setting and PeriodFacility based cross sectional study design was conducted in Addis Ababa city, Addis Ababa is the capital city of Ethiopia. It has 11 sub cities. Among these Akaki-Kality sub-city is one of them. According to the 2007 population census the total population of Akaki Kality sub city was 258,030 populations. Of the total population of Akaki kality sub-city, female 131,595 and male 126,435 account. This sub-city has 13 administrative districts and 11 health facilities, 1public hospital, 9 public health centers and 1NGO health center. All public and NGO health facilities were providing ART and PMTCT services. The study was conducted from July, 2021-August 2021
Population and EligibilitySource population were all HIV positive mothers attending PMTCT clinics who had infants of age less than 6 months for follow-up in health facilities which provide PMTCT service in, Addis Ababa city
Study population were all HIV positive mothers attending PMTCT clinics who had infants of age less than 6 months for follow-up in health facilities which provide PMTCT service in Akaki Kality sub city, Addis Ababa. Study Population was all HIV positive mothers who had infants of age lees than 6 months attending at randomly selected health facilities for PMTCT services in Akaki Kality sub city, Addis Ababa. Study Unit/Element were all randomly selected HIV positive mothers who had infants age less than 6 months attending PMTCT services in randomly selected health facilities in Akaki Kality sub city, Addis Ababa.
HIV positive mothers who fulfill the eligibility criteria during the data collection period and willing to give their consent were included. Those HIV positive not fulfill the eligibility criteria during the data collection period were excluded.
Sample Size Determination, Sampling Technique and Sampling ProcedureSample size (n) for first objective was designed using a single population proportion formula considering the following assumptions: (Zα∕2) constant 95% confidence interval, margin of error d (5%), and p = 41.92% (by considering proportion of assumptions of HIV positive mothers who practiced Exclusive breast feeding 41.92% reported by study done national meta-analysis [3].
First, listed all 11 Health facilities, after the listing all health facilities which were providing ART and PMTCT services. This list was used as a sampling frame to randomly select the health facilities. Hence, among the 11 health facilities 4 health facilities were selected namely; Trunesh Bejing hospital, Kality HC, Gelan HC and Saris HC. In the selected health facilities, the HIV positive mothers attending PMCT/ART service and had infants age less than 6 months during the study period obtained from registration book of each health facilities. And then to pick out the study participants a systematic random sampling technique was used. Finally, the study participants were selected by systematic random sampling technique using the same sampling intervals (Kt h). Using the formula k=N/n, which is equal to k=N/n=617/255=2. Therefore, the Kthvalue was 2. Accordingly, mothers attending health facilities for PMTCT services were selected after every 2nd until calculated sample size achieved. And then the study subjects were proportionally allocated for each selected public health facility.
Data Collection ToolsPre-tested and structured questionnaires were used to collect the data. The questionnaires contain variables related to socio-demographic, knowledge, attitude, and practice of mothers on Infant feeding practice and infant feeding options among HIV positive mothers. The questionnaires were prepared in English and translated to Amharic language (local language) by language expert and then re-translated back to English to check for any inconsistencies in the meaning of words. Three data collectors were recruited; 2 Nurses and 1 Heath officer as data collectors and one supervisor. The data collectors and supervisor trained for 1 day on how to interview mothers and how to fill the questionnaires based on prepared instruction/guidelines. During the training, the importance of obtaining the respondents verbal consent and respecting their right to respond or not to respond to any part of the questions were emphasized, in addition to ensuring privacy and confidentiality.
Data Management and AnalysisIn addition to the training given for the data collectors, the questionnaires had been pre-tested before the actual data collection days, which was on 5% of the sample size in health facilities which found in Yeka sub city. Moreover, during data collection supervisor was checking in the field how the data collectors were doing their task. The principal investigator had also closely been supervising the field activity on daily basis. At the end of each data collection day the principal investigator had been also checking the completeness of filled questionnaires and whether recorded information makes sense to ensure the quality of data collected. Besides this, the principal investigator was carefully entering and thoroughly cleans the data before the commencement of the analysis. The coded and cleaned data were entered into Epi info version 7 and then exported to SPSS version 25. After completion of data entering, it was checked and cleaned before analysis. Description of frequency, mean, median, proportion and SD were done and Logistic regression analysis had been carried out. The association between the dependent and independent variables was analyzed using bivariable and multivariable logistic regression. P-value less than 0.2 in bi variable analysis had been entered in to multi variable logistic regression to control confounders.
Finally, p-value < 0.05 in multivariable logistic regression model was considered as statistically significant.
Operational Definitions
Exclusive breast feeding: for the first 6 months of life; that means the infant receives only breast milk including expressed breast milk without any other liquids or solids, not even water and allowed to receive ORS, drops, and syrups (vitamins, minerals, and medicines), but nothing else.
Mixed Feeding: Giving the baby some breast milks an extra food drink
Ethical Consideration
The ethical clearance was obtained from the Institutional Review Board (IRB) of Kotebe Metropolitan University Menelik Medical and Health Science College. Then approval was given by Addis Ababa public health research and emergency management directorate. While written informed consent had been taken from the study Participant ‘s their strict confidentiality was insured and also identity was not being shown and there had been no dissemination of the information without the respondent’s permission. The data given by the participants was used only for research purposes. The names of the participants were omitted.
Results
Socio Demographic and Economic Characteristics of the ParticipantsA total of 255 individuals participated with a response rate of 100%. The mean age of respondents was 30 years with SD of (±5.229) years with the minimum age of 20 and maximum of 43 years. Eighty-two percent (82%) of the participants were married and two hundred nineteen 219 (85.9.5%) of the study population had formal education. The median monthly incomes of the respondents was 5450ETB and sixty-eight 68 (26.7%) of them were house wives. (Table1)
Obstetric History of the participantsFrom all participants one hundred sixty-nine 169 (66.3%) of them attended ANC services during pregnancy of which 46.3% of them had a follow up of 3 times. One hundred sixty-nine (66.3%) of them got counseling services, during their follow up. From those who got counseling services 107(42%) of them were during their ANC visit. About 250(98%) of the participants attended PNC visit. From 98% of those disclosed their HIV status, majority were disclosed from their husband.
Maternal and Child Health Related factors of the ParticipantsThe result showed that two hundred forty 240(94.1%) of the participants had CD4 counts below normal. About one hundred twenty-four 124 (48.6%) of them were in stage one disease progression. From those interviewed 169 (66.3%) of them had encountered breast or other related illness from which 25.1% of them had other type of illness. Only seventy-nine (31%) of them changed the way of feeding their child as a result of illness encountered. Out of One hundred sixty-nine (66.3%) encountered long term illness. Majority of them had problem of TB and hypertension 47.8% and 11% respectively. Concerning infant health one hundred eighty-two (71.4%) of them had encountered any illness of which ninety-one (35.7%) were with problems of diarrheal diseases followed by seventy-five (29.4%) with problems of fever and one hundred sixty-two (89%) of the mothers changed the ways of feeding their infants during their illness.
Knowledge Towards Exclusive Breastfeeding PracticeTwo hundred thirty-nine (93.7%) knew that HIV virus transmits from mother to child during pregnancy and delivery and 13 (6.3%) didn’t know when HIV virus transmits from mother to child. Two hundred twenty-six (88.6%) of them knew breast feeding options recommended for HIV positive mothers and majority 222(87.1%) of them get this knowledge from health care worker during any one of their visit to health facilities. Two hundred eighteen (85.5%) of them had knew breast milk alone is sufficient for first six months of life. But twenty (7.9%) didn’t know as breast milk alone is sufficient and for how long breast milk alone is given. One hundred sixty-nine (66.3%) respondents had good knowledge concerning exclusive breastfeeding practice (table 3).
Exclusive Breast Feeding PracticeTwo hundred forty-two (94.9%) had breastfed their infants. 234 (91.8%) had initiated breastfeeding within one hour of birth and 21 (8.2%) after one hour. No one reported practicing pre-lacteal feeding. Regarding exclusive breastfeeding, 191 (74.9%) of respondents breastfed exclusively for the first 6 months of life. Sixty-four (25.1%) of mothers practiced exclusive replacement feeding. The most common reason cited for practicing exclusive replacement feeding was an illness of the child (66.5%) which was followed by the illness of the mother (20.6%). the most common reason cited for practicing exclusive replacement feeding was thinking that it was safe for infant 175(71.1%) followed by fear of HIV transmission to their infants39(15.9%). (Figure:2).
Binary Logistic regression was performed to assess the association of each independent variable with exclusive breast feeding practice. The factors that showed a p-value of 0.2 and less were added to multivariate regression model. The result revealed that on the bivariate analysis, educational status of the mother, current occupation of the mother, counseling service, knowledge, PNC visit, ANC visit and house hold income were associated with exclusive breast feeding
In multivariate logistic regression to control confounding effect of one variable over the other variable were adjusted. Based on this knowledge, PNC visit and ANC visit were significantly associated with exclusive breast feeding practice at P-value of < 0.05. The odds of respondents with ANC follow up were 4.828 times practicing exclusive breast feeding than those who hadn’t. (AOR=4.828, 95% CI 2.512, 9.280); P=0.0001). Concerning PNC follow up those with PNC follow up were 2.057 times practicing exclusive breast feeding than those with hadn’t. (AOR=2.057, 95% CI 1.085, 3.898); p=0.027). Those participants with a good knowledge had 7.227 times practicing exclusive breast feeding than those with poor knowledge. (AOR=7.227, 95% CI 3.766, 13.869); p=0.0001 (table 4).
Discussion
The study had tried to assess the prevalence of exclusive breast feeding practice and determinant factors of exclusive breast feeding practice. It has shown that exclusive breast feeding was more influenced by having proper knowledge about Exclusive breast feeding, ANC and PNC follow up status of the mothers.
In this study found that 74.9%, with 95% CI (69.2, 80.2) of the mothers’ practiced breast feeding their babies exclusively for 6 months. This finding was similar with that of study done in southern Ethiopia, Northern Ethiopia and EDHS 2016 (24, 25, and 11).
However, this finding was higher than findings reported by studies done in Kenya, Addis Ababa, Southern nation nationality and peoples of Ethiopia and Middle East countries (18, 2, 24 and 18). This difference might be due to the difference in culture of feeding habit, study time as well as the availability of resources to practice exclusive breast feeding and the efforts made by the government in promoting the optimal child feeding practice for HIV infected mothers mainly in the PMTCT, exposed infant, and ART clinics. Might be an improvement health care utilization and knowledge of the mothers about PMTCT is better in this study area than those mentioned above areas.
Multi-variable logistic regression revealed that knowledge of respondents, ANC and PNC follow up had significant association with exclusive breast feeding practice. The odds of exclusive breast feeding practice among HIV-- positive mothers with good knowledge had 7.227 times higher than those who had poor knowledge; AOR; 7.227 (3.766, 13.869). This result was similar to that of studies done in Kenya, Southern, Ethiopia, and Oromia regional state (17, 24, 30 and 31) respectively which showed that mothers with good knowledge had more practicing exclusive breast feeding as compared to those with poor knowledge. This may be due to the fact that mothers who had knowledge about the duration of exclusive breast feeding knew the benefits of exclusive breast feeding for themselves and their infants as well as understand the consequence of not feeding their infants exclusively for the first 6 months of infant life, so they easily adhere to exclusive breast feeding
Conclusion and Recommendations
This study revealed that high proportion of mothers practiced exclusive breastfeeding for the First six months of life. This study also identified several factors associated with EBF practice of HIV positive women. Those mothers with ANC Follow up, Knowledge on EBF and PNC follow were factors significantly associated with EBF practice of HIV positive women.
Policy makersNeed to formulate a multidimensional knowledge change strategy to improve mothers’ knowledge towards exclusive breast feeding with involvement of mothers, family members, and the community at large.
Health Facilities- Strengthening information provided regarding infant feeding options during antenatal and postnatal care.
- Proper Health education and counseling should be given specific to service providing department.
Strength and Limitations of the study
Strength- Achieved 100% response rate
- The study used standardized structured questionnaire
- Face to face interview was used which may increase the validity of the research
Limitations
- The study is conducted in the government health centers administered by Akaki Kaliti sub city only, which didn’t represent the private health facilities.
- Information on EBF feeding bias on recall. So, might not remember the time they introduced extra food and drinks.
Transparency Statement
The leading author LG affirmed that the manuscript is an honest, accurate and transparent account of the study being reported that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been explained.
Data Availability StatementThe original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding authors.
Ethics Statement
The study involving human participants were reviewed and approved by Ethical approval was secured from Addis Ababa public health research and emergency management directorate and then a support letter was submitted to the selected sub-city and respective selected health facilities. The participants provided their written informed consent to participate in the study.
Authors’ Contributions
LG and TB did the conceptualization, data correction and formal analysis. LG involved in drafting writing the proposal and final result. TB was engaged in reviewing, analysis and editing of the manuscript. All authors equally contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to acknowledge Kotebe Metropolitan University, Menelik II College of Medicine and Health Sciences, Adis Ababa Health bureau, Akaki Kality sub-city health department, each health facility, data collectors, supervisor and all study participants.
Conflict of Interest
There is no conflict of interest in this manuscript
- Hazemba AN, Ncama BP, Sithole SL (2016) Promotion of exclusive breastfeeding among HIV-positive mothers: An exploratory qualitative study. Int Breastfeed J [Internet] 11: 1-10.
- Belay GM, Wubneh CA (2019) Infant Feeding Practices of HIV Positive Mothers and Its Association with Counseling and HIV Disclosure Status in Ethiopia: A Systematic Review and Meta-Analysis. AIDS Res Treat.
- Genetu H, Yenit MK, Tariku A (2017) Breastfeeding counseling and support are associated with continuous exclusive breastfeeding from one week to six months of age among HIV exposed infants in north Gondar zone, Ethiopia: A cross-sectional study. Int Breastfeed J 12: 1-8.
- Rutto NK, Onyango RO, Andang’O P, Kishoyian G (2019) Predictors of Exclusive Breast Feeding among HIV-- Positive Mothers in North Rift Region of Western Kenya. Ann Med Health Sci Res 9: 695-705.
- Ngoma-Hazemba A, Ncama BP (2016) Analysis of experiences with exclusive breastfeeding among HIV-positive mothers in Lusaka, Zambia. Glob Health Action 9.
- Earsido A, Abebe W, Dereje N (2017) Prevalence and Determinants of Exclusive Breastfeeding Practices among Infants in Hossana Town, Southern Ethiopia: A Community Based Cross-Sectional Study. EC Gynaecol [Internet] 4: 69-79.
- Aishat U, David D, Olufunmilayo F (2015) Exclusive breastfeeding and HIV/AIDS: A crossectional survey of mothers attending prevention of mother-to-child transmission of HIV clinics in southwestern Nigeria. Pan Afr Med J 21.
- WHO, UNICEF. HIV and Infant Feeding in Emergencies: Operational Guidance [Internet] 1-52.
- Behzadifar M, Saki M, Behzadifar M, Mardani M, Yari F, Ebrahimzadeh F et al. (2019) Prevalence of exclusive breastfeeding practice in the first six months of life and its determinants in Iran: A systematic review and meta-analysis. BMC Pediatr 19: 1-10.
- West NS, Schwartz SR, Yende N, Schwartz SJ, Parmley L et al. (2019) Infant feeding by South African mothers living with HIV: Implications for future training of health care workers and the need for consistent counseling 11 Medical and Health Sciences 1117 Public Health and Health Services. Int Breastfeed J 14: 1-7.
- Central Statistical Agency Addis Ababa EI (2016) Demographic health survy Ethiopia.
- Mihret MS, Asaye MM, Mengistu BA, Belete H (2020) Mixed Infant Feeding Practice and Associated Factors among HIV-Positive Women under Care in Gondar City’s Public Health Facilities within Two Years Postpartum: A Cross-Sectional Study. Int J Pediatr (United Kingdom).
- Igbokwe L, Aniwada E, Uleanya N, Adinma E (2016) Factors that Influence Infant Feeding Options of HIV-Positive Mothers in Urban and Rural Communities in SouthEast, Nigeria. Br J Med Med Res 15: 1-10.
- Republic FD (2015) Federal Democratic Republic of Ethiopia Ministry of Health NATIONAL MENTAL 6.
- Hiv UON, Feeding I (2016) Updates on Hiv and Guideline.
- Ikeako L, Ezegwui H, Nwafor M, Nwogu-Ikojo E, Okeke T (2015) Infant Feeding Practices among HIV-Positive Women in Enugu, Nigeria. Br J Med Med Res 8: 61-8.
- Odeny BM, Pfeiffer J, Farquhar C, Igonya EK, Gatuguta A et al. (2016) The Stigma of Exclusive Breastfeeding among Both HIV-Positive and HIV-Negative Women in Nairobi, Kenya. Breastfeed Med 11: 252-8.
- Andare N, Ochola S, Chege P (2019) Determinants of infant feeding practices among mothers living with HIV attending prevention of mother to child transmission Clinic at Kiambu Level 4 hospital, Kenya: A cross-sectional study. Nutr J 18: 1-8.
- Yapa HM, Drayne R, Klein N, De Neve JW, Petoumenos K et al. (2020) Infant feeding knowledge and practice vary by maternal HIV status: A nested cohort study in rural South Africa. Int Breastfeed J 15: 1-10.
- Investigator NOF, Advisors NOF, Title F, The OF, Tadesse F (2018) Addis Ababa University College of Health Sciences, Department of Nursing and Midwifery.
- Mebratu L, Mengesha S, Tegene Y, Alano A, Toma A (2020) Exclusive Breast-Feeding Practice and Associated Factors among HIV-Positive Mothers in Governmental Health Facilities, Southern Ethiopia. J Nutr Metab.
- Girma YB, Minda A (2020) Determinants of Exclusive Breast Feeding Practice among HIV Positive Mothers in North East Ethiopia: A mixed method study 1-22.
- Ejara D, Mulualem D, Gebremedhin S (2018) Inappropriate infant feeding practices of HIV-positive mothers attending PMTCT services in Oromia regional state, Ethiopia: A cross-sectional study. Int Breastfeed J 13: 1-10.
- 24Eshetu Modjo K (2015) Attitude and Practice Towards Exclusive Breast Feeding and Its Associated Factors Among HIV Positive Mothers in Southern Ethiopia. Am J Heal Res 3: 105.
FIGURE 1
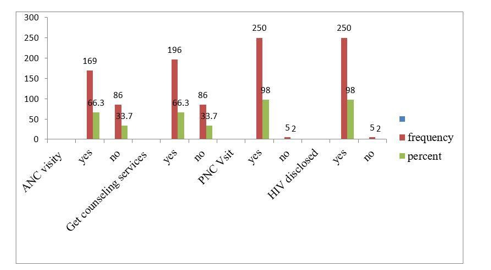
Figure 1: Obstetric History of the study participants found in health facilities of Akaki Sub city Addis Ababa, Ethiopia, 2021
FIGURE 2
Figure 2: Exclusive breast feeding practice of participants found in Akaki Kality sub city, Addis Ababa, Ethiopia, 2021
Tables at a glance
Figures at a glance