Contraceptives Rights and use in Selected Africa Countries: The Role of Social Cultural Determinants
Received Date: August 12, 2024 Accepted Date: September 12, 2024 Published Date: September 15, 2024
doi: 10.17303/jfsrh.2024.1.104
Citation: Sunmola Kazeem Adebayo, Abatan Sunday Matthew, Solanke Bola Luqman,Adeusi Temitope Joshua, Olaosebikan Johnson Sogo (2024) Contraceptives Rights and use in Selected Africa Countries: The Role of Social Cultural Determinants. J Fertil Steril Reprod Health 3: 1-12
Abstract
Despite the rights of women of reproductive age to contraceptive use, the fertility rate in low-and middle-income countries (LMICs) remains high due to the low use of contraceptive use when compared with the more technically advanced countries. This paper therefore, seeks to provide answer to what the prevalence of contraceptive rights and usage among women of reproductive ages is? Also, what are the socio-cultural factors influencing contraceptive use in four sub-Saharan Africa countries? Data on contraceptive use and the associated factors were purposively extracted for analysis from four LMICs countries (Nigeria, Cameroon, Mali, and Zambia) with the most recent Demographic and Health Survey. A total number of 79,550 respondents were pooled from the selected sub-Saharan Africa countries comprising of Nigeria (41,821), Cameroon (13,527), Mali (10,519) and Zambia (13,683). The study found that the women autonomy on the use of contraceptives is very low in the selected SSA countries. The proportion was as low as 15% in Zambia to 26% in Cameroon and 38% in Mali; the proportion of women using contraceptives among the selected countries ranges from 14% from Nigeria, Mali (16%), and Cameroon (20%) to 37% from Zambia. Again, except for Mali, couples who jointly decided on not using contraceptive was more than those who personally decide or whose spouses decided never to use. The study further noted that religion, place of residence, and older women were associated with lower odds of contraception while younger women, education, to tal children ever born, and wealth status are significantly related to higher use of contraception. Furthermore, women aged 20-29 were almost two times (OR= 1.59, p < 0.05, CI: 1.47-1.72) likely to use contraceptive use when compared with women below 20 years. The study concludes that the role of religion and cultural beliefs to stabilize fertility through contraceptives is critical in this part of the world. This study recommends that government and religious leaders need to do more on awareness campaigns and sensitization on the reproductive health benefits of small family size on both mother and child. By implication, for Africa to reap the benefits of demographic dividends, cultural norms and values placed on large family sizes and preferences for the male child should be discouraged.
Keywords: Contraceptive Use; Socio-Economic Inequalities; Low-And Middle-Income Countries
Introduction
There are about 1.1 billion people in Sub-Saharan Africa and this figure has been projected to double by 2050 but resources remain sparse [1]. The figure puts sub-Sahara Africa as the highest in terms of population growth globally [2]. More so, the Total Fertility Rate (TFR) in Sub-Saharan Africa countries remains high as a result of the low uptake of contraceptive use despite the right of women to contraceptive usage. Most of the women in countries in SSA had a fertility rate of more than five children, a fertility rate of 7.6 was reported in Niger, 8.2 in Chad, 6 in Burkina Faso, 6.1 in Mali [3], and 5.3 in Nigeria [4]. More so, estimates showed that on average, births per woman were about 4.8 in SSA as against 3.3 in Arab nations; 2.5 in South Asia, 2.1 in Latin America and the Caribbean, and 1.6 in European Union [3].
Prevalence of contraceptive use among married or related women of reproductive age is approximately 22% in SSA versus 86% in East Asia and 72% in Latin America and the Caribbean [3]. Contraception (CPT) was defined as "the prevention of pregnancy by interfering with the standard process of ovulation, fertilization, and implantation". It is "the intentional use of artificial methods or other techniques to prevent pregnancy as a result of sexual intercourse” [5]. Hence Contraceptives help women to prevent unwanted pregnancies while enjoying healthy sexual relationships [6,7]. Some of the contraceptives are vaginal methods (foam, jelly, and suppository), condom, Lactational Amenorrhea Method (LAM), Intra-Uterine Device (IUD), standard day method (SDM), contraceptive pills, injectable, implants and vasectomy, contraceptive pill, and emergency contraception among others [8,9].
Previous studies revealed that contraceptive use is of social and public health importance that demands urgent attention because of the perceived challenges associated with non-usage for the individual, family, and society [2,10,11]. The observed consequences are unintended pregnancies and unsafe abortion [9]. Unsafe abortions continue to be a problem among young women in SSA because of other factors such as ignorance/illiteracy, religion [12,13]. Other factors such as the cultural, structural, legal, and weak public health systems that limits access to family planning services [14]. Contraceptive uptake can reduce maternal deaths from 308, 000 to 84,000 and new born death from 2.7 million to 538,000 per year respectively [15]. Contraceptive use plays a significant role in reducing Total Fertility Rates (TFR) as such countries majorly depend on its use for birth control measures [16].
About 220 million women in Low and Middle-Income Countries (LMICs) have been estimated to have an unmet need for contraception [17]. In Sub-Saharan Africa, the rate of contraceptive use of 17% had been reported among women of reproductive age [18]. At the country level, contraceptive use among women in Ghana was reported to be 27% [16] and 15% in Nigeria [19]. The prevalence of 52% was reported in Eswatini and Namibia each, 4% in Sudan [20], and 51% in Ethiopia [21]. The prevalence of 8% was reported in Niger, 5.4% in Chad, 15% in Burkina Faso, and 10%in Mali [3]. The unmet need for contraceptives in Ghana was 15%, Botswana, 9.6% among married women [22], and 19% in Nigeria [23].
However, there is a variation from country to country because of many factors such as illiteracy, religion, education [24]. Other determinants of the use of contraceptives include family composition, myths about contraceptive side effects, employment, male partner disapproval, communication with male partners, and social/cultural factors [25]. Contrary to women who make decisions about their own sexual health, women who had the prior conversation with their spouses are more likely to utilize contraception. Also, the number of surviving children, marital status, location and geographic area of residence, religious affiliation, and women's autonomy is significantly related to contraceptive use [26]. The relationship between exposure to mass media, knowledge of contraceptive methods, and parity and utilization of contraceptives had been established [27,28].
In SSA, the decision making power lies on the man, there is poor access to material resources to seek family planning services and the use of contraceptives is often strongly influenced by spousal or familial support of, or opposition to family planning [29,30]. However, the consistent and correct use of contraceptives is a cost-effective method to improve the maternal, child and socioeconomic status of people the world over. This is why sustainable development goals 2030 calls for increased attention to ensure universal access to sexual and reproductive healthcare services and utilization of contraceptives [14]. This paper, therefore, aims at examining the prevalence of contraceptive use. It also aims to determine the associated socio-economic differentials, cultural and religious factors influencing the low uptake of contraceptive use in the selected sub-Saharan Africa countries.
Theoretical Perspective
Many theories and models ranging from social learning theory to theory of planned behaviour had previously been adopted by scholars to explain the nexus between socio-cultural factors and contraceptive use [31,32]. However, this paper adopted the Health Belief Model (HBM) because it is a "well-tested and comprehensive social cognitive model [33]” that attempted to explain and predict health-related behaviours change, especially regarding the uptake of health-related services such as contraceptive uptake [34,35]. The theory opined that the “beliefs of people about their health status, the perceived benefits of action and barriers to action, and self-efficacy predict their engagement or not in health-promoting behaviour". Also, the presence of stimulus or cue to action helps to initiate the healthpromoting behaviour [34].
Not only that HBM does not account for other factors that influence health-related behaviours such smoking but also does not take cognizance of non-health related behaviours like exercising for aesthetic reasons [36]. More so, HBM does not consider the impact of emotions on healthrelated behaviour [37]. However, the model is very relevant and has been employed in developing the frameworks for contraceptive use and uptake globally [2,32,35].
Figure 1 below shows the link between individual’s socio-demographic variables (such as age, education, religion, children ever born, residence and wealth index) and contraceptive use.
Materials and Methods
Research Design
This study employed a cross-sectional research design. This study employed secondary data sources of four sub-Saharan Africa countries namely Nigeria, Cameroon, Mali, and Zambia (CDHS-2018, MDHS-2018, NDHS-2018, & ZDHS-2018).
Study Population
The study population includes all women of reproductive age 15-49 years who were using contraceptive use or not during the period under review.
Sampling Strategy
The data of selected countries were purposively pooled for the analysis based on the countries with the most recent Demographic and Health Survey (2018). The population sizes of the selected sub-Saharan countries differ – Nigeria (41,821), Cameroon (13,527), Mali (10,519), and Zambia (13,683).
Definitions of Variables
The following variables have been contextualized for the purpose of this study:
a. Contraceptive rights: Contraceptive rights in this study simply implies that women has equal power to access contraceptives
b. Contraceptive use: Contraceptive use means the use of contraceptives by women
c. Socio-cultural determinants: These are variables which can influence the rights and use of contraceptives among women of childbearing ages. This study is limited to socio-cultural factors such as age, education, religion, Children Ever Born (CEB), residence and wealth index. Age of respondents who were using contraceptives or not ranges from 15-49 years; education of respondents include those with no education, primary, secondary and higher education; religion of respondents include Christians, Islam and those into other religion; Children Ever Born means the number of children the respondents had ever given birth to. This ranges from those with no child to those with three or more children. Residence is categorized as respondents who either lived in the rural or urban areas. Wealth index was categorized into those who were either poor, rich or fall in between the poor and the rich.
Analytical Strategy
Both descriptive and inferential statistics were employed to address the study objectives. Bar chart was used to describe the prevalence of contraceptive rights and use in the selected countries. Also, binary logistic regression was employed to establish the relationship between the socio-- cultural determinants and dichotomous dependent variable (contraceptive use). Dependent variable was measured as: (“1” = contraceptive use, “0” = non-use of contraceptive). Stata statistical software version 14 was used to analyze the data. The result of the study was significant at p < 0.001.
Results
Prevalence of Contraceptive Use among Married Women in sub-Saharan Africa
According to Table 1, only a small percentage of women in the selected countries have access to and utilize contraceptives. Contraceptive usage decisions varied from 15.1% in Zambia to 23.3% in Nigeria, 26.3% in Cameroon, and 38.3% in Mali, while usage rates were found to be as low as 14.3% in Mali, 16.2% in Cameroon, 19.5% in Zambia, and 24.3% in Mali. The socio-cultural factors as well as the patriarchal nature of Africa society seem to be largely responsible for the low uptake of contraceptives. These reflect in figure 2 as majority of respondents across selected countries revealed that decision why they are not using was taken by husbands/others or jointly taken by spouse.
Figure 3 above shows the percentage distribution of respondents by decision on not using contraceptives among married women of childbearing ages. The graph reveals that the joint decisions by spouse never to use contraceptives were more predominant in Nigeria (42%), Cameroon (37%) and Zambia (57%). Conversely, only Mali (15.3%) had the least proportion of spouses who jointly decided not to use contraceptives.
Table 2 below shows there is a significant relationship between all the socio-demographic characteristics of married women and contraceptive rights and use. The study further noted that religion, place of residence, and older women were associated with lower odds of contraception while younger women, education, total children ever born, and wealth status are significantly related to higher use of contraception. Furthermore, women aged 20-29 were almost 2 times (OR= 1.59, p < 0.05, CI: 1.47-1.72) likely to use contraceptive use when compared with women below 20 years.
It was also found from the study that women with higher education were 4 times more likely to use contraceptive use than those with no formal education (OR=4.23, p < 0.05, CI: 3.89-4.60). Religion was another socio-demographic variable considered in this study. The result shows that women who were Islam were less likely to use contraceptive use when compared with the Christians (OR=0.40, p < 0.01, CI: 0.38-0.42). Moreover, women who have had three children or more were almost 6 times more likely to use a contraceptive than those with no child (OR: 5.86, p < 0.05, CI: 5.42-6.34).
The study was limited to four selected sub-Saharan Africa countries (Nigeria, Cameroon, Mali and Zambia) with most recent survey data (2018 Demographic and Health Survey). Nevertheless, the findings of this study can be used by the governments of the selected countries for appropriate decision making and intervention program and policy such as sensitization awareness and empowering women with right information about the health benefits of contraceptives use on both mothers and children. By extension, ensuring that the selected sub-Sahara Africa reap and optimize the benefits of demographic dividend.
Discussion
Level of Contraceptive Rights and Use in Selected Countries
This study established a low contraceptive rights and low across the four selected countries. The patriarchal many societies in Africa nations seem to largely account for this. Women are expected to submit to the authorities of their husbands while men exercise control over their wives in whatever they do including their reproductive health issues. Another likely reason for the low rights and use of contraceptives in SSA countries is the love for having many children. It is believed that the more the number of living children, the more likely their old age is secured. More so, there seems to be low uptake of contraceptive use in the selected sub-Sahara countries because of the perceived beliefs or myths of women towards the use of contraceptives. Most women, particularly in developing countries such as Africa belief that contraceptive use can result to infertility whenever they desire to have children. Another misconception for low contraceptive use was the likelihood of developing non-- communicable diseases such as cancer or obesity among others. The above reasons for the low contraceptive use in the selected SSA countries can be likened to Health Belief Model (HBM). The model emphasized that beliefs of people about their health status, the perceived benefits of action and barriers to action, and self-efficacy predict their engagement or not in health-promoting behaviour.
This finding corroborates the result of Maiga et al., (2015) and [29] who opined that the decision to access and to seek the use of contraceptives rests on the husbands. In Africa society, even though women have the right to contraceptive use, they still submit to the wishes and authorities of their husbands. By implication, the issue of gender inequality which is often caused by patriarchal nature of SSA countries remain public health concerns which require urgent attention if SSA countries must achieve Sustainable Development Goals 2030.
Apart from that, society encourages large family sizes and the preference for a male child is high. All these factors among others are largely responsible for the low uptake of contraceptives among women in Africa. The finding from this study corroborated with the study of other researchers who submitted a low contraceptive use as a result of a preference for large family sizes in sub-Saharan Africa when compared with the other regions such as East Asia, Latin America, and the Caribbean [3].
The West African countries with the least use of contraceptives include Nigeria and Mali. This seems to account for the reason why West Africa is more densely populated when compared with other regions in Africa such as East Africa (Zambia) and Central Africa (Cameroon). Of all the selected sub-Saharan Africa, Zambia contraceptive rights and use are relatively higher. The likely reason why contraceptive rights and use in Zambia is relatively higher could be as a result of the effort of the Government of the Republic of Zambia to increase the contraceptive prevalence rate for methods from 33% in 2007 to 58% by 2020 [38].
Socio-cultural Determinants of Contraceptive Use in selected sub-Saharan Africa
This study found that women aged 20-29 years are more likely to use contraceptives. The likely reason for this could be that they are at the peak of sexual behavior where the urge for sex is high. Again, these are the population group who are expected to be in school. Hence, they are likely to prevent the occurrence of unwanted pregnancies. More educated women seem to be more likely to use contraceptives because of their exposure to sex education on the implication of unsafe sex which includes but are not limited to STDs including HIV/AIDS. This study corroborates the findings of [43] who opined that educated women were more likely to use a method of contraceptives in SSA. On the contrary to the finding of this research, [39] in their study found that education did not change the use of contraceptives among women in SSA.
Moreover, women who were Islam seem to be less likely when it comes to contraceptive use. Religious beliefs and practices of large family size and polygamy among African Muslims seem to account for this result. The findings of this study are similar to that of [26] who opined a significant relationship between the number of surviving children, marital status, geographic area of residence, religious affiliation as well as women's autonomy in contraceptive use.
On the children ever born, women who had a minimum of three children are more likely to use contraceptives. The possibility for this could be that the women were through with childbearing. Hence, they had to prevent themselves from having an unwanted pregnancy. The findings of [40] study revealed that, among other factors, gender norms, demographics, and fertility norms had a major impact on the usage of contraception in African countries. Other researchers such as [41] also submitted that contraceptive use among fecund women of childbearing age is significantly associated with contraceptive uptake.
Women from wealthy backgrounds predominantly use contraceptives more than poor women. The reason is that they are likely to be more educated and possibly incur more on their children on education and other standards of living more than the less privileged women. This consequently could encourage women to curtail the number of children by increasing the use of contraceptives. The finding of this study is in line with the result of [42] who found women in the highest wealth quintile were more likely to use contraceptives than those with the lowest wealth quintile.
The finding of this study is rooted in the Health Belief Model. The model established the link between individual socio-demographic factors (age, education, wealth index, religion, and place of residence among others), perceived benefits of contraceptive use and the willingness to use modern contraceptive. The theory also emphasized on the connections between individual socio-demographic factors, subjective norms towards contraceptives and the willingness to use contraceptives. Perceived efficacy to use contraceptives was also noted by HBM to greatly influence willingness to use modern contraceptives.
By implication, enhancing the poor socio-economic status of women, those who live in the rural area and women with middle wealth quintile is fundamental to eradicating low contraceptive rights and use in sub-Saharan Africa.
Conclusions
The role of religion and cultural beliefs to stabilize fertility through contraceptives is critical in this part of the world. Again, the selected sub-Saharan Africa has relatively low contraceptive rights and use. Furthermore, socio-demographic attributes of women in the selected sub-Saharan Africa are great factors influencing contraceptive rights and use.
Recommendations
Based on the findings from the study on the low contraceptive use among married women in sub-Saharan Africa, the following recommendations are made:
Government and religious leaders need to do more on awareness campaigns and sensitization on the reproductive health benefits of small family size on both mother and child.
For Africa to reap the benefits of demographic dividends, cultural norms and values placed on large family sizes and preferences for the male child should be discouraged.
There is need to reduce gender inequalities among couples in the aspect of reproductive decision like contraceptive should be upheld.
Acknowledgements
The research was conceptualized by SKA. The literautre review was conducted by SKA, ASM ATJ and SBL. Methodology was done by SKA, SBL and ATJ. Analysis was done by SKA, ASM, SBL and OJS. SKA, ASM, SBL, ATJ and OJS wrote the article. SKA provided supervision.
- World Population Review (2021). High income countries 2020.
- Fagbamigbe A (2021). How soon does modern contraceptive use starts after sexual debut in Africa? Survival analysis of timing and associated factors among Never-In-Union Women. Scientific African, e00719.
- Atake EH, Ali PG (2019) Women’s empowerment and fertility preferences in high fertility countries in Sub-Saharan Africa. BMC women’s health 19: 1-14.
- Sunmola K, Olaosebikan J, Adeusi T (2021) Determinants of Disparity in Desired Fertility among Married Women in Urban and Rural Areas of Southwest Nigeria. European Journal of Health Sciences 6: 48-63.
- Jain R, Muralidhar S (2011) Contraceptive methods: needs, options and utilization. The Journal of Obstetrics and Gynecology of India 61: 626-34.
- Durowade KA, Omokanye LO, Elegbede OE, Adetokunbo S, Olomofe CO, Ajiboye AD, et al. (2017) Barriers to contraceptive uptake among women of reproductive age in a semi-urban community of Ekiti State, Southwest Nigeria. Ethiopian journal of health sciences 27: 121-8.
- Ngozi AI, Lynda UN (2020) Low Contraceptive Use in Nigeria and its Implications for Population Growth and Sustainable Development. The Nigerian Journal of Medical Sociology 2.
- Aviisah PA, Dery S, Atsu BK, Yawson A, Alotaibi RM, Rezk HR, et al. (2018) Modern contraceptive use among women of reproductive age in Ghana: analysis of the 2003–2014 Ghana demographic and health surveys. BMC women’s health 18: 1-10.
- Iyanda AE, Dinkins BJ, Osayomi T, Adeusi TJ, Lu Y, Oppong JR (2020) Fertility knowledge, contraceptive use and unintentional pregnancy in 29 African countries: a cross-sectional study. International journal of public health 65: 445-55.
- Blackstone SR, Nwaozuru U, Iwelunmor J (2017) Factors influencing contraceptive use in sub-Saharan Africa: a systematic review. International quarterly of community health education 37: 79-91.
- Ahinkorah BO (2020) Predictors of modern contraceptive use among adolescent girls and young women in sub- -Saharan Africa: a mixed effects multilevel analysis of data from 29 demographic and health surveys. Contraception and reproductive medicine 5: 1-12.
- Getahun GK, Kidane M, Fekade W, Shitemaw T, Negash Z (2023) Exploring the reasons for unsafe abortion among women in the reproductive age group in western Ethiopia. Clinical Epidemiology and Global Health 22: 101301.
- Nyachwaya NS, Mwanzo I, Osur J (2023) Predictors of unsafe abortion among women seeking postabortion care at the Nakuru County Referral Hospital, Nakuru County Kenya. International Academic Journal of Health, Medicine and Nursing 2: 292-313.
- Ahinkorah BO, Budu E, Aboagye RG, Agbaglo E, Arthur-Holmes F, Adu C et al. (2021) Factors associated with modern contraceptive use among women with no fertility intention in sub-Saharan Africa: evidence from cross-sectional surveys of 29 countries. Contraception and Reproductive Medicine 6: 1-13.
- Darroch JE, Sully E, Biddlecom A (2017) Adding it up: investing in contraception and maternal and newborn health, 2017-supplementary tables. New York, NY: The Guttmacher Institute.
- Abdulai M, Kenu E, Ameme D, Bandoh D, Tabong P, Lartey A, et al. (2020) Demographic and socio-cultural factors influencing contraceptive uptake among women of reproductive age in Tamale Metropolis, Northern Region, Ghana. Ghana Medical Journal 54: 64-72.
- Belda SS, Haile MT, Melku AT, Tololu AK (2017) Modern contraceptive utilization and associated factors among married pastoralist women in Bale eco-region, Bale Zone, South East Ethiopia. BMC health services research 17: 1-12.
- Ba DM, Ssentongo P, Agbese E, Kjerulff KH (2019) Prevalence and predictors of contraceptive use among women of reproductive age in 17 sub-Saharan African countries: a large population-based study. Sexual & Reproductive Healthcare 21: 26-32.
- Iheyinwa CS, Oladosu M (2016) Socio-demographic factors, contraceptive use and fertility preference among married women in South-South Region of Nigeria.
- DESA U (2019) Family Planning and the 2030 Agenda for Sustainable Development: Data Booklet. ST/ESA/SER. A/429). United Nations, Department of Economic and Social.
- Asresie MB, Fekadu GA, Dagnew GW (2020a) Contraceptive use among women with no fertility intention in Ethiopia. Plos one 15: e0234474.
- Wulifan JK, Mazalale J, Kambala C, Angko W, Asante J, Kpinpuo S, et al. (2019) Prevalence and determinants of unmet need for family planning among married women in Ghana-a multinomial logistic regression analysis of the GDHS, 2014. Contraception and reproductive medicine 4: 1-14.
- Olaosebikan J, SUNMOLA KA, Adeusi T (2021) Socio-demographic Characteristics, CEB and Contraceptive Use among Women of Childbearing Age in Southwest Nigeria. American Journal of Humanities and Social Sciences Research 5: 277-84
- Stonehill A, Bishu SG, Taddese HB (2020) Factors associated with long-acting and short-acting reversible contraceptive use in Ethiopia: an analysis of the 2016 Demographic and Health Survey. The European Journal of Contraception & Reproductive Health Care 25: 350-8.
- Odimegwu, C. O., and Adewoyin, Y. (2021). Latent and Under-explored Determinants of Contraceptive Use in Nigeria. Sexuality Research and Social Policy 18, 715–725.
- Nketiah-Amponsah E, Arthur E, Abuosi A (2012) Correlates of contraceptive use among Ghanaian women of reproductive age (15-49 years). African journal of reproductive health 16: 154-69.
- Ochako R, Mbondo M, Aloo S, Kaimenyi S, Thompson R, Temmerman M, et al. (2015) Barriers to modern contraceptive methods uptake among young women in Kenya: a qualitative study. BMC public health 15: 1-9.
- Debebe S, Limenih MA, Biadgo B (2017) Modern contraceptive methods utilization and associated factors among reproductive aged women in rural Dembia District, northwest Ethiopia: Community based cross-sectional study. International Journal of Reproductive BioMedicine 15: 367.
- Mohammed A, Woldeyohannes D, Feleke A, Megabiaw B (2014) Determinants of modern contraceptive utilization among married women of reproductive age group in North Shoa Zone, Amhara Region, Ethiopia. Reproductive health 11: 1-7.
- Maïga A, Hounton S, Amouzou A, Akinyemi A, Shiferaw S, Baya B, et al. (2015) Trends and patterns of modern contraceptive use and relationships with high-risk births and child mortality in Burkina Faso. Global health action 8: 29736
- Montgomery MR, Casterline JB (1996) Social learning, social influence, and new models of fertility. Population and development review 22: 151-75.
- Kiene SM, Hopwood S, Lule H, Wanyenze RK (2014) An empirical test of the Theory of Planned Behaviour applied to contraceptive use in rural Uganda. Journal of health psychology 19: 1564-75
- Hall, K. S. (2012). The health belief model can guide modern contraceptive behavior research and practice. Journal of midwifery & women’s health 57: 74-81.
- Rosenstock IM (1974) The health belief model and preventive health behavior. Health education monographs 2: 354-86.
- Kahsay ZH, Tegegne D, Mohammed E, Kiros G (2018) Application of individual behavioral models to predict willingness to use modern contraceptives among pastoralist women in Afar region, Northern Ethiopia. PloS one 13: e0197366.
- Janz NK, Becker MH (1984) The health belief model: A decade later. Health education quarterly 11: 1-47.
- Glanz K, Rimer BK, Viswanath K (2015) Health behavior: Theory, research, and practice. John Wiley & Sons
- Republic of Zambia G (2013) Family Planning Services: Integrated Family Planning Scale-up Plan 2013–2020. 2013. Ministry of Community Development Mother and Child Health: Lusaka, Zambia, 1-181.
- Emina JB, Chirwa T, Kandala NB (2014) Trend in the use of modern contraception in sub-Saharan Africa: does women’s education matter? Contraception 90: 154-61.
- Elfstrom KM, Stephenson R (2012) The role of place in shaping contraceptive use among women in Africa. PloS one 7: e40670.
- Asresie MB, Fekadu GA, Dagnew GW (2020b) Contraceptive use among women with no fertility intention in Ethiopia. Plos one 15: e0234474.
- Adebowale SA, Adedini SA, Ibisomi LD, Palamuleni ME (2014) Differential effect of wealth quintile on modern contraceptive use and fertility: evidence from Malawian women. BMC women’s health 14: 1-13.
- Stanfors M, Larsson C (2014) Women’s education, empowerment, and contraceptive use in sub-Saharan Africa: findings from recent demographic and health surveys. Etude de la Population Africaine 28: 1022-34.
- Central Statistical Office (CSO) [Zambia], Ministry of Health (MoH) [Zambia], and ICF International. Zambia Demographic and Health Survey 2013-14. Rockville, Maryland, USA: Central Statistical Office, Ministry of Health, and ICF International; 2014.
- Institut National de la Statistique (INSTAT) and ICF. (2019). 2018 Mali demographic and health survey Datasets.
- National Institute of Statistics (INS) and ICF. Cameroon Demographic and Health Survey 2018.
- Yaoundé, Cameroon and Rockville, Maryland, USA: INS and ICF; 2020.
- National Population Commission (NPC) [Nigeria] and ICF (2019). Nigeria Demographic and Health Survey 2018 Key Indicators Report. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF. Nigeria: NPC, ICF.
FIGURE 1
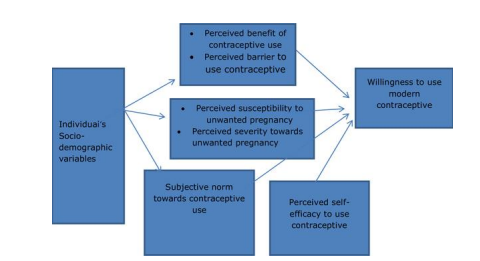
figure:1 Theoretical framework for willingness to use modern contraceptive according to Kahsay et al., 2018
FIGURE 2
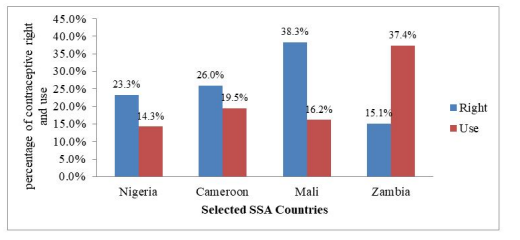
figure:2 Showing the level of Contraceptive Right and Use in Selected Countries
FIGURE 3
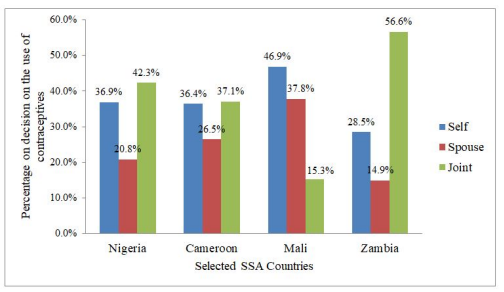
figure:3 Showing the Decision on not Using Contraceptives in Selected Countries
Tables at a glance
Figures at a glance