Ambulatory Blood Pressure Monitoring and its Importance in the Management of Diabetic Patients
Received Date: January 06, 2025 Accepted Date: January 20, 2025 Published Date: January 25, 2025
doi: 10.17303/jhhi.2025.1.101
Citation: Francisco Villalba Alcala, Ana Belen Romero Cañadillas (2025) Ambulatory Blood Pressure Monitoring and its Importance in the Management of Diabetic Patients. J Hypertens Health Impacts 1: 1-12
Abstract
Numerous independent studies have shown that the average BP during Sleep is a better marker of CV risk than clinical BP and activity measures or of 24 hours derived from the ABPM. The prevalence of an altered circadian BP pattern and nocturnal hypertension is very high in patients with diabetes, so in these patients, the diagnosis of hypertension and its therapeutic control are frequently inadequate in the absence of 24-h BP assessment using ABPM. For all these reasons, ABPM should be the tool of choice in patients with diabetes for the correct diagnosis of hypertension and to establish the scheme most appropriate therapeutic that allows the control of elevated nocturnal BP, which could result in a significant reduction in CV events.
Keywords: Diabetic Patients; Ambulatory Blood Pressure Monitoring; Arterial hypertension; Acute Myocardial Infarction;Cardiovascular
Acronyms and Abbreviations
ABPM = Ambulatory Blood Pressure Monitoring; HTA = Arterial hypertension; BP = Blood pressure; AMI = Acute Myocardial Infarction; CV = Cardiovascular; SBP = Systolic blood pressure; DBP = Diastolic blood pressure; PP = PulsePressure; ACEI = Angiotensin-converting enzyme inhibitor; ARA II = Angiotensin II receptor antagonists; RAAS = Renin Angiotensin Aldosterone System; HR = Heart Rate; HR = Hazard Ratio; AMPA = Self-Measurement of Blood Pressure; CVD = Cardiovascular Disease; CKD = Chronic Kidney Disease; ACV = Cerebrovascular Accidents; IMC = Body Mass Index
Introduction
The concept of cardiovascular risk factor comes from the 1960s. Between 1930 and 1950, studies began to be published in which it was observed that People who suffered from Acute Myocardial Infarction (AMI) were preferably men and had a higher cholesterol concentration and blood pressure higher than those who did not suffer from it. However, given the case-control design of these studies, no unequivocal causal relationships could be established. This motivated the setting the first large prospective study, the Framingham study, which began in 1948 with the recruitment of more than 4,000 men and women between 39 and 59 years old. The first analysis was carried out in 1957, after 4 years of complete follow-up of 90% of the included population, and demonstrated that the occurrence of coronary heart disease was more common in men and was favored by the presence of high blood pressure (HTA), obesity and hypercholesterolemia. Smoking should have waited a second analysis of the data, which was carried out 2 years later, to demonstrate their association with cardiovascular disease. These predictor variables of AMI were I would call risk factors [1,2]. Based on successive analyzes of the data. From the Framingham study, more risk factors were identified such as diabetes, which later demonstrated its unequivocal association with cardiovascular disease in different populations. These classic factors can divided into modifiable and non-modifiable (Table 1) [3,4].
The Framingham is a prospective population-based study that began in Framingham and that for the last 75 years has allowed researchers collect data on cardiovascular diseases and their predisposing factors. One of the myths that the Framingham study helped debunk was that hypertension. Diastolic blood pressure was more dangerous than systolic blood pressure in terms of cardiovascular risk. In fact, among their conclusions are that systolic HBP has a stronger with coronary disease than diastolic. Two other articles related the Systolic HBP with strokes and heart failure, which did not happen with diastolic HBP Contributed to modifying medical practice, disease treatment cardiovascular disease to work actively on prevention and identification of people at risk. Factors such as hypertension, dyslipidemia, and diabetes increase the risk of suffering a cardiovascular event and are recognized as risk factors. Risk from Kannel's original article in his publication \\"Factors of Risk in the Development of Coronary Heart Disease. Six year follow-up experience. The Framingham study\\", in Annals of Internal Medicine in 1961.
Diabetes has currently become one of the modifiable risk factors most prevalent worldwide and establish the most appropriate therapeutic scheme that allowing BP control is something that is essential.
Development of the Topic
Numerous independent studies have shown that the average rest period (period of sleep) of BP is a better marker of CV risk than conventional clinical BP and then the activity or 24-h averages derived from ABPM [5-7], also in patients with diabetes [8-10]. In general, these studies show that, when analyzed jointly the averages of activity and rest adjusted by variables of significant influences (including sex, age, diabetes, chronic kidney disease, smoking, previous CV event, etc.), only the average of rest, but not the average of activity, It is a significant and independent marker of CV morbidity and mortality. There are new Emerging perspectives on alterations in the circadian pattern of BP in patients with diabetes and its potential normalization through timing (chronotherapy) of antihypertensive treatment at bedtime with the double objective of increase BP control and reduce CV risk [5,8,11,12].
Ambulatory Blood Pressure Pattern in Patients with Diabetes
Patients with diabetes constitute one of the groups of greatest interest when it comes to evaluate the potential of ABPM as a diagnostic tool, due to the strong association between this disease and increased risk of damage to target organs, stroke and CV morbidity and mortality. The no-dipper pattern and nocturnal hypertension, conditions that necessarily require ABPM for diagnosis, are common in diabetes [13-16].
Patients with diabetes constitute one of the groups of greatest interest when it comes to evaluate the potential of ABPM as a diagnostic tool, due to the strong association between this disease and increased risk of damage to target organs, stroke and CV morbidity and mortality. The no-dipper pattern and nocturnal hypertension, conditions that necessarily require ABPM for diagnosis, are common in diabetes [13-16].
Ayala et al. [17] in a prospective and controlled multicenter study investigated the influence of diabetes on the circadian BP profile among patients hypertensive. In patients with diabetes, ambulatory SBP was significantly higher elevated (p < 0.001), mainly during the hours of night rest and early hours of the activity cycle, regardless of the presence/absence of treatment.
Antihypertensive (figure 1, left panel). Ambulatory DBP, however, was significantly lower (p < 0.001) in patients with diabetes, mainly during the hours of daytime activity (figure 1, right panel). As a consequence of these differences in SBP and DBP, ambulatory PP was significantly higher (p < 0.001) in patients with diabetes throughout the 24 hours of the day (Figure 2, right panel). The proportion of patients with a 48-h mean PP >53 mmHg, a threshold associated with increased CV risk [18] was significantly higher in patients with diabetes (63 vs. 34%; p < 0.001). Heart rate was significantly higher during the hours of nocturnal rest and minor during most of the cycle of activity in patients with diabetes than without (figure 2, left panel). The prevalence of the no-dipper pattern was significantly higher in patients with diabetes (62.1 vs. 45.9%; p < 0.001), as has already been recently corroborated [19]. The biggest difference between groups was in the prevalence of the riser pattern (SBP depth < 0.001). The main factor in the diagnosis of hypertension or inadequate BP control in patients with diabetes it was high BP during sleep; thus, 89.2% of hypertensive patients with uncontrolled diabetes had nocturnal hypertension [17].
Additionally, Ayala et al.17 used the data collected from the 12,765 participants in their cross-sectional study to investigate possible influencing factors on the profile nodipper in hypertensive patients. The logistic regression analysis indicated that the profile no-dipper (as a categorical variable) was simultaneously and significantly associated, in order of importance, with reduced estimated glomerular filtration rate, advanced age, presence of diabetes, low HDL-cholesterol, not smoking (due to the expected increase in activity BP associated with the pressor effect of tobacco), low triglycerides, mass index elevated body count and elevated albumin/creatinine ratio (table 2). Furthermore, the pattern no-dipper was significantly associated with increased antihypertensive drugs in single morning dose. These results indicate the strong association between the absence of adequate decrease in BP during sleep (no-dipper pattern) and diabetes, the presence of kidney disease, aging and central obesity.
Effects of the Time of intake of Antihypertensive Drugs
Chronotherapy applied to drugs improves the diagnosis and treatments of diseases by administering drugs according to the biorhythms that dictate the functioning of the human organism, since with this technique (called chronotherapy) we manage to optimize the effectiveness provided by each medication, thus how to advance in the prevention, diagnosis and treatment of pathologies, being able to improve cardiovascular results and reduce this risk.
In general, hypertensive subjects, including patients with diabetes, ingest all your antihypertensive medication in the morning. However, it has been documented that diverse circadian rhythms in physiological and biochemical functions and processes can significantly affect pharmacokinetics (release processes, absorption, distribution, metabolization and elimination) and pharmacodynamics (effects pharmacological) of antihypertensive drugs. Therefore, circadian timing or the timing of drug administration over 24 hours can modify the pharmacokinetics or the therapeutic and adverse effects of drugs [20-22].
Descriptive studies [23,24] and a good number of randomized clinical trials with antihypertensive drugs have documented relevant differences in their effectiveness for reduce BP, duration of action, safety profile and effects on pattern circadian BP that depend on the time of day of its administration (chronotherapy) [20-22]. For example, the monotherapy intake of ACEI or ARA-II at at bedtime, rather than upon rising, reduces BP more during sleep. Sleep without loss of efficiency during active hours, which leads to an increase significant depth towards a more dipper profile. These results, furthermore, are independent of the terminal half-life of the drug (usually calculated only at from studies in which patients were treated in the morning) and appear to be rather related to the activation of the renin-angiotensin-aldosterone system (RAAS) during the second half of the sleep period [25].
Moyá et al. [26] investigated the influence of the time of day (in relation to the cycle of rest/wake of each subject) of antihypertensive treatment on the circadian profile and the degree of control of ambulatory BP, as well as on clinical parameters and analytical tests of interest, in hypertensive patients with diabetes, the results of the study, in First, that patients with diabetes who ingested the full dose of ≥1 antihypertensive drugs at bedtime, compared with those taking all night medication upon waking up, had a lower prevalence of metabolic syndrome and chronic kidney disease (49 vs. 54%; p = 0.023); they had the quotient albumin/creatinine, glucose, total cholesterol and LDL-cholesterol significantly minor (p < 0.001); and had an estimated glomerular filtration rate and HDL-cholesterol significantly higher (p < 0.001). Intake of ≥1 antihypertensive drugs in full dose at bedtime was associated with a mean resting BP significantly less than treatment with all medication upon rising (p < 0.001). The depth was significantly lower and the prevalence of the non-dipper pattern higher with all medication upon rising (68.6%) than with ≥1 drug upon waking. going to bed (55.8%; p < 0.001), and was reduced even more in patients taking all medication at bedtime (49.7%; p < 0.001), because this last group was characterized by having the lowest resting mean SBP (figure 3). The prevalence of riser pattern was much higher (23.6%) in patients taking all medication upon getting up than in those who took either any (20.0%), or all drugs at the same time. go to bed (12.2%; p < 0.001). This last group presented the highest rate of patients with Well-controlled ambulatory BP (p < 0.001), which was achieved with a smaller number of antihypertensive drugs (P < 0.001) compared with those treated at get up [26].
Influence of Chronotherapy on Cardiovascular risk in Patients with and without Diabetes
It has been discovered that asthma, allergic rhinitis, cancer, arthritis, heart attacks, etc. To cite some examples, they have a greater incidence at certain times of the day; heart attacks myocardial acute events are more frequent in the morning; otherwise, allergic rhinitis it is more frequent at night. Thus, the treatment must also follow a recommendation or application scheme adhered to a schedule based on the individual characteristics of the patient.
Most ABPM studies carried out to date have many limitations, including the use of arbitrary fixed bands of clock hours to define wake/rest (or erroneously day/night), which results in the calculation of values which do not represent the true BP activity/rest means for each individual; and most of the published results are derived from studies based on a single ABPM record for each patient at the time of inclusion, under the apparent erroneous assumption that the ambulatory BP profile remains unchanged during the years of follow-up despite the effects of treatment antihypertensive, aging and the development of damage to target organs or concomitant diseases [5,6,27].
In this sense, the Ambulatory Monitoring for Prediction of CV Events study (MAPEC) was designed to prospectively investigate the comparative prognostic value of various parameters derived from ABPM and study whether the intake of the dose. Complete with at least one antihypertensive drug at bedtime works best control of BP and reduction of CV risk than conventional therapy based on administer all medication in the morning upon rising [5,11,27,28,29]. In this study Prospectively, 3,344 subjects participated, of which 2,610 were hypertensive patients. According to ABPM criteria [30,31]. At the time of inclusion and then annually (or with more frequently if it was necessary to adjust antihypertensive treatment based on ABPM results) during a median of 5.6 years of follow-up, BP and physical activity (wrist actigraphy) were monitored simultaneously for 48h to in order to determine in a precise and individualized way the averages of activity and rest of the PA. The results of the MAPEC study, the first in which participants were periodically evaluated using ABPM, indicate, first of all, that the average rest, but not activity, SBP is the most significant predictor of CV events in a survival model adjusted for the significant variables of sex, age, diabetes, anemia and chronic kidney disease (for every 1-DT of elevation, hazard ratio [HR] 1.63; 95% CI [1.44-1.85]; p < 0.001 for the rest mean; 0.94 [0.81-1.08]; p = 0.348 for the average activity). The assessment of the possible joint contribution of several parameters derived from ABPM as predictors of CV risk revealed that the best fitted model includes only the mean of resting SBP (HR = 1.23; 95% CI [1.16-1.32]; p < 0.001) and the depth of SBP (HR = 0.98; 95% CI [0.97-0.99]; p = 0.019). Furthermore, when the average of SBP rest was adjusted for both mean SBP activity and BP clinical, only the first significantly predicted the increased risk of CV events, both in the general population [5,27] and specifically in patients with diabetes [8]. Which More importantly, analysis of changes in ambulatory BP over the years of Follow-up revealed a 17% decrease in CV risk for every 5 mmHg of reduction in mean resting SBP, independent of changes in BP clinical or in the average activity calculated from ABPM [5,6,27]. These results, Taken together, they indicate that resting mean BP could be a new target therapeutics for reducing CV risk that requires, obviously, the evaluation accuracy of patients using ABPM [31].
The MAPEC study thus constitutes the first prospective trial of the impact of Antihypertensive chronotherapy on CV risk. In this study, patients randomized to take medication at bedtime were characterized by having in their last evaluation with ABPM, after 5.6 years of follow-up, lower mean rest of BP, greater depth, lower prevalence of the non-dipper pattern and greater prevalence of controlled ambulatory BP than patients taking the entire medication when getting up [29]. Patients treated at bedtime had an HR of Total CV events significantly lower than patients treated upon rising (0.39; 95% CI [0.29-0.51]; p < 0.001). The difference between groups was also significant for the total of major events, that is, the sum of CV death, heart attack, myocardium and ischemic and hemorrhagic stroke (0.33; 95% CI [0.19-0.55]; p < 0.001). These The results were validated in high CV risk subgroups and further characterized due to a high prevalence of nocturnal hypertension, including patients with diabetes [32], resistant hypertension [28] and chronic kidney disease [33].
Conclusions
The prevalence of subclinical BP alterations, detected by ABPM, is elevated in patients with diabetes and are associated with the presence of other risk factors. Vascular risk such as metabolic control, BMI and more atherogenic lipid profile. The non-dipper pattern and nocturnal BP averages are determinants in the risk of micro and macrovascular complications of diabetes and although there are no recommendations of the main scientific societies for the use of ABPM specific in patients with diabetes, if there is strong evidence that, in patients hypertensive diabetics, the use of antihypertensive drugs before going to bed probably favors BP control and reduces macrovascular events.
The ABPM studies published to date reviewed here agree on document the high prevalence of an altered circadian BP pattern in patients with diabetes. Most importantly, the prevalence of the riser pattern, associated with the highest CV risk among all possible BP patterns, it is more than double in patients with diabetes than without it. Patients with diabetes also have a significant elevation of ambulatory PP over 24 hours, reflecting greater arterial stiffness and may thus be an added cause of the documented higher CV risk in them [34]. One of the determining characteristics of the BP profile in diabetes is the high average BP during nighttime rest hours, in turn causing a high prevalence of nocturnal hypertension and, as a consequence, errors in diagnosis of hypertension when it is based exclusively on the clinical measurement of BP or even in home self- -measurements (AMPA). These results, taken together, largely explain the higher CV risk of patients with diabetes and justify the need to use ABPM as an essential diagnostic tool for hypertension in patients with diabetes, both for the correct assessment of their CV risk to establish the most appropriate therapeutic scheme for the control of high nocturnal BP and ambulatory PP, which could in turn result in a significant reduction in CV events, as has already been demonstrated [32].
The goal of antihypertensive treatment is to reduce BP with the aim of preventing damage to target organs and reduce the risk of CV events. The beneficial effects associated with BP reduction are consistent and, to some extent, independent of the medication used.
The therapeutic strategy of a single morning dose, still common, does not take into account that the correlation between BP level and CV risk is much greater for ABPM than for clinical measures of PA [5,35]; than the mean resting BP, but not the mean activity or 24 h nor clinical BP, is an independent prognostic marker CV [5,6,8,27,28] risk and that the effectiveness in reducing the level (mainly of the resting average) and improve the circadian pattern of BP towards a more dipper profile of a good number of antihypertensive drugs from 6 different families and their combinations depends markedly on the time of intake in relation to the cycle of activity and rest of the patient [20-22]. In the specific field of diabetes, the results of the study by Moyá et al. [26] document a significantly lower CV risk markers and a better metabolic profile in patients with diabetes treated at bedtime compared to those taking all medication when getting up; The results also document a lower average rest period of the BP and reduced prevalence of the no-dipper/riser pattern of high CV risk in patients with diabetes treated at bedtime. These results indicate that bedtime treatment, together with ABPM assessment to establish the correct diagnosis of hypertension and avoid possible nocturnal hypotension associated with treatment, should be the preferred therapeutic regimen in patients with diabetes [26]. On the other hand, the results of the MAPEC study [5,11,27,28,29,32,33], indicate that reducing the average of the period of BP rest and increase the depth towards a more dipper profile (two new therapeutic objectives that require evaluation of patients with ABPM) significantly reduce CV morbidity and mortality and intake of the full dose of at least one antihypertensive, preferably all, at bedtime reduces significantly the risk of CV events in both the general hypertensive population [29] as specifically in patients with diabetes [32]. In this sense, it is notable that already in 2012, the American Diabetes Association recognized the clinical relevance of antihypertensive chronotherapy by recommending that hypertensive patients with diabetes. They should be treated with ≥1 drug at bedtime [36]. This recommendation implies in fact that bedtime treatment should be the therapeutic regimen of choice in all patient with diabetes newly diagnosed with hypertension. The blocking of RAAS receptors achieved through the ingestion of the ACEI or ARA II at the time of lying down is superior to any other treatment regimen in reducing the risks of CVD, diabetes and CKD [37]. Diabetes is associated with greater BP variability than non-diabetics along with worse damage to vascular and renal function [38]. This same recommendation, complemented with the indication to use ABPM as a new gold standard for diagnosis of hypertension and individualized assessment of CV risk, has recently been extended to other groups, including elderly subjects and patients with chronic kidney disease, previous CV event and resistant hypertension or secondary [31].
Practical Ideas
● Patients with diabetes present a significant elevation of ambulatory PP throughout 24 hours, which reflects greater arterial stiffness and may thus be a cause added to the documented increased CV risk, in them the prevalence of the riser pattern, associated with the highest CV risk among all possible BP patterns, it is more twice as much as in patients without diabetes.
● One of the determining characteristics of the BP profile in diabetes is the high average BP during the hours of night rest, in turn causing a high prevalence of nocturnal hypertension and, as a consequence, errors in diagnosis of hypertension when it is based exclusively on clinical measurement of the BP or even by AMPA.
● Antihypertensive treatment at bedtime should be the therapeutic regimen of choice in all patients with diabetes newly diagnosed with hypertension. He blockade of RAAS receptors achieved by ingestion of the ACEI or ARA II at bedtime is superior to any other treatment regimen for reduce the risks of CVD, diabetes and CKD.
● In diabetics, ABPM should be included in routine clinical care, as method to confirm the diagnosis of hypertension, to determine the nyctameral pattern of BP these patients and assess the response to treatment by facilitating chronotherapy, non-optimal control or to see the degree of control in 24 hours.
- Dawber TR, Moore FE, Mann GV (1957) Coronary heart disease in the framingham study. Am J Public Health, 47: 4-23.
- Dawber TR, Kannel WB, Revotskie N, Stokes JL, Kagan A, Gordon T (1959) Some factors associated with the development of coronary heart disease. Six years´ follow-up experience in the Framigham Study. Am J Public Health, 49: 1349-56.
- Mostaza JM, Peña R, Lahoz C (2001) Clin Invest Arteriosclerosis, 13: 5-14.
- Villalba Alcalá F (2003) Cardiovascular Risk Factors: Concept and Classification. In Cardiovascular Risk Factors. Chapter 2: 23-32.
- Hermida RC, Ayala DE, Mojón A, Fernández Jr (2011) Decreasing sleep-time blood pessuredetermined by ambulatory monitoring reduces cardiovascular risk. J Am Coll Cardil, 58: 1165-73.
- Hermida RC, Ayala DE, Mojón A, Smolensky MH, Portaluppi F, Fernández JR (2014) Sleep-time ambulatory blood pressure as a novel therapeutic target for cardiovascular risk reduction. J Hum Hypertens, 28: 567-74.
- Roush GC, Fagard RH, Salles GF, Pierdomenico SD, Reboldi G, Verdecchia P, et al. (2014) Prognostic impact from clinic, daytime, and nighttime systolic blood pressure in 9 cohorts on 13,844 patients with hypertension. J Hypertens, 32: 2332-40.
- Hermida RC, Ayala DE, Mojón A, Fernández JR (2012) Sleep-time blood pressure as a therapeutic target for cardiovascular risk reduction in type 2 diabetes. Am J Hypertens, 25: 325-34.
- Astrup AS, Nielsen FS, Rossing P, Ali S, Kastrup J, Smidt UM, et al. (2007) Predictors of mortality in patients with type 2 diabetes with or without diabetic nephropathy: A follow-up study. J Hypertens, 25: 2479-85.
- Bouhanick B, Bongard V, Amar J, Bousquel S, Chamontin B (2008) Prognostic value of nocturnal blood pressure and reverse-dipping status on the occurrence of cardiovascular events in hyperten sive diabetic patients. Diabetes Metab, 34: 560-7.
- Hermida RC, Ayala DE, Mojón A, Fernández JR (2013) Cardiovascular risk of essential hypertension: Influence of class, number, and treatment-time regimen of hypertension medications. Chronobiol Int. 30: 315-27.
- Hermida RC, Moyá A, Ayala DE (2015) Ambulatory blood pressure monitoring in diabetes for the assessment and control of vascular risk. Endocrinol Nutr, 62: 400-10.
- Cuspidi C, Meani S, Lonati L, Fusi V, Valerio C, Sala C, et al. (2006) Short-term reproducibility of a non-dipping pattern in type 2 diabetic hypertensive patients. J Hypertens, 24: 647-53.
- Afsar B, Sezer S, Elsurer R, Ozdemir FN (2007) Is H.O.M.A index a predictor of nocturnal nondipping in hypertensives with newly diagnosed type 2 diabetes mellitus? Blood Press Monit, 12: 133-9.
- Pistrosch F, Reissmann E, Wildbrett J, Koehler C, Hanefeld M (2007) Relationship between diurnal blood pressure variation and diur nal blood glucose levels in type 2 diabetic patients. Am J Hypertens, 20: 541-5.
- Palmas W, Pickering T, Teresi J, Schwartz JE, Eguchi K, Field L, et al. (2008) Nocturnal blood pressure elevation predicts progression of albuminuria in elderly people with type 2 diabetes. J Clin Hypertens (Greenwich). 10: 12-20.
- Ayala DE, Moyá A, Crespo JJ, Castineira ˜ C, Domínguez-Sardina˜ M, Gomara S, et al. (2013) Circadian pattern of ambulatory blood pres sure in hypertensive patients with and without type 2 diabetes. Chronobiol Int, 30: 99-115.
- Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Pede S, Porce llati C (1998) Ambulatory pulse pressure: A potent predictor of total cardiovascular risk in hypertension. Hypertension, 32: 983-8.
- Gorostidi M, de la Sierra A, González-Albarrán O, Segura J, de la Cruz JJ, Vinyoles E, et al. (2011) Abnormalities in ambulatory blood pressure monitoring in hypertensive patients with diabetes. Hypertens Res, 34: 1185-9.
- Smolensky MH, Hermida RC, Ayala DE, Tiseo R, Portaluppi F (2010) Administration-timedependent effect of blood pressure-lowering medications: Basis for the chronotherapy of hypertension. Blood Press Monit, 15: 173-80.
- Hermida RC, Ayala DE, Fernández JR, Mojón A, Smolensky MH, Fabbian F, et al. (2013) Administration-- time-differences in effects of hypertension medications on ambulatory blood pressure regulation. Chronobiol Int, 30: 280-314.
- Hermida RC, Ayala DE, Smolensky MH, Fernández JR, Mojón A, Crespo JJ, et al. (2014) Chronotherapeutics of conventional blood pressure-lowering medications: Simple, low-cost means of improving management and treatment outcomes of hypertensive-related disorders. Curr Hypertens Rep. 2014: 16.
- Villalba Alcalá F, et al. (2004)"Study using ambulatory blood pressure monitoring of the white coat effect in hypertensive patients treated and controlled in Primary Care." Rev Esp Cardiol, 57: 652-60.
- Villalba Alcalá F, et al. (2003) "Influence on the White Coat Effect and heart rate of antihypertensive drugs used in an urban health center." Rev Invest Clín (Tlalpan) (Mexico) 55: 429-37.
- Fabbian F, Smolensky MH, Tiseo R, Pala M, Manfredini R, Portaluppi F (2013) Dipper and nondipper blood pressure 24-hour patterns: Circadian rhythm-dependent physiologic and pathophysiologic mechanisms. Chronobiol Int. 30: 17-30.
- Moyá A, Crespo JJ, Ayala DE, Ríos MT, Pousa L, Callejas PA, et al. (2013) Effects of time-of-day of hypertension treatment on ambulatory blood pressure and clinical characteristics of patients with type 2 diabetes. Chronobiol Int. 30: 116-31.
- Hermida RC, Ayala DE, Fernández JR, Mojón A (2013) Sleep-time blood pressure: Prognostic value and relevance as a therapeutic target for cardiovascular risk reduction. Chronobiol Int. 30: 68-86.
- Ayala DE, Hermida RC, Mojón A, Fernández JR (2013) Cardiovascular risk of resistant hypertension: Dependence on treatment-time regimen of blood pressure-lowering medications. Chronobiol Int, 30: 340-52.
- Hermida RC, Ayala DE, Mojón A, Fernández JR (2010) Influence of circadian time of hypertension treatment on cardiovascular risk: Results of the MAPEC study. Chronobiol Int, 27: 1629-51.
- Mancia G, Fagard R, Narkiewicz K, Redón J, Zanchetti A, Böhm M, et al. (2013) ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens, 31: 1281-357.
- Hermida RC, Smolensky MH, Ayala DE, Portaluppi F, Crespo JJ, Fabbian F, et al. (2013) Ambulatory blood pressure monitoring recommendations for the diagnosis of adult hypertension, assessment of cardiovascular and other hypertension-associated risk, and attainment of therapeutic goals. Joint recommendations from the International Society for Chronobiology (ISC), American Association of Medical Chronobiology and Chronotherapeutics (AAMCC), Spanish Society of Applied Chronobiology, Chronotherapy, and Vascular Risk (SECAC), Spanish Society of 410 R.C. Hermida et al. Atherosclerosis (SEA), and Romanian Society of Internal Medicine (RSIM). Chronobiol Int, 30: 355-410.
- Hermida RC, Ayala DE, Mojón A, Fernández JR (2011) Influence of time of day of blood pressurelowering treatment on cardiovascular risk in hypertensive patients with type 2 diabetes. Diabetes Care 34: 1270-6.
- Hermida RC, Ayala DE, Mojón A, Fernández JR (2011) Bedtime dosing of antihypertensive medications reduces cardiovascular risk in CKD. J Am Soc Nephrol, 22: 2313-21.
- Raija Lithovius , Gordin D, Forsblom C, Saraheimo M, Harjutsalo V, Groop PH (2018) on behalf of the FinnDiane Study Group. Ambulatory blood pressure and arterial stiffness in individuals with type 1 diabetes. Diabetologia 61: 1935-45
- Eguchi K, Pickering TG, Hoshide S, Ishikawa J, Ishikawa S, Schwartz J, et al. (2008) Ambulatory blood pressure is a better marker than clinic blood pressure in predicting cardiovascular events in patients with/without type 2 diabetes. Am J Hypertens, 21: 443-50.
- American Diabetes Association (2012) Standards of Medical Care in Diabetes-2012. Diabetes Care, 35: S11-63.
- Hermida RC, Ayala DE, Fernandez JR, Mojon A, Smolensky MH (2018) Hypertension: New perspective on its definition and clinical management by bedtime therapy substantially reduces cardiovascular disease risk. Eur J Clin Invest. 2018; 48: e12909.
- Rouxinol-Dias AL, Gonçalves ML, Ramalho D, Silva J, Barbosa L, Polónia J (2022) Comparison of Blood Pressure Variability between 24 h Ambulatory Monitoring and Office Blood Pressure in Diabetics and Nondiabetic Patients: A Cross-Sectional Study. Int J Hypertens, 2022: 1022044.
FIGURE 1
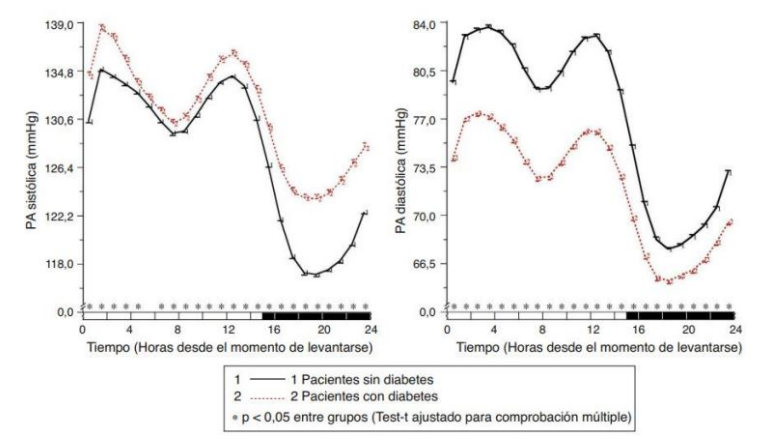
Figure 1: Circadian Pattern of SBP (left) and DBP (right) in hypertensive patients without (solid line) and with diabetes (dashed line) assessed through 48-hour ambulatory blood pressure monitoring. The shaded bar on the horizontal axis of the graphs indicates the average nighttime hours of patient sleep
FIGURE 2
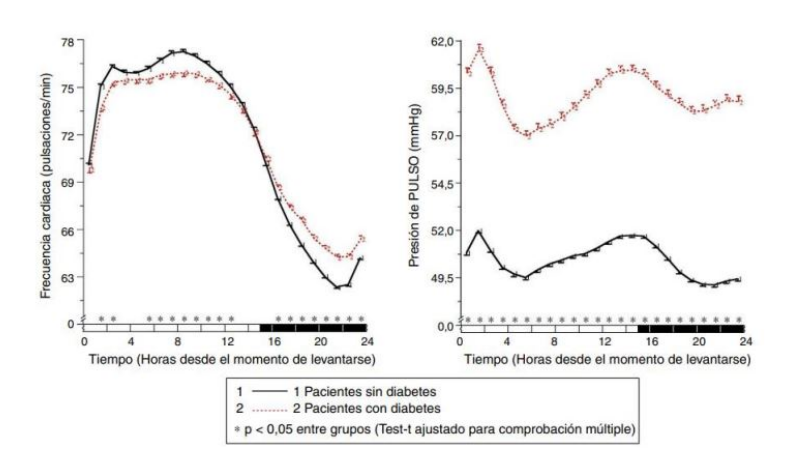
Figure 2: Circadian pattern of heart rate (left) and pulse pressure (PP) (right) in hypertensive patients without (solid line) and with diabetes (dashed line) assessed through 48-hour ambulatory blood pressure monitoring (ABPM). The shaded bar on the horizontal axis of the graphs indicates the average nighttime rest period of the patients.
FIGURE 3
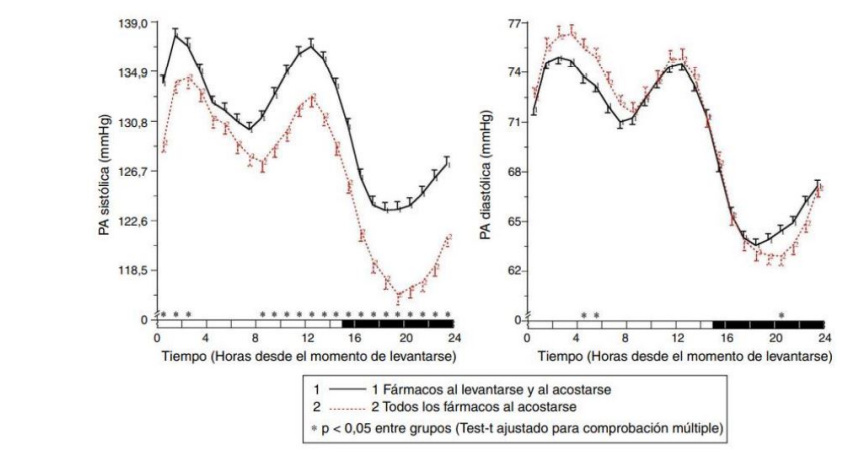
Figure 3: Circadian Pattern of Systolic Blood Pressure (left) and Diastolic Blood Pressure (right) in hypertensive patients with diabetes evaluated through 48-hour ambulatory blood pressure monitoring (ABPM) and classified based on their antihypertensive treatment scheme: medication intake both upon waking up and before going to bed (solid line) or intake of all medication at bedtime (dashed line). The shaded bar on the horizontal axis of the graphs indicates the average nighttime rest period of the patients
Tables at a glance
Figures at a glance