Case Report Open Access Spontaneous Hemopneumothorax: Late Manifestation of a Cavitary Lesion by Aspergillus Infection
Received Date: October 21, 2023 Accepted Date: November 21, 2023 Published Date: November 23, 2023
doi: 10.17303/jlpm.2023.2.102
Citation: Daniel E Font Rivera, Kyomara Hernandez-Moya, Juan M Garcia Puebla, Claudia Quiles Cruz, Jonathan Torrens Olan et al. (2023) Spontaneous Hemopneumothorax: Late Manifestation of a Cavitary Lesion by Aspergillus Infection. J Lung Dis Pulm Med 2: 1-7
Abstract
Background: Spontaneous hemopneumothorax (SH) is a rare life-threatening condition that involves accumulation of blood and air in the pleural space in absence of any trauma or other underlying diseases. It is a complication of 1-12% of patients with spontaneous pneumothorax. Late recognition and delayed intervention can lead to higher mortality rate.
Case presentation: A 33-year-old man who was brought to the emergency room with a history of dry cough, chest pain, shortness of breath, weakness, dizziness, and hemoptysis of five days evolution. Physical examination detected marked reduction of breath sounds on the left hemithorax. A chest X-ray showed apical pneumothorax and pleural effusion. Computed Tomography scan detected the presence of a thick-walled cavitary lesion, bronchopleural fistula, and a complex hemorrhagic left-sided hemopneumothorax associated with lungs collapse. An emergency left-sided thoracostomy was performed. Besides, antifungal and antibiotics were administered and surgical excision of the lower lobe. There was a complete resolution of the patient’s symptoms and post-op images showed expansion of the lungs and prevention of further hemoptysis.
Conclusion: Spontaneous hemopneumothorax is a potentially life-threatening disorder. Effective management of this condition requires early recognition and appropriate early intervention. Once the diagnosis is confirmed, early thoracotomy should be considered.
Keywords: Spontaneous Hemopneumothorax; Spontaneous Pneumothorax; Spontaneous Hemothorax; Thoracostomy
Background
Hemothorax is a clinical entity, defined as the extraction of pleural fluid with hematocrit more than 50% of the patient’s blood [1,2]. Hemothorax is mostly associated with open or closed-chest trauma, an infection/inflammation, coagulopathies, malignancies, congenital arteriovenous malformations, and some iatrogenic causes arising from certain procedures including thoracentesis, central line insertion, pleural biopsy, and catheterization [1-3]. There is one subcategory of hemothorax, referred to as spontaneous hemothorax, in which blood accumulates in the pleural space without any obvious cause or trauma [2,4]. Spontaneous hemothorax is usually associated with anticoagulation, neoplasia, or pleural adhesion rupture. Although the clinical appearances of SH vary greatly, the primary manifestation includes progressive chest pain and dyspnea. In extreme cases it can lead to hemodynamic instability [2].
Another rare clinical entity with quite similar manifestations as that of SH is spontaneous hemopneumothorax (SHP), which mostly occurs in young adults [5]. SHP is a combination of two medical conditions: pneumothorax and hemothorax. In pneumothorax, air with a limited amount of fluid accumulates in the pleural cavity and causes lung collapse. SHP is defined as the accumulation of more than 400 ml blood in the pleural cavity along with spontaneous pneumothorax in absence of trauma or other related causes [1,6]. Spontaneous pneumothorax (SP) is a well-known disorder with typical symptoms including acute onset of chest pain and dyspnea and it gets complicated with the occurrence of SHP [6]. Around 0.5 -12% of patients suffering from SP may develop SHP [6]. The key clinical features of SHP are chest pain, dyspnea, anemia, and often hemodynamic instability and shock that can be fatal and depends on the extent of hemorrhage [7]. It may be lifethreatening in about one-third of the patients [5]. If there is considerable blood loss, then thoracostomy is required for intrapleural chest drain to obtain homeostasis [6]. The first case of SHP was reported in 1876 and several lethal cases were reported in the earlier part of 20th century [6,8]. Nonetheless, SHP is a rare disorder globally in which to our knowledge only few case studies has been reported.
In this report, we describe an uncommon case of a patient with SHP who presented to our emergency room with chest pain, shortness of breath, and dry cough along with some other clinical manifestations slightly different from those described in previous literature.
Case Presentation
A 33-year-old immunocompetent man brought to the emergency room with symptoms of dry cough, chest pain, and dyspnea for several days and hemoptysis of five days of evolution. His clinical history revealed that he had suffered from pulmonary aspergillosis a month ago without any history of trauma and received treatment with antifungal drug voriconazole for 2 weeks; however, he had poor outpatient follow up of antifungal treatment. His vital signs on admission were as follows: blood pressure 90/50 mmHg, heart rate 114 beats/min, respiratory rate: 18 breaths/min, body temperature 36.3 °C, bodyweight: 190 lbs., height: 5’10’’, and body-mass index 27.2 kg/m2. His physical examination was remarkable for decreased breath sounds on the left hemithorax, otherwise normal examination. Chest radiograph showed a left-sided apical pneumothorax associated with pleural effusion, right mediastinal shifting, and cavitary lesion (Figure 1). Computed tomography (CT) scan of the chest confirmed the presence of a thick-walled cavitary lesion with bronchopleural fistula (Figure 2). Additionally, a complex hemorrhagic left-sided hemopneumothorax linked with the collapse of left lung was detected (Figure 3).
Laboratory evaluation of complete blood count (CBC) showed significant leukocytosis (25,700) with stable hemoglobin level (12.1mg/dL) and platelet count (Table 1). Complete metabolic panel (CMP) data was consistent with hyperglycemia with blood glucose level of 236 and acute kidney injury with a creatinine level of 1.49, lactic acid of 43.7 mg/dL, and coagulation profile within normal range (Table 1). The basal metabolic panel (BMP) showed sodium 139, potassium 4.2, chloride 106, and bicarbonate 23 (Table 1). Arterial blood gas (ABG’s) measures indicated partial pressures of carbon dioxide (pCO2) and oxygen (pO2) to be 32.8 mmHg and 75.1 mmHg respectively and oxygen saturation of 95.2% (Table 1). The patient was subjected to emergency left-sided thoracostomy and about 1,400mL of bright red blood was drained from the thoracostomy tube. Subsequently, he became hemodynamically unstable, with a decrease in hemoglobin from 12.1 mg/dL to 9 mg/dL. Intravenous antifungal and antibiotic therapy (Voriconazole and Vancomycin + Meropenem) were started immediately based on patient critically ill state and established by Infectious disease specialist to provide adequate broad spectrum antimicrobial coverage for fungal, MRSA and anaerobic species. Due to continued drainage and hemodynamic instability a left lower lobectomy of the lung was performed by cardiothoracic surgeon. The patient responded to the treatment well and ultimately his clinical symptoms were subsided within 1 week.
Discussion
Spontaneous hemopneumothorax is a rare clinical condition resulting from the rupture of tiny blood vessels adhered between parietal and visceral pleura [9]. Bleeding in SHP occurs due to any of the three probable mechanisms- firstly, the rupture of the small non-contractile vessels on the parietal pleura having vascular adhesions with the visceral pleura [1,5,6] secondly, the tearing of vascularized bullae and underlying lung parenchyma and finally, shearing of congenital aberrant blood vessels between the parietal pleura and bullae [1,4-6]. The resulting hemorrhage and shock may require emergency surgery [7]. SHP is a complication of primary or secondary pneumothorax [5]. The chest Xray of our patient revealed a left-sided apical pneumothorax associated with pleural effusion indicating the link between spontaneous pneumothorax with SHP in the absence of any trauma, underlying lung diseases, and surgery. Pleural effusion is directly correlated to pleural invasion and has a high hematocrit value and bloody appearance [10].
The patient had previously suffered from pulmonary aspergillosis, which was treated with the antifungal drug voriconazole; however, he had an inappropriate follow-up for treatment with antifungals. His radiographic images revealed a late manifestation of pulmonary aspergillosis complications. Aspergillosis is caused by a ubiquitous fungus Aspergillus spp. The fungus can be inhaled in the form of air-borne spores, and they colonize in the airways. Typically, pulmonary aspergillosis is found in individuals suffering from underlying airway diseases, such as asthma or cystic fibrosis or other lung diseases, or in immune compromised individual [11,12]. Zhang and colleagues (2010) reported a patient with a 20-year history of asthmatic disease suffering from recurrent pneumothorax and pleural aspergillosis [12]. In contrast, our patient had no history of underlying pulmonary disease, yet he developed aspergillosis, which could be due to his impaired immune system. Moreover, when aspergillosis is not treated properly, the colonies of Aspergillus spp. remain in the pleural cavity, which primarily leads to the formation of bronchopleural fistula, followed by pleural cavity infection resulting in the cavitary lesion [13]. Likewise, the cavitary lesions and bronchopleural fistula in our patient represented unsuccessfully treated aspergillosis. One of the devastating complications of pulmonary aspergillosis is massive hemoptysis [11] as seen in our patient. No causal relationship between spontaneous pneumothorax and aspergillosis has been elucidated till date. Hence, it is less likely that spontaneous hemopneumothorax in our patient is correlated to previous Aspergillus spp. infection.
While there isn't a direct and widely recognized link between pulmonary aspergillosis and spontaneous hemopneumothorax, it's important to note that aspergillosis can contribute to various pulmonary complications, particularly in individuals with weakened immune systems or underlying lung conditions. Aspergilloma, a fungal ball composed of Aspergillus species, can form in pre-existing lung cavities, such as those resulting from tuberculosis or other lung diseases. In some cases, aspergillomas may erode into blood vessels, potentially leading to bleeding into the airspaces (hemoptysis), but this is distinct from spontaneous hemopneumothorax
Spontaneous non-traumatic hemopneumothorax has a much higher incidence in males than in females (about 30 times more) [6] with a median age presentation of 22 to 34 years [1], in conformity our patient was a 33- year-old male. The patients with pneumothorax have a higher probability of developing SHP. The escape of air from the lungs into the pleural space in pneumothorax prevents the lungs from expansion and ultimately the lungs collapse leading to severe breathing problem, dry cough, and dyspnea. Accordingly, our patient had left-sided SHP associated with abrupt lung collapse.
A large spontaneous hemopneumothorax is often deadly if a patient suddenly develops hypovolemic shock symptoms due to excessive blood loss [6,9]. Therefore, late diagnosis and treatment may increase the mortality rate of SHP patients [9]. The physicians should be aware of the symptoms of SHP and differentiate it from SP or SH. The main symptoms that are anticipated to alert the physician about SHP include detection of an air-fluid line at radiologic images, development of a hemorrhagic effusion, and hypovolemic shock symptoms [5]. No treatment consensus for SHP exists at present [12]. However, immediate management of SHP typically includes fluid resuscitation and drainage of pleural space, hemostasis, and finally re-expansion of the lungs [4,5]. In some cases, homologous blood transfusion is required [4]. Conservative or surgical management most often depends on the patient’s hemodynamic status since it may lead to lethal complications. We performed left- -sided tube thoracostomy immediately in our patient to secure effective drainage of fluid from the pleural space. The patient underwent a left lower lobectomy and systemic treatment with intravenous antifungal and antibiotics for pulmonary aspergillosis with the resolution of the clinical symptoms successfully. The surgical resection of the infected portion of the lung probably improved the prognosis of the patient.
Conclusion
In conclusion, spontaneous hemopneumothorax is a rare clinical entity that can result in potentially lifethreatening conditions. Furthermore, it is quite uncommon to detect a case of SHP and pulmonary aspergillosis simultaneously. SHP is an atypical but treatable clinically. The healthcare professionals should be aware of the signs, symptoms, and available acute and lifesaving management for this type of manifestation. The diagnosis of SHP is based on identifying the clinical patterns of sudden chest pain, shortness of breath, dyspnea, amount of blood loss and air leakage, and shock. The treatment regime must be decided according to the patient’s health condition, clinical manifestations, and etiology of the disease. Timely diagnosis and management using early thoracostomy and occasionally surgical intervention is crucial to obtain improved long-term outcomes in patients with SHP.
Declaration of Interest
None
Funding
This case report did not receive any specific grant form any funding agency in the public, commercial or notprofit sectors.
- Ali HA, Lippmann M, Mundathaje U, Khaleeq G (2008) Spontaneous Hemothorax- A Comprehensive Review. Chest 134: 1056-65.
- Patrini D, Panagiotopoulos N, Pararajasingham J, Gvinianidze L, Iqbal Y, Lawrence DR (2015) Etiology and management of spontaneous haemothorax. J Thorac Dis 7: 520-6.
- Li PS, Tsai CL, Hu SY, Lin TC, Chang YT (2017) Spontaneous hemothorax caused by ruptured multiple mycotic aortic aneurysms: a case report and literature review. J Cardiothorac Surg 12.
- Ho C, Ismail AR (2014) Spontaneous Haemothorax: A Case Report. Med J Malaysia 5: 234-5.
- Kakaris S, Athanassiadi K, Vassilikos K, Skottis I (2004) Spontaneous hemopneumothorax: a rare but lifethreatening entity. Eur J Cardiothorac Surg 25: 856-8.
- Chen Y, Guo Z (2018) Unusual case of primary spontaneous hemopneumothorax in a young man with atypical tension pneumothorax: a case report. J Med Case Rep 12.
- Hsu CC, Wu Yl, Lin HJ, Lin MP, Guo HR (2005) Indicators of haemothorax in patients with spontaneous pneumothorax. Emerg Med J 22: 415-17.
- Hsu NY, Shih CS, Hsu CP, Chen PR (2005) Spontaneous hemopneumothorax revisited: clinical approach and systemic review of the literature Ann Thorac Surg 80: 1859-63
- Kim ES, Kang JY, Pyo CH, Jeon EY, Lee WB (2008) 12-year experience of spontaneous hemopneumothorax. Ann Thorac Cardiovasc Surg 12: 149-53.
- Krenke R, Joanna K, Korczynski P, Kupis W, Szolkowska M, Chazan R (2011) Hemoptysis and spontaneous hemothorax in a patient with multifocal nodular lung lesions. Chest 140: 245-51.
- Betancourt BY, Garofoli AC, Sandhu JS, Borna N, M Sy A (2015) Pulmonary aspergillosis presenting with recurrent haemoptysis. BMJ Case Rep.
- Zhang W, Hu Y, Chen L, Gao J, Xie L (2010) CPalsee rueproart l aspergillosis complicated by recurrent pneumothorax: a case report. J Med Case Rep 4.
- Rummens P, Bruyneei M, Lungarella M, Ninane V (2014) Aspergillus tracheobronchitis,bronchopleural fistula and empyema after lobectomy for aspergilloma. Med Mycol Case Rep 6: 25-8.
FIGURE 1
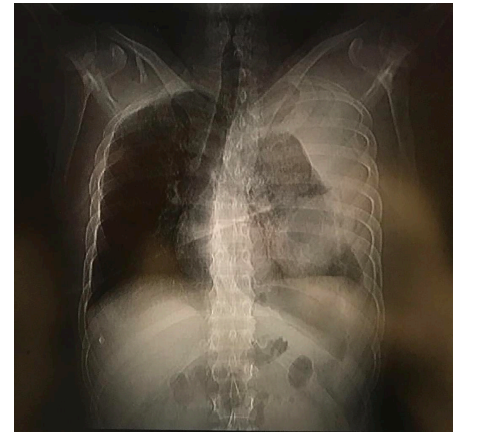
Figure 1: Initial Chest X-ray with left sided pnuemothorax with right tracheal deviations
FIGURE 2

Figure 2: Chest CT scan showing thick wall cavitary lesion with a left sided hemopneumothorax and fistula
FIGURE 3
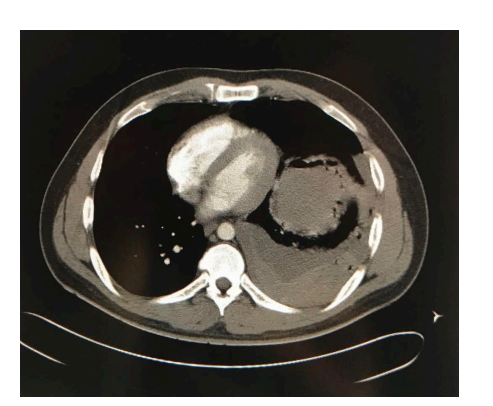
Figure 3: Chest CT scan showing thick wall cavitary lesion with a left sided hemopneumothorax and fistula
Tables at a glance
Figures at a glance