COVID-19 and Diabetes Mellitus Treatment
Received Date: December 17, 2023 Accepted Date: January 17, 2024 Published Date: January 20, 2024
doi: 10.17303/jmdd.2024.2.101
Citation: Ibrahim Tugrul (2024) COVID-19 and Diabetes Mellitus Treatment. J Metab Disord Diabetes 2: 1-10
Abstract
Coronavirus Disease 2019 (COVID-19), caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), has been the global health problem for more than one year. Diabetes mellitus has been a common comorbid condition in COVID-19 patients. The prognosis of COVID-19 disease is adversely affected by diabetes mellitus. Diabetes mellitus could be a risk factor for severity and mortality in patients with COVID-19. This review aims to explore the effectiveness and safety of the antidiabetic drugs in COVID-19 patients. Numerous studies have shown that pro-inflammatory cytokine levels are extremely high in COVID-19 patients. Dipeptidyl peptidase-4 (DPP-4), also known as CD26, is involved in cytokine production and inflammation. DPP4 inhibitors, commonly called gliptins, are widely used as effective oral hypoglycemic drugs in the treatment of type-2 diabetes mellitus. The research studies of DPP-4 inhibitors have exciting potential for diabetic patients infected with COVID-19. Sodium-glucose cotransporter-2 (SGLT2) inhibitors, reduce blood glucose levels. SGLT2 inhibitors have anti-inflammatory effect. However, SGLT2 inhibitors can cause ketoacidosis, especially in critically ill COVID-19 patients. A significant number of COVID-19 patients develop cardiac complications. Glucagon-like peptide 1 (GLP-1) agonists and thiazolidinediones such as pioglitazone have shown to upregulate ACE2. Metformin use is associated with a significant reduction in the rate of heart failure and with increased incidence of acidosis in critically ill patients. Hence, insulin remains the drug of choice in these situations. The results may be useful for the clinical treatment of COVID-19 patients with comorbid Diabetes Mellitus.
Keywords: COVID-19; Diabetes Mellitus; DPP4 Inhibitor; SGLT2 Inhibitor; Metformin; Thiazolidinediones
Core Tip: Diabetes mellitus is a common comorbid condition in patients with COVID-19. The prognosis of COVID-19 disease is adversely affected by diabetes mellitus. Diabetes Mellitus could be a risk factor for severity and mortality in patients with COVID-19. This review aims to explore the effectiveness and safety of the antidiabetic drugs in COVID-19 patients.
Introduction
Coronavirus Disease 2019 (COVID-19), caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-- CoV-2), has been the global health problem for more than one year. COVID-19 is highly contagious and is leading to high mortality rates [1]. The most common symptoms and clinical spectrum of COVID-19 ranges from asymptomatic presentation or upper respiratory symptoms (flu like symptoms, fever, headache, fatigue, sore throat, coughing, dyspnea) to gastrointestinal symptoms, severe pneumonia, acute respiratory distress syndrome (ARDS), septic shock and death [1-3]. Hypertension and Diabetes Mellitus are the most common comorbid conditions in patients with COVID-19. The prognosis of COVID-19 disease is adversely affected by diabetes mellitus [4]. In a systematic review including eight different studies, encompassing a total of 46,248 confirmed cases, Yang et al. found that the most common co-morbidities among COVID-19 patients were hypertension (17%), diabetes (8%). and respiratory diseases (2%) [5]. Diabetes could be a risk factor for severity and mortality in patients with COVID-19. The Chinese Center for Disease Control and Prevention, after analysing 72.314 COVID-19 cases, reported that diabetic patients had a threefold higher mortality rate than non-diabetic patients (7.3% vs 2.3%) [6]. The literature has shown that diabetes mellitus is a major comorbidity that significantly increases the risk of death and adverse complications in individuals with COVID-19 [7,8]. Patients with diabetes are expected to have an increased severity and risk of being admitted to the intensive care unit (ICU) with respiratory failure and multiorgan dysfunction following SARS-CoV-2 infection [2,6]. It has been shown that hyperglycemia is one of the risk factors in these patients [9]. One of the largest retrospective cohort studies conducted on in-patient subjects, indicates that well-controlled blood glucose levels are associated with a remarkable reduction in death and adverse complications in COVID-19 patients with comorbid Diabetes Mellitus [8,10]. Such studies show the importance of intensive blood glucose management in COVID-19 patients with comorbid diabetes mellitus [10]. Glycemic control is beneficial in restoring the dysregulation of the immune system and preventing infections [11]. Most antihyperglycemic medications showed anti-inflammatory effects in animal models of lung injury [12]. It is worthwhile considering that such patients are on multiple oral hypoglycemic agents and these medications may also affect the response to infections [13]. Therefore, this review aims to explore the effectiveness and safety of antidiabetic drugs in COVID-19 patients with comorbid Diabetes Mellitus.
DPP4, DPP4 Inhibitors and COVID-19
Dipeptidyl peptidase-4 (DPP4), also known as CD26, is a glycoprotein on the cell surface [14]. This protein is multifunctional and is involved in cytokine production, DNA synthesis, signal activation, and cell proliferation [15]. Interferons upregulate the expression of DPP4 [16]. Interleukin (IL)12 and tumor necrosis factor (TNF)-alpha are involved in the DPP4 translation and translocation [16]. DPP4 also has a role in the induction of hypoxia-inducible factor-1 (HIF-1) alpha, which increases the inflammation [16]. In recent years, the role of DPP-4 in chronic inflammation has been proved [16]. CD26 has a role in regulating the migration and maturation of CD4+T-cell, antibody production, cytokine secretion but the exact role of this protein in immune cells is not clear. CD26+T cells have a strong ability to migrate via endothelial cells [16,17]. So, DPP-4 has a different role in the immune system, such as inflammation-related disease, immune responses, and T cell activation. It also increases inflammation [16]. DPP4 inhibitors, commonly called gliptins, are widely used as effective oral hypoglycemic drugs in the treatment of type-2 diabetes mellitus. However, DPP4 inhibition has the potential to exert a positive pleiotropic effect on vascular and inflammatory diseases [18,19], or even direct anti-inflammatory effect on various cell types: T cells, macrophages, and adipocytes [20]. DPP4 (CD26) inhibitor sitagliptin affect adipocytes and macrophages as an anti-inflammatory agent and exerts anti-inflammatory effects by suppressing NF-κB activation [15,16].
Numerous studies have shown that pro-inflammatory cytokine levels are extremely high in subjects with severe/critical COVID-19. Cytokine storm syndrome (CSS) seems to be of particular concern in patients with severe or critical conditions of infection. COVID-19 patients have high levels of pro-inflammatory cytokines in the lung; thus, blocking circulating IL-6, IL-1, and TNF could be effective for patients in respiratory insufficiency in COVID-19 [20,21]. DPP4/CD26 is variously expressed on epithelia and endothelial of the systemic vasculature, lung, kidney, small intestine and heart. In particular, DPP4 distribution in the human respiratory tract may facilitate the entrance of the virus into the airway tract itself and could contribute to the development of cytokine storm and immunopathology thus causing fatal COVID-19 pneumonia [22]. A recent commentary on Diabetes Research and Clinical Practice described the interplay between the Middle East Respiratory Syndrome (MERS-CoV), another coronavirus responsible for an outbreak of acute respiratory syndrome, and human DPP4 identified as a functional receptor for virus spike protein [23]. It is speculated that membrane-related human DPP4 may also be a functional SARS-CoV-2 receptor. Therefore, the research of DPP4 inhibitors, currently available for type 2 diabetes can be used as a new strategic direction to prevent COVID-19 [24]. Furthermore, as a class of oral hypoglycemic agents, DPP4 inhibitors can effectively reduce glycosylated hemoglobin. Therefore, the research studies of DPP-4 inhibitors have exciting potential for diabetic patients infected with COVID-19 [24]. DPP4 inhibitors may have the anti-inflammatory effect independent of their effect on the GLP-1 level. DPP4 inhibitors are supposed to decrease the expression of CD26 on the immune cell surface, which led to the inhibition of innate immune system activity. Some data suggest that the positive role of DPP4 inhibitors like sitagliptin in controlling the inflammation is due to the increase of GLP-1 [16]. Using existing DPP4 inhibitors (such as sitagliptin, linenegliptin, vildagliptin, etc.) to inhibit the activity of DPP4/CD26 may be an effective weapon to block the host CD26 receptor, thereby blocking SARS CoV2 to enter T cells to prevent infection of COVID-19 [24,25]. With specific respect to lung diseases, Kawasaki et al. demonstrated the direct anti-inflammatory effects of DPP4 inhibition on lipopolysaccharide (LPS)-induced lung injury in mice and in human lung epithelial cells. Similarly, DPP4 inhibitor administration in mice is able to exert protective effects in the lung [20,26]. Telikani et al. have determined serum levels of TNF-α, IL-1 β, and IL-10 in 60 patients with DM; sitagliptin treatment significantly decreased the high levels of pro-inflammatory TNF-α, and at the same time increased anti-inflammatory IL-10 concentrations [27]. Thus, increased plasma DPP4 may represent a driver for clinical severity of SARS-COV2 infection. On one side, the broad DPP4 distribution could contribute to explain the large number of SARS-CoV-2 target organs, which are more than those expressing angiotensin-converting enzyme 2 (ACE2) receptors, identified as the main SARS-CoV-2 receptor so far [28]. One can speculate that DPP4 inhibitors could block an alternative entry site for SARS-CoV-2, thus being beneficial for COVID-19 patients [29]. On the other hand, while binding to soluble DPP4, they could decrease its putative neutralizing/antiviral potential [29]. What is the rationale for postulating link between DPP4 and lower susceptibility to COVID‐19 in children? It has been found that DPP4 may also be released in a soluble form. Possibly, the latter might act as a decoy receptor for viral spike proteins, decreasing the virulence of SARS-CoV-2 [29]. Two observations seem to support this hypothesis. First, it was proven that the level of soluble DPP4 negatively correlated with patient's age. Furthermore, as shown in a small proof of concept study, children were slightly less sensitive to DPP4 inhibitor alogliptin, compared to adults, possibly due to the increased level of soluble DPP4 [29].
Given the already established safety profile of these classes of drugs, and their clinical availability, they might be “repurposed” as potential therapeutic drug candidates for coronavirus pneumonia in DM patients. Interestingly, as gliptins are known to have little or no hypoglycemic effects, they might be used safely in non-diabetic patients [20]. Figure 1.
Metformin and COVID-19
Metformin is a leading first-line anti-diabetic medication, and it is the most commonly prescribed drug for the treatment of DM [8,10]. Metformin has shown anti-inflammatory actions in preclinical studies, and furthermore metformin treatment reduced the circulating levels of inflammation biomarkers in people with DM [30,31]. The results of a study which compared the outcomes in hospitalized Chinese patients showed that mortality was significantly lower in the subjects receiving metformin (2.9% versus 12.3%; P = 0.01) [32]. For individuals with COVID-19 and diabetics, the established beneficial effects of metformin on blood glucose management, cardiac protection, and immune modulation may result in a more beneficial outcome of the viral disease than if metformin use is withheld [10]. However, concerns have been raised regarding the potential side effects of metformin use as it can promote lactic acidosis in individuals with COVID-19 and pre-existing DM, particularly for individuals with severe symptoms of COVID-19 [33]. In addition, the potential of metformin to enhance the expression of ACE2 [34], the viral receptor for SARS-COV-2 [35], has also raised the concern that metformin use may promote the progression of COVID-19. Hence, whether metformin use should be recommended or discontinued in individuals with COVID-19 and pre-existing DM remains highly controversial. Considering the urgency of the COVID-19 pandemic, and the significant number of individuals with COVID-19 and pre-existing DM who could be treated with metformin, information on the clinical impact of its usage in the context of COVID-19 would have significant and immediate implications [10]. Furthermore, metformin use is significantly associated with reduced heart failure as well as an inflammatory response. These findings offer important information to assist clinicians in the decision to use metformin to manage diabetic patients with COVID-19 [10].
Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors and COVID-19
Sodium-glucose cotransporter-2 (SGLT2) inhibitors, inhibit the SGLT-2 protein in the proximal convoluted tubule in the kidney, thereby preventing the uptake of both sodium and glucose to promote their urinary excretion [36]. SGLT2 inhibitors reduce blood levels of glucose. Research studies also suggest the anti-inflammatory effect of SGLT2 inhibitors [37]. In diabetic patients, the treatment with SGLT2 inhibitors reduced infiltration of inflammatory cells into arterial plaques [38] and decreased the mRNA expression levels of some cytokines and chemokines, such as TNF, IL-6 and monocyte chemoattractant protein 1 (MCP1) [39]. However, SGLT2 inhibitors can cause ketoacidosis, especially in critically ill patients[30]. Importantly, SGLT2 inhibitors have profound effects on urinary glucose and sodium excretion, resulting in osmotic diuresis and potentially dehydration. COVID-19 may induce cardiomyopathy and lead to unstable hemodynamics, causing renal ischemia. The natriuretic effect of SGLT2 inhibitors induces blood volume contraction, interferes the hemodynamic stability, and may be detrimental during active COVID-19 disease. Another important concern is that use of SGLT2 inhibitors in patients with diabetes and COVID-19 infection may increase urinary tract infection and diabetic ketoacidosis [30,40]. As such, the use of SGLT2 inhibitors could be difficult in patients under critical care, who need cautious control of their fluid balance.
However, clinicians should consider if SGLT2 inhibitors use would promote virus replication by enhancing intrarenal ACE2 expression in COVID-19 patients, which may lead to deterioration of renal function and further impact the viral activity in the lungs and heart. Unlike Angiotensin-Converting Enzyme Inhibor/Angiotensin Receptor Blockor (ACEI/ARB), the clinical benefits of SGLT2 inhibitors use to improve cardiac and renal outcomes may need more strong evidence to support its irreplaceability. Additional prospective trials are imperative to confirm the advantages and disadvantages of SGLT2 inhibitors in COVID-19 patients, including the combined use with ACEI/ARB. Due to the uncertainty of SGLT2 inhibitors use in patients with COVID-19 infection, an international prospective phase III clinical study (DARE-19) is ongoing to evaluate the effect of dapagliflozin versus placebo, given once daily for 30 days, in reducing disease progression, complications and all-cause mortality in all patients admitted with COVID-19 (Clinicaltrials.gov NCT04350593) [40] The result of this study might help reveal the implications of the use of SGLT2 inhibitors in such patients [30].
Thiazolidinediones and COVID-19
The thiazolidinediones are agonists of the peroxisome proliferator-activated receptor-γ (PPARγ), a nuclear receptor that regulates the transcription of various genes involved in glucose and lipid metabolism [41]. In many studies, thiazolidinediones have been found to reduce insulin resistance and to have putative anti-inflammatory and antioxidant effects, contributing to their anti-atherosclerotic properties [30,42,43]. PPAR-γ agonists attenuated LPS-induced lung injury in murine models [44]. Thiazolidinediones reduce cardiovascular events in terms of recurrent myocardial infarction/stroke in people with DM [45]. However, thiazolidinedione therapy was associated with weight gain and oedema and more importantly was associated with aggravation of heart failure [30]. Increased plasma volume secondary to fluid retention is attributed as cause of heart failure [45]. A significant number of COVID-19 patients, 25% of total cases, develop cardiac complications causing cardiac failure/arrest and death [2,45]. Heart failure is likely to be exacerbated by use of pioglitazone; in fact, it has been associated with significant elevations in Natriuretic peptides. Moreover, pioglitazone has been shown to upregulate ACE2 [45]. These results do not support the use of thiazolidinedione in patients with COVID-19. More clinical trials are needed to optimize the risk–benefit ratio of using thiazolidinediones in patients with COVID-19 [30].
Glucagon-like Peptide 1 (GLP-1) Agonists and COVID-19
Glucagon-like peptide 1 (GLP-1) agonists attenuated LPS-induced lung injury in murine models [46]. Interestingly, the GLP-1 agonist, liraglutide, provoked an increase in ACE2 expression in the lungs of both diabetic and control rats, and in the circulating angiotensin-(1-7) in diabetic animals [47,48]. GLP-1 analogues may interact with the COVID-19 disease process through two key processes [49]; upregulation of ACE2 receptors and anti-inflammatory effects. In rats, use of the GLP-1 analogue liraglutide was associated with upregulation of ACE2 receptors in the cardiopulmonary system [47]. Secondly, the use of GLP-1 analogues is known to improve metabolic health generally at least partly through reducing endovascular inflammation [50]. Indeed, one pre-clinical trial found that use of liraglutide in rats was associated with reduced inflammatory measures, including macrophage infiltration, and reduced TNF-α and IL-6 levels [51]. Based on these findings, it might be proposed that GLP-1 agonist therapy might exert protective effects against SARS-CoV-2 induced lung injury [48]. However, there is a paucity of evidence from human studies in this area [52] and we are not aware of any ongoing trials examining the potential impact of these medications of COVID-19 outcomes [49].
Insulin and COVID-19
Pro-inflammatory cytokines such as TNF-alpha and IL6, disturb the insulin action, which consequently leads to systemic and local insulin resistance [53]. Insulin exerts immunomodulatory effects independent of glycemic control. Several studies suggest a potential benefit of insulin therapy in different animal models of acute lung injury and ARDS. Insulin inhibits synthesis of pro-inflammatory factors, including TNFα and IL-6 and attenuates oxidative stress seen in acute lung injury [48]. Optimal glucose control using an insulin infusion significantly reduced IL-6 and D-dimer levels and improved severity in patients with COVID-19 with or without diabetes mellitus [30,54]. In critically ill COVID-19 patients, the risk of metabolic acidosis associated with metformin might be exacerbated as well as the consequences of volume depletion with SGLT-2 inhibitors. Hence, insulin remains the drug of choice in these situations [14]. Early insulin therapy reduces the risk of developing diabetic ketoacidosis or hyperglycemic hyperosmolar states, taking into account that some diabetic patients with COVID-19 may deteriorate rapidly to acute lung injury and ARDS [48].
Conclusion
COVID-19 is a worldwide pandemic, which has resulted in an extraordinary number of infections and deaths worldwide. People with diabetes are particularly vulnerable to develop more severe forms of the disease. Common pathways appear to exist that may explain the susceptibility of this patient population to COVID-19, and some medications commonly used for people with diabetes may interact with these pathways. The results may be useful for clinical treatment of COVID-19 patients with comorbid diabetes mellitus.
- Mirabelli M, Chiefari E, Puccio L, Foti DP, Brunetti A (2020) Potential Benefits and Harms of Novel Antidiabetic Drugs During COVID-19 Crisis. International journal of environmental research and public health 17: 10.
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z et al. (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395: 1054-62.
- Cheung KS, Hung IFN, Chan PPY, Lung KC, Tso E, Liu R et al. (2020) Gastrointestinal Manifestations of SARS-- CoV-2 Infection and Virus Load in Fecal Samples From a Hong Kong Cohort: Systematic Review and Meta-analysis. Gastroenterology 159: 81-95.
- Bornstein SR, Dalan R, Hopkins D, Mingrone G, Boehm BO (2020) Endocrine and metabolic link to coronavirus infection. Nat Rev Endocrinol 16: 297-8.
- Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q et al. (2020) Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis 94: 91-5.
- Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. J Am Med Assoc 323: 1239-42.
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW (2020) the Northwell COVID-19 Research Consortium, Barnaby DP, Becker LB, Chelico JD, Cohen SL, Cookingham J, Coppa K et al. (2020) Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 323: 2052-9.
- Zhu L, She ZG, Cheng X, Qin JJ, Zhang XJ, Cai J et al. (2020) Association of Blood Glucose Control and Outcomes in Patients with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab 31: 1068-77.e3.
- Bode B, Garrett V, Messler J, McFarland R, Crowe J,Booth R et al. (2020) Glycemic Characteristics and Clinical Outcomes of COVID-19 Patients Hospitalized in the United States. J Diabetes Sci Technol 14: 813-21.
- Cheng X, Liu YM, Li H, Zhang X, Lei F, Qin JJ et al. (2020) Metformin Is Associated with Higher Incidence of Acidosis, but Not Mortality, in Individuals with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab 32: 537-47.e3.
- Chen CF, Chen YT, Chen TH, Chen FY, Yang YP, Wang ML et al. (2020) Judicious use of sodium-glucose cotransporter 2 inhibitors in patients with diabetes on coronavirus-19 pandemic. J Chin Med Assoc 83: 809-11.
- Nakhleh A, Shehadeh N (2020) Interactions between antihyperglycemic drugs and the renin-angiotensin system: Putative roles in COVID-19. A mini-review. Diabetes Metab Syndr 14: 509-12.
- Dalan R (2020) Is DPP4 inhibition a comrade or adversary in COVID-19 infection. Diabetes Res Clin Pract 164: 108216.
- Bouhanick B, Cracowski JL, Faillie JL (2020) French Society of Pharmacology, Therapeutics (SFPT). Diabetes and COVID-19. Therapie 75: 327-33.
- Hu X, Liu S, Liu X, Zhang J, Liang Y, Li Y (2017) DPP-4 (CD26) inhibitor sitagliptin exerts anti-inflammatory effects on rat insulinoma (RINm) cells via suppressing NF-κB activation. Endocrine 55: 754-63.
- Mozafari N, Azadi S, Mehdi-Alamdarlou S, Ashrafi H, Azadi A (2020) Inflammation: A bridge between diabetes and COVID-19, and possible management with sitagliptin. Med Hypotheses 143: 110111.
- Matteucci E, Giampietro O (2009) Dipeptidyl peptidase-4 (CD26): knowing the function before inhibiting the enzyme. Curr Med Chem 16: 2943-51.
- Seferović PM, Coats AJS, Ponikowski P, Filippatos G, Huelsmann M, Jhund PS et al. (2020) European Society of Cardiology/Heart Failure Association position paper on the role and safety of new glucose-lowering drugs in patients with heart failure. Eur J Heart Fail 22: 196-213.
- Cattadori G, Pantanetti P, Ambrosio G (2019) Glucose-lowering drugs and heart failure: implications of recent cardiovascular outcome trials in type 2 diabetes. Diabetes Res Clin Pract 157: 107835.
- Pantanetti P, Cangelosi G, Ambrosio G (2020) Potential role of incretins in diabetes and COVID-19 infection: a hypothesis worth exploring. Intern Emerg Med 15: 779-82.
- Shi Y, Wang Y, Shao C, Huang J, Gan J, Huang X et al. (2020) COVID-19 infection: the perspectives on immune responses. Cell Death Differ 27: 1451-4.
- Solerte SB, Di Sabatino A, Galli M, Fiorina P (2020) Dipeptidyl peptidase-4 (DPP4) inhibition in COVID-19. Acta Diabetol 57: 779-83.
- Iacobellis G (2020) COVID-19 and diabetes: Can DPP4 inhibition play a role?. Diabetes Res Clin Pract 162: 108125.
- Liu Y, Xie H, Gao H, Xie C (2020) Efficacy and safety of DPP-4 inhibitor in the treatment of patients with COVID-19 combined with diabetes mellitus: A protocol for systematic review and meta-analysis. Medicine (Baltimore) 99: e22592.
- Solerte SB, Di Sabatino A, Galli M, Fiorina P (2020) Dipeptidyl peptidase-4 (DPP4) inhibition in COVID-19. Acta Diabetol 57: 779-83.
- Kawasaki T, Chen W, Htwe YM, Tatsum K, Dudek SM (2018) Some of the protective effects of sitagliptin could be mediated through extra-glycemic action, as modulating DPP4/CD26 in rats, the DPP4 inhibition of sitagliptin improves LPS-induced lung injury. Am J Physiol Lung Cell Mol Physiol 315: L834-45.
- Telikani Z, Sheikh V, Zamani A, et al. (2020) Effect of sitagliptin on serum levels of TNF-α, IL-1β and IL-10 in patients with type 2 diabetes mellitus. Koomesh 22: 71-7.
- Barchetta I, Cavallo MG, Baroni MG (2020) COVID-19 and diabetes: Is this association driven by the DPP4 receptor? Potential clinical and therapeutic implications. Diabetes Res Clin Pract 163: 108165.
- Krejner-Bienias A, Grzela K, Grzela T (2020) Do novel drugs for diabetes help in COVID-19? Another brick in the wall?. J Diabetes 12: 703-4.
- Lim S, Bae JH, Kwon HS, Nauck MA (2021) COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nat Rev Endocrinol 17: 11-30.
- Cameron AR, Morrison VL, Levin D, Mohan M, Forteath C, Beall C et al. (2016) Anti-Inflammatory Effects of Metformin Irrespective of Diabetes Status. Circ Res 119: 652-65.
- Luo P, Qiu L, Liu Y, Liu XL, Zheng JL, Xue HY et al. (2020) Metformin Treatment Was Associated with Decreased Mortality in COVID-19 Patients with Diabetes in a Retrospective Analysis. Am J Trop Med Hyg 103: 69-72.
- Bornstein SR, Rubino F, Khunti K, Mingrone G, Hopkins D, Birkenfeld AL et al. (2020) Practical recommendations for the management of diabetes in patients with COVID-19. Lancet Diabetes Endocrinol 8: 546-50.
- Zhang J, Dong J, Martin M, He M, Gongol B, Marin TL et al. (2018) AMP-activated Protein Kinase Phosphorylation of Angiotensin-Converting Enzyme 2 in Endothelium Mitigates Pulmonary Hypertension. Am J Respir Crit Care Med 198: 509-20.
- Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S et al. (2020) SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 181: 271-80.e8.
- Musso G, Gambino R, Cassader M, Pagano G (2012) A novel approach to control hyperglycemia in type 2 diabetes: sodium glucose co-transport (SGLT) inhibitors: systematic review and meta-analysis of randomized trials. Ann Med 44: 375-93.
- Amin EF, Rifaai RA, Abdel-Latif RG (2020) Empagliflozin attenuates transient cerebral ischemia/reperfusion injury in hyperglycemic rats via repressing oxidative-inflammatory-apoptotic pathway. Fundam Clin Pharmacol 34: 548-58.
- Han JH, Oh TJ, Lee G, Maeng HJ, Lee DH, Kim KM et al. (2017) The beneficial effects of empagliflozin, an SGLT2 inhibitor, on atherosclerosis in ApoE -/- mice fed a western diet. Diabetologia 60: 364-76.
- Garvey WT, Van Gaal L, Leiter LA, Vijapurkar U, List J et al. (2018) Effects of canagliflozin versus glimepiride on adipokines and inflammatory biomarkers in type 2 diabetes. Metabolism 85: 32-7.
- Chen CF, Chien CH, Yang YP, Chou SJ, Wang ML, Huo TI, Lin CC (2020) Role of dipeptidyl peptidase-4 inhibitors in patients with diabetes infected with coronavirus-19. J Chin Med Assoc 83: 710-1.
- Yki-Järvinen H (2004) Thiazolidinediones. N Engl J Med 351: 1106-18.
- Li AC, Brown KK, Silvestre MJ, Willson TM, Palinski W, Glass CK (2000) Peroxisome proliferator-activated receptor gamma ligands inhibit development of atherosclerosis in LDL receptor-deficient mice. J Clin Invest 106: 523-31.
- Lim S, Lee KS, Lee JE, Park HS, Kim KM, Moon JH et al. (2015) Effect of a new PPAR-gamma agonist, lobeglitazone, on neointimal formation after balloon injury in rats and the development of atherosclerosis. Atherosclerosis 243: 107-19.
- Grommes J, Mörgelin M, Soehnlein O (2012) Pioglitazone attenuates endotoxin-induced acute lung injury by reducing neutrophil recruitment. Eur Respir J. 40: 416-23.
- Pal R, Banerjee M (2020) Comment on "Is the type of diabetes treatment relevant to outcome of COVID-19?". J Diabetes 12: 705-7.
- Zhu T, Li C, Zhang X, Ye C, Tang S, Zhang W et al. (2018) GLP-1 Analogue Liraglutide Enhances SP-A Expression in LPS-Induced Acute Lung Injury through the TTF-1 Signaling Pathway. Mediators Inflamm 2018: 3601454.
- Romaní-Pérez M, Outeiriño-Iglesias V, Moya CM, Santisteban P, González-Matías LC et al. (2015) Activation of the GLP-1 Receptor by Liraglutide Increases ACE2 Expression, Reversing Right Ventricle Hypertrophy, and Improving the Production of SP-A and SP-B in the Lungs of Type 1 Diabetes Rats. Endocrinology 156: 3559-69.
- Nakhleh A, Shehadeh N (2020) Interactions between antihyperglycemic drugs and the renin-angiotensin system: Putative roles in COVID-19. A mini-review. Diabetes Metab Syndr 14: 509-12.
- Williams DM, Nawaz A, Evans M (2020) Diabetes and Novel Coronavirus Infection: Implications for Treatment. Diabetes Ther 11: 1915-24.
- Rizzo M, Nikolic D, Banach M, Patti AM, Montalto G, Rizvi AA (2014) Incretin-based therapies, glucometabolic health and endovascular inflammation. Curr Pharm Des 20: 4953-60.
- He J, Yuan G, Cheng F, Zhang J, Guo X (2017) Mast Cell and M1 Macrophage Infiltration and Local Pro-Inflammatory Factors Were Attenuated with Incretin-Based Therapies in Obesity-Related Glomerulopathy. Metab Syndr Relat Disord 15: 344-53.
- Pal R, Bhadada SK (2020) Should anti-diabetic medications be reconsidered amid COVID-19 pandemic? Diabetes Res Clin Pract 163: 108146.
- Cai D, Yuan M, Frantz DF, Melendez PA, Hansen L et al. (2005) Local and systemic insulin resistance resulting from hepatic activation of IKK-beta and NF-kappaB. Nat Med 11: 183-90.
- Sardu C, D'Onofrio N, Balestrieri ML, Barbieri M, Rizzo MR, Messina V et al. (2020) Outcomes in Patients With Hyperglycemia Affected by COVID-19: Can We Do More on Glycemic Control? Diabetes Care 43: 1408-15.
FIGURE 1
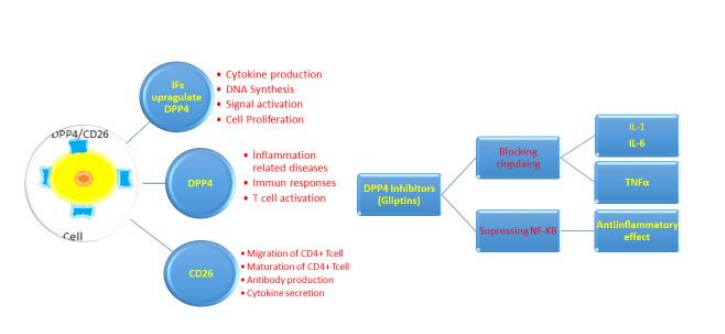
Figure 1: Role of Dipeptidyl peptidase-4 (DPP4) reseptors and effects of DPP4 inhibitors in COVID-19. IFs; interferons, IL-1; Interleukin 1, IL-6; Interleukin 6, and TNFa ; tumor necrosis factor (TNF)-alpha
Figures at a glance