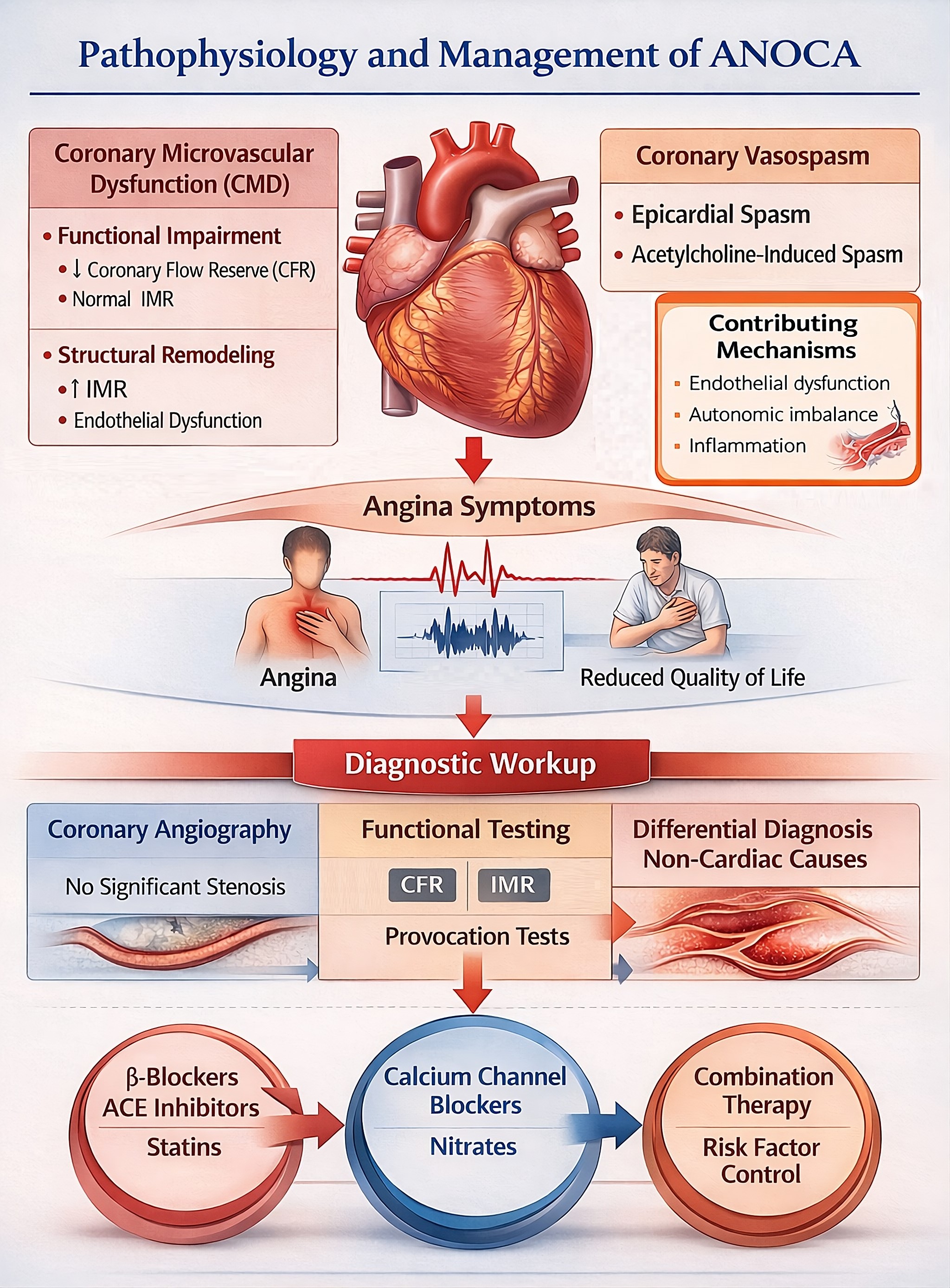
Figure 1: Angina with non-obstructive coronary arteries (ANOCA) is a heterogeneous clinical syndrome predominantly driven by coronary microvascular dysfunction (CMD) and coronary vasomotor disorders. CMD may result from functional impairment, characterized by reduced coronary flow reserve (CFR) with normal microvascular resistance, or from structural remodeling associated with increased index of microvascular resistance (IMR) and endothelial dysfunction. Coronary vasomotor disorders include epicardial and microvascular vasospasm, which may be provoked by acetylcholine testing. Endothelial dysfunction, autonomic imbalance, and inflammatory processes contribute to the development and progression of these abnormalities. These mechanisms lead to angina symptoms and impaired quality of life despite the absence of obstructive epicardial coronary artery disease. Diagnostic evaluation begins with coronary angiography demonstrating no significant stenosis and is complemented by invasive functional testing, including assessment of CFR, IMR, and vasoreactivity, as well as exclusion of non-cardiac causes of chest pain. Management should be mechanism-based, with beta-blockers, angiotensin-converting enzyme inhibitors, and statins commonly used in CMD, calcium channel blockers and nitrates as first-line therapy in vasospastic angina, and comprehensive cardiovascular risk factor control as part of an individualized treatment strategy.
Tables at a glance
Figures at a glance