A Comprehensive Review of L-carnitine
Received Date: December 24, 2023 Accepted Date: January 24, 2024 Published Date: January 27, 2024
doi: 10.17303/jmph.2024.3.103
Citation: Nishi Mohile, Dr. Shashikant Bagade, Vanshita Hardiya, Akshita Rana, Krisha Patel (2024) A Comprehensive Review of L-carnitine. J Med Plant Herbs 3: 1-15
Abstract
Due to its essential function in energy metabolism and fatty acid oxidation, l-carnitine has been studied as an ergogenic supplement to increase the amount of activity that healthy athletes can perform. Early studies show that it improves acute physical performance, leading to higher power output and maximum oxygen usage. Subsequent research indicates that taking a l carnitine dietary supplement improves the body's ability to recover from exercise. It has been shown that l-carnitine attenuates muscle soreness and lessens indicators of cellular damage and free radical production in addition to easing muscular injury. It is hypothesized that supplementation-based increases in serum and muscle l-carnitine concentrations will improve endothelial function, improve blood flow, and supply muscle tissue with oxygen, hence lessening the disruptions to cells and biochemistry caused by hypoxia. Additional research on older adults revealed that l-carnitine supplementation can result in a rise in muscle mass, a drop in body weight, and a reduction in both physical and mental exhaustion. According to recent research on animals, l-carnitine may play a part in controlling mitochondrial homeostasis and preventing age-related muscle protein breakdown.
Keywords: L-carnitine; Degradation of L-carnitine; Biosynthesis of L-carnitine
Introduction
The quaternary amine carnitine (ß-hydroxy-trimethyl aminobutyrate), which was initially isolated from muscle in 1905 and given its name from the Latin carnis (flesh or meat), is found in nearly all mammal species as well as several microbes and some higher plants. Glycolysis and other metabolisms depending on carnitine are among the oldest in the history of life. L-carnitine was dubbed Vitamin BT because it functions as a vitamin in the mealworm and in several other larvae in the same family [1]. The proper growth and development of these insects can be ensured by small doses of vitamin BT. But since humans and other higher creatures can synthesis L-carnitine, the term "Vitamin B" is misleading. As a result, L-carnitine is considered a chemical that resembles a vitamin rather than a vitamin. L-- carnitine is a conditionally necessary micronutrient because, in some circumstances, an individual's need for it may outweigh their ability to synthesis it. L-carnitine inside the cell and preventing reactions that are particular to L The whole-body carnitine pool also includes several carnitine esters, the most well-known of which is the short-chain ester acetyl-L- carnitine [1,2]. As the last precursors to trimethyl lysine, the essential amino acids lysine and methionine are used in the liver, kidneys, and brains of mammals to synthesis L-carnitine. In certain species, these organs also include the testes. Many foods also contain L-carnitine, however, the greatest options for including carnitine in the diet are red meats like lamb and beef. Seafood, poultry, and milk are additional excellent sources of carnitine. L-carnitine essentially moves the fatty acid chains into the mitochondrial matrix, enabling the cells to metabolize fat and produce energy from their fat reserves [2].
Sources of L-carnitineSkeletal and cardiac muscle contains almost 90% of the entire carnitine pool; the remaining portion is found in the liver, kidneys, and other tissues. L-carnitine concentrations in skeletal muscles, which serve as the primary reservoir, are at least 50–200 times greater than those in the plasma.The typical concentration in blood ranges from around 41 μM/L in females to 50 μM/L in males. The body needs 15 mg of L-carnitine each day, which is obtained from external sources and endogenous production. Therefore, a modest rate of inner carnitine synthesis, food consumption, and effective renal control of carnitine all contribute to the maintenance of carnitine homeostasis. An adult human organism weighing around 70 kg is normally capable of synthesis of 11–34 mg of L-carnitine daily (160–480 g/kg body weight). However, in terms of stress and physical strain, this quantity may not be adequate, particularly for athletes or sportsmen who have undergone advanced training. Since severe vegetarians do not consume any vegetable protein, they are also likely to be low in L- carnitine, which is mostly found in meats and dairy products. Subnormal blood levels of L- carnitine are also linked to other rare situations involving preterm infants, hemodialysis patients, hereditary abnormalities, or certain chronic conditions. Understanding the amounts of L-carnitine found in various biological components is beneficial when people need exogenous supplementation due to carnitine deficiency. The majority of people take more carnitine than is necessary for apparent maintenance. In humans who are omnivores, a well- designed diet meets around 75% of the daily requirement for carnitine, with only 25% coming from endogenous synthesis. Red meat, especially lamb and cattle, is the main source of L-carnitine. Fish, pork, and chicken, as well as dairy products such as whole milk and cottage cheese, have lesser levels of the amino acid. Products made from plants typically do not have enough carnitine [3,4].
Biosynthesis of L-carnitineHumans can produce L-carnitine through a multi- -step process involving multiple cell compartments using the amino acids lysine and methionine. S-adenosyl-methionine, which is produced from methionine, is the methyl donor in a reaction catalyzed by lysine methyltransferases that methylate protein-bound lysine to form ε-N-trimethyl lysine in various organs. Protein hydrolysis releases ε-NTrimethyl lysine to produce carnitine. The manufacture of endogenous L-carnitine involves four enzymes. All of them are common, except for γ-butyrobetaine hydroxylase, which is not present in skeletal or cardiac muscle.
Nonetheless, the human kidney, testes, and liver all have high levels of expression for this enzyme [5,6].
Since cardiac and skeletal muscles cannot produce L-carnitine on their own, they must receive it from the bloodstream. L-carnitine is mostly produced in the liver and is needed for the oxidation of fatty acids in these muscles. The rate of protein turnover and the degree of methylation of peptide-linked lysine determine the rate of L-carnitine production. Although increases in dietary carnitine intake level or renal reabsorption may boost endogenous Lcarnitine production, excess lysine in the diet may not [7].
Therapeutic use of L-carnitineTreatment with carnitine has been recommended for a wide range of hereditary and acquired illnesses. It can be used to remove harmful metabolites even in cases when plasma and tissue carnitine concentrations are normal, as well as to restore low concentrations in situations linked to deficient states. There are formulations for intravenous and oral use. Even so, there have been few controlled studies and mainly anecdotal accounts of L-carnitine's effectiveness due to the rarity of the majority of the specific illnesses for which it is used. Fortunately, side effects from using L-carnitine are rare and usually mild. Large oral doses can sometimes result in unpleasant fishy smells and diarrhea, although these side effects can typically be avoided by reducing the dosage.
Degradation of L-carnitineEnterobacteria are involved in the conversion of L-carnitine in the gastrointestinal tract when it is taken orally. Pharmacological dosages of carnitine were used in animal research to first show how carnitine breaks down. It has also been seen in humans in circumstances where they consume a typical diet. For aerobic development, L-carnitine can be utilized as a source of both carbon and nitrogen, or it can be employed to preferentially exploit the carbon chain after trimethylamine is broken down. Certain bacteria use carnitine as an electron acceptor through crotonobetaine when they are anaerobic and lack preferred substrates. It has been shown in rats and humans that enteric bacteria can formtrimethylamine and butyrobetaine from L-carnitine (by reducing crotonobetaine). Microbial carnitine dissimilation results in the following end products: trimethylamine in Serratia marcescens, Acinetobacter calcoaceticus, and Pseudomonas putida; glycine betaine in Pseudomonas putida; -butyrobetaine in Escherichia coli, Citrobacter freundii, and multiple Salmonella species; and carbon dioxide and water in Acetinobacter calcoaceticus and Pseudomonad putida [8,9].
L-Carnitine DeficiencyTransfer of long chain fatty acids to the mitochondrial matrix for oxidation requires carnitine. Fatty acids become the main substrate for energy production during fasting times, when they are oxidized in the liver, heart muscle, and skeletal muscle. 60% of muscle oxygen use during extended aerobic exercise is accounted for by fatty acid oxidation. Instead of using fatty acids directly for oxidative metabolism, the brain oxidizes ketones made from acetyl CoA and acetoacetyl CoA, which are produced by the liver's fatty acid oxidation. Deficiency is brought on by an inadequate amount of carnitine in the blood, and this can contribute to a variety of hereditary and acquired illnesses.(9) An autosomal recessive fatty acid oxidation condition resulting from impaired carnitine transport is primary carnitine deficiency. This illness manifests itself either early in childhood as hypoketotic hypoglycemia, which is caused by depletion of glucose reserves an alternate substrate to fatty acids or later in life as cardiomyopathy or skeletal myopathy [9].
There are two main forms of carnitine deficiency that have been identified: myopathic (MCD) and systemic (SCD). Low levels of carnitine in plasma and specific tissues, along with lipid deposit deposition and renal carnitine leakage, are the hallmarks of sickle cell disease (SCD). This particular condition is becoming recognized as a potential cause of very low birth weight or even sudden infant death syndrome. It is characterized by progressive cardiomyopathy and skeletal muscle failure, where fatty acids comprise a basic energy source. Particularly preterm babies have little fat reserves and frequently need their parents' prolonged nourishment, which includes emulsified lipids to provide growth-promoting calories and vital fatty acids. Lipid buildup in the muscles and mild to severe muscular weakness are characteristics of MCD. Although the concentration of carnitine in skeletal muscle is low, the levels of carnitine in plasma and liver are normal.
Secondary causes of low levels of L-carnitine in the diet include dialysis therapy, diabetes, mitochondrial myopathy, inborn errors of metabolism, specifically metabolic defects in fatty acid oxidation, and inadequate absorption from the gastrointestinal tract. Vegetarians may experience a carnitine shortage due to an inadequate food intake. Furthermore, despite the presence of substrate amino acids in parenteral nutrition fluids, prior research has demonstrated that newborns receiving carnitine-free parenteral nutrition are unable to synthesize enough carnitine to maintain plasma concentrations equivalent to those found in healthy newborn infants or older children. Low plasma free carnitine levels and high total carnitine levels are also possible in patients with alcoholism and ketosis, primarily as a result of elevated.
Effect of L-Carnitine in Fatty Acid MetabolismIn order for free long-chain fatty acids to be converted to acylcarnitine and then transported into the mitochondrial matrix, l-carnitine is a cofactor of multiple enzymes, including acylcarnitine transferases I and II and carnitine translocase. These molecules undergo fJ- oxidation before entering the Krebs cycle, which is where energy production takes place.
Lack of l-carnitine causes the buildup of free fatty acids in the cytoplasm to be toxic to the cell, and the inability of the mitochondria to generate fatty acids results in an energy shortage.
Synthesis of L-carnitine
The Chemical Optical Resolution MethodChemical optical resolution methods state that diastereomers are produced when an optically pure chiral optical resolution agent reacts with D, L-carnitine, or the racemate of its derivatives. The difference in solubility in a suitable solvent is then used to resolve the target diastereomers. The target L-carnitine is produced by hydrolyzing the aforementioned molecule once more. D-camphoric acid, L-tartaric acid, dibenzoyl-D-tartaric acid, dibenzoyl- L-tartaric acid, D-mandelic acid, and N-acetyl-D-glutamic acid are among the frequently used optical resolution agents [10].
Several chemical processes have been suggested for the large-scale synthesis of carnitine. To create two diastereomers that can be separated from one another, the D, L-racemic mixture is typically treated with an optically active acid, such as D-(-)-tartaric acid, D-(+)-camphor- sulfonic acid, (+)-dibenzoyl-D-(-)-tartaric acid, Nacetyl-L-(+)-glutamic acid, and D-(+)- camphoric acid. D-(+)-camphoric acid is utilized as a resolution agent in a racemic combination of D and L-carnitine in the traditional process outlined in U.S. Patent 4,254,053, producing L-(-)-carnitinamide, which is hydrolyzed to generate L-(-)-carnitine, and D-(+)- carnitinamide as a by-product. Nevertheless, a lot of resolution processes are difficult and
expensive, and they always produce equimolar amounts of D-(+)-carnitine or a precursor as a by-product, which has the opposite configuration of L-(-)-carnitine [11].
The Biological Method
The biological technique of making L-carnitine involves the use of enzymes or microbes. Stereo-selective hydroxylation of butyrobetaine with relevant enzymes or stereo-selective hydration of crotonobetaine with relevant enzymes are the two methods used to manufacture L-carnitine from raw materials [11].
Microorganisms capable of converting crotonobetaine into L-carnitine act in an aqueous media to convert crotonobetaine to L-carnitine. A bacterium that can convert crotonobetaine into L-carnitine is defined as one that, when exposed to crotonobetaine in the following circumstances, generates L-carnitine through the action of the microorganism's enzymes on the substrate crotonobetaine,A strain DSM number 3225 (HK 1331b) microorganism is cultured in a bioreactor with growth substrate in the presence of crotonobetaine and/or γ- butyrobetaine [11,12].
The culture fluid is directed outside the bioreactor in a circulation that performs a cell separation. L-carnitine is separated from the cell-free solution by withdrawing a volume of the solution from the bioreactor that is equal to the amount supplied as a substrate. Utilizing the benefits of the novel operating method, the continuous process's biomass retention, increased productivity, and significantly enhanced long-term stability.
An other biological technique for obtaining L-carnitine involves the interaction between trimethylamine and (R)-3,4-epoxybutyric acid. A racemic 3,4-epoxybutyric acid ester is produced by a chemical reaction starting with (R)-3,4-epoxybutyric acid as the primary raw material [11].
Such an ester, according to the biological process, is optically resolved to selectively yield a (R)-3,4-epoxybutyric acid ester, which is then hydrolyzed once more to yield the desired molecule. Excellent stereo-selectivity has been demonstrated by this approach, even though it necessitates precise reaction modulation and a lengthy reaction period of about 24 hours [12].
Use Chiral Material from the Natural SourceThere is a way to make L-carnitine using chiral material derived from a natural source. D- mannitol is utilized as a raw ingredient in this process.Then, L-carnitine is made by a series of stages. There is now a different way to make L-carnitine from (S)-3-activated hydroxybutyrolactone. This approach involves mixing a 25% trimethylamine solution of 2.0 equivalent with (S)-3-activated hydroxybutyrolactone of 1.0 equivalent. After that, the mixture is mixed for an hour at room temperature in a tight container. Furthermore, the combination is reacted for 16 hours at 100 °C to obtain pure L-carnitine; however, the yield is not stated.
(S)-3-activated hydroxybutyrolactone yields L-carnitine. Using traditional chemistry, (S)-3- hydroxybutyrolactone (S-HGB), often referred to as (S)-3-activated hydroxybutyrolactone (S-HGB), is an essential building block for the production of additional chiral intermediates. Gamma-butyrolactone (S)-3-hydroxyl is a type of crucial intermediate in chemical synthesis. Additionally, it is a crucial chiral source (Chira Pool) [11].
(S)-3-hydroxy-γ butyrolactone (S-HGB) can be used to synthesize ezetimibe and linezolid, and it is a precursor to several enantiopure intermediates for chiral medicines, including cholesterol-lowering medications. In synthetic organic chemistry, enantiopure (S)-3-hydroxy- γbutyrolactone and its structurally related C3-C4 compounds are a key target for chiral building blocks [20]. The alcohols and carboxylic acids in optically pure HGBs can be further derived. Among other things, S-HGB can be transformed into (S)-4-Chloro-3- hydroxybutyrate (S-CHB) and then into hydroxy-nitrile (HN) for the manufacture of Lcarnitine, 4-hydroxy-2-pyrrolidone, oxazolidinones, and intermediates of hydroxy-methyl- glutaryl-CoA (HMG-CoA) reductase inhibitors.
The Process used in the Production PlantEpichlorohydrin and trimethylamine are two inexpensive basic ingredients that are typically used in the chemical production of L-carnitine. After the race mate's separation by processes like fractional crystallization. At this stage, optical resolution is challenging. The biotechnological method of producing L-carnitine is more efficient than the chemical method in terms of procedure. Reports state that compared to chemical operations, biotechnological techniques produce 90% less trash for incineration, 25% less wastewater, and about 50% less total organic waste. Consequently, the manufacture of L-carnitine by microorganisms has become more popular [13].
Researchers decided to use the L-carnitine preparation method of (S)-3-activated hydroxybutyrolactone based on comparisons of the available methods. This is because a very simple and low-cost method of preparing (S)-3-activated hydroxybutyrolactone has been developed, which involves oxidizing and successively cyclizing inexpensive natural D- carbohydrates and hydrogen peroxide [13]. There should be a certain prerequisite for (S)-3- activated hydroxybutyrolactone as a raw material. Using this technique, it will be possible to obtain very pure and high yields of L-carnitine by using inexpensive chemicals in aqueous solutions [13].
(S)-3-activated hydroxybutyrolactone undergoes a ring-opening reaction as the initial reaction step. In the following phase of the reaction, the ring-opened molecule of 4- hydroxy3-activated hydroxybutyric acid experiences an epoxidation reaction wherein the presence of a base causes a stereospecific reversal of the chiral center. From there, a salt of 3,4-epoxybutyric acid that is optically pure is made. The final stage of the reaction process is the reaction of (R)-3,4-epoxybutyric acid with trimethylamine to produce L-carnitine. The procedure above produced sodium 3,4-epoxybutyrate, which was not isolated from an aqueous solution containing 25% trimethylamine equivalent was added right away to the reagent solution, and L-carnitine was produced by stirring it for two hours at 45°C
L-carnitine can be extracted and purified from reagent solution using a well-known technique, ideally one that involves cation exchange resin. The optical purity of L-- carnitine obtained with the cation exchange resin method of separation and purification is more than 95%, with a yield of at least 55%. Moreover, a similar outcome can be achieved by reacting trimethylamine with sodium 3,4-epoxybutyrate, which is created during the reaction of epoxybutyric acid.
Four process units go into the creation of L-carnitine. The following are the process units: sodium (R)-3,4-epoxybutyrate preparation, L-carnitine preparation, (S)-3- methanesulfonyl hydroxybutyrolactone preparation, and (S)-4-hydroxy-3-methanesulfonyl hydroxybutyric acid preparation [13].
Reaction of L-carnitine on Various Diseases Male infertilityNumerous investigations have verified increased reactive oxygen species (ROS) overproduction in prostato-vesiculoepididymitis individuals. Moreover, a lower sperm count is associated with a lower level of L-carnitine. Because of this, the use of L-carnitine is advised in the treatment of male infertility, and since the initial controlled and uncontrolled trials, extremely encouraging outcomes have been obtained. There was a considerable reduction in both baseline and provoked ROS generation with the combined use of carnitines, specifically carnitine and acetyl-carnitine complex. Similar to several antioxidants, carnitine/acetyl-- carnitine combination appears to have a restorative effect by either replacing fatty acids in membrane phospholipids or removing increased intracellular harmful acetyl- coenzyme A (acetyl-CoA) [14,15].
Terminate Renal DiseaseHemodialysis eliminates L-carnitine and shortand medium-chain acylcarnitine molecules from the bloodstream. Patients with end-stage renal disease (ESRD) receiving hemodialysis are at risk for developing a progressive carnitine shortage due to a combination of factors, including L-carnitine loss into the dialysate and reduced kidney production. A increased risk of cardiovascular mortality has been linked to a high acylcarnitine-to-L-carnitine ratio, which is caused by inadequate clearance of long-chain acylcarnitine molecules [16,17]. Patients receiving hemodialysis may experience a number of disorders as a result of carnitine depletion, including refractory anemia, anomalies in plasma lipid levels, and weakness and exhaustion of the muscles. Serum C-reactive protein, a marker of inflammation and a predictor of death in patients receiving hemodialysis, and LDL cholesterol decreased when L- carnitine treatment was given orally or intravenously, according to a 2014 systematic review and meta-analysis of 31 randomized controlled trials involving 1,734 patients with ESRD, though the latter was not considered to be significant to be clinically relevant. Other serum lipids (such as total and HDL cholesterol, triglycerides) and anemia-related markers (such as hemoglobin concentration, hemoglobin-related erythropoietin-requiring dose, albumin, and hemoglobin-to-crit ratio) were not affected by L-carnitine [16].
Effect on Heart FailureThe incapacity of the heart to pump enough blood to meet all of the body's requirements is known as heart failure. The buildup of atherosclerotic plaque in the coronary arteries may cause coronary heart disease by preventing the heart's inner regions from receiving enough blood flow, which can lead to cardiac injury and reduced pumping capacity.Heart failure may result from myocardial infarction-related damage to the heart muscle. Furthermore, heart failure may result from the heart's reduced ability to pump blood in dilated cardiomyopathy situations [18]. Measures of exercise tolerance are widely used to track the severity of heart failure since exercise puts more strain on the already compromised heart.The left ventricular ejection fraction (LVEF), an objective indicator of the heart's pumping capacity, is also calculated via echocardiography. Systolic heart failure is indicated by an LVEF of less than 40%. Patients with heart failure who have aberrant acylcarnitine profiles and high acylcarnitine to free carnitine ratios in their blood have been associated with severe illness and a bad prognosis [18].
Effect on Bone MassAs people age, their cells' concentration of carnitine decreases, which has an impact on different tissues' fatty acid metabolism. Bones that depend on osteoblasts for ongoing metabolic and reconstructive processes to maintain bone mass are particularly badly impacted [19]. Osteoporosis is a common condition in the elderly, although it primarily affects women who have gone through menopause. Patients with osteoporosis are more likely to fracture because their bone is more brittle as a result of disturbed bone microarchitecture. It was discovered that giving animals a carnitine mixture—which contains propionyl L- carnitine or one of its pharmacologically acceptable salts—could raise the concentrations of osteocalcin in their serum. In contrast, serum osteocalcin levels in control animals tended to decline with age [20].
Our carnitine levels decrease with aging. Patano and colleagues suggest that this age-related decrease in energy availability may have deleterious effects on osteoblast activity and bone remodeling. Research has shown that fatty acid oxidation produces 40–80% of the energy needed for osteoblastic lineage cells. This implies that regulating the oxidation of fatty acids could regulate the amount of energy accessible to osteoblasts for the creation of proteins [20]. Researchers found that L-carnitine supplementation can affect bone density and minimize bone turnover by decreasing bone loss and boosting bone microstructural characteristics through the use of an aged ovariectomized rat model [21].
Cardiovascular Disease
Patients with severe cardiovascular conditions, such as coronary heart disease, chronic heart failure, and peripheral vascular disease, have been demonstrated to benefit from L-carnitine. Giving L-carnitine to individuals with chronic heart disease during a 12-month period avoided ventricular remodeling and attenuated left ventricular dilatation, which in turn decreased the risk of chronic heart failure and mortality. L-carnitine improves glucose metabolism and lessens the toxicity of elevated free fatty acid levels to lessen cardiac damage during ischemia.(22) It has been established that L-carnitine protects against ST-elevation myocardial infarction. Prompt L-carnitine delivery after an acute myocardial infarction and ongoing maintenance therapy attenuate. gradual dilatation of the left ventricle. At six months, L-carnitine lowers early mortality but not the total risk of death or heart failure. In addition, supplementing with L-carnitine decreases the size of infarcts and cardiac biomarkers, prevents ventricular hypertrophy and dysfunction, and lowers the overall frequency of cardiac events, which includes nonfatal infarction and cardiac fatalities. According to Xue and colleagues, the restoration of myocardial energy stores and the start of normal oxidative metabolism are the reasons behind L-carnitine's positive benefits in cardiovascular disease [23].
It is commonly advised to take supplements containing carnitine if you have cardiovascular disease. But as previously noted, carnitine supplementation exacerbates both injury and recovery of contractile function following brief ischemia in the perfused rat heart when it does not enhance glucose oxidation [23].
Drug InteractionsL-carnitine losses are increased when pivalic acid combines with L-carnitine and is eliminated in the urine as pivaloylcarnitine (see also Secondary carnitine deficit). As a result, extended usage of antibiotics containing pivalic acid, such as cefditoren pivoxil pivampicillin, pivmecillinam, and pivcephalexin, might result in secondary L-carnitine insufficiency. When combined with L-carnitine, the anticonvulsant valproic acid (Depakene) creates a valproylcarnitine ester, which is eliminated in the urine. This disruption of Lcarnitine production occurs in the liver. However, only a small percentage of valproic acid users require L-carnitine supplementation. Young age (less than 2 years), significant neurological issues, usage of many antiepileptic medications, poor nutrition, and ketogenic diet intake are risk factors for L-carnitine shortage with valproic acid.
Reaction to Muscle injury of L-CarnitineMuscle soreness and injury brought on by exercise can both lower quality of life and restrict training. L-carnitine has been shown to improve exercise performance in addition to aiding in post-exercise recovery through a variety of methods. On the other hand, performance during a second round of intense cycling exercise after three hours was not enhanced by a single administration of l-carnitine [24,25].
L-carnitine supplementation was found to reducediscomfort, soreness, and the release of creatine kinase, a muscle marker, in a cross-over trial. This suggests that the vitamin is beneficial in preventing tissue rupture and the resultant leaking of cytosolic proteins [26]. The beneficial effects of l-carnitine on lowering exercise-induced hypoxia, ensuing muscle damage, and delayed onset muscle soreness (DOMS) were further supported in a series of studies conducted by Kraemer and colleagues [27]. It was possible to show that daily use of 2 g l-carnitine, as opposed to a placebo, decreased muscle disruption during intense exercise using the magnetic resonance imaging (MRI) technique [18]. Along with this, there was a notable drop in purine metabolism indicators including hypoxanthine and xanthine oxidase, as well as released cytosolic proteins such myoglobin, creatine kinase, and malondialdehyde (MDA) [28]. In one investigation, the effects of two distinct l-carnitine dosages on these metabolic indicators and the subjective perception of muscle soreness were compared [29]. The researchers found that supplementing with 1 g and 2 g of l- carnitine daily produced similar advantages, adding to the body of evidence supporting the supplement's potential.The researchers also found that over three weeks, supplementing with l-carnitine l-tartrate, or 2 g of l-carnitine daily, increases the amount of androgen receptors on muscle cells, which enhances protein signaling, which is necessary for muscle cell repair and post-exercise recovery [30].
Reaction on Blood Flow and Endothelial FunctionBy guarding against carnitine deficit in endothelial cells, l-carnitine supplementation decreased structural and biochemical muscle damage and facilitated tissue repair, improving blood flow and oxygen supply.(30) Dubelaar and Hülsmann's early research served as the foundation for the new paradigm [31,32]. Here, it was shown that, both in the absence of enhanced muscle l-carnitine level and upon l-carnitine infusion, dogs' muscle contractile force was markedly boosted and accompanied by an elevated blood flow [32]. Furthermore, during ischemia, l-carnitine extends endothelial cells' capacity to control blood flow. This suggested a process separate from the accumulation of muscle l-carnitine and energy generation. The authors postulated that enhanced force resulted from a change in the capillaries encircling the muscle [32].
Nuesch et al.'s findings confirmed this vascular effect. It was demonstrated that following maximal exercise, plasma carnitine levels in athletes taking 1 g of l-carnitine remained elevated as opposed to significantly declining in athletes not taking supplements [33]. In a cross-over study, Volek et al. looked into the flow-mediated dilation (FMD) following a high-fat meal to learn more about the impact of l-carnitine on endothelial cell function.
Following three weeks of l-carnitine supplementation, peak FMD reduced in the placebo arm but post-prandial brachial artery FMD rose in response to a five-minute upper arm occlusion [33]. These findings provide credence to the theory that l-carnitine improves vascular function by modulating endothelial function [33].
L-Carnitine as an Anti-OxidantThe function of l-carnitine supplementation in reducing oxidative stress during exercise is one of the possible processes underlying this effect. Muscle damage is mostly brought on by acute cellular and structural injury as well as following biochemical reactions during tissue regeneration, particularly during eccentric exercise (active force producing lengthening contractions) [34,35]. Long-term dysfunction can result from modifications to the surrounding tissue and sarcomeres of muscle fibers, allowing the healing process to last up to ten days. By distancing ATP synthesis from the Krebs cycle from cell energy use, local hypoxia brought on by exercise may potentially exacerbate inflammation and muscle damage [36].
Reactive oxygen species may occur as a result of this (ROS). In the end, the release of intracellular components into the interstitium and the ensuing inflammation cause DOMS, which is characterized by discomfort, edema, and rigidity of the muscles in addition to pain when moving [16]. These events are caused by molecules like MDA, hypoxanthine, or creatine kinase that are produced when sarcolemma rupture occurs. Parandak et al. also reported on the antioxidant benefits of l-carnitine on exercise-induced oxidative stress. When compared to a placebo before and 24 hours after exercise, daily administration with 2 g l- carnitine over 14 days significantly enhanced total antioxidant capacity. However, indices of muscle injury and lipid peroxidation remained significantly lower [16]. Additionally, Parthimos et al. discovered that l-carnitine administration after training enhanced the overall antioxidant status that basketball players otherwise showed in the absence of supplementation [16].
Ho and colleagues initially presented experimental evidence indicating a positive impact on recovery after exercise in middle-aged healthy men and women, with an average age of 45 and 52, respectively [17]. However, the majority of these investigations were conducted in young, healthy volunteers. L-carnitine supplementation, once again, attenuated a rise in stress markers during and after exercise, such as muscle pain as reported by the individuals [17].
Reaction of L-Carnitine on AgingAging might offer insights into the future course of l-carnitine research and application. Although studies on the benefits of l-carnitine ingestion in physically demanding conditions have shown that the healthy young to middle-aged population can benefit from it, the effects of l-carnitine intake in physically exhausted senior individuals are still unknown. Sarcopenia is the name for the age-related decrease in skeletal muscle mass, strength, and general activity. It is a complex age-related disorder. Sarcopenia is caused by various factors, including reduced mobility, poor nutritional health, and a deterioration in mitochondrial activity [37].
As sarcopenic subjects age, changes in protein metabolism and a decrease in protein synthesis have been documented [38]. While the balance of proteolytic and anabolic processes controls protein metabolism in young, healthy persons, sarcopenia results in a lack of sufficient protein synthesis and increasing breakdown, which in turn causes physical weakness in elderly individuals [37]. According to a recent study using the nematode Caenorhabditis elegans, some aggregation proteins may be involved in the age-related decrease of muscular mass. A further process contributing to the age-related decrease of muscle mass is the progressive reduction in anabolic stimulus sensitivity. Furthermore, the loss of type II fibers was linked to this deterioration in the elderly [39].
Diet and physical activity are two factors that can affect sarcopenia. It has been demonstrated that eating meat and resistance training work in concert to improve older people's muscle endurance and strength as well as their ability to synthesize muscle proteins [40]. Furthermore, senior citizens' physical performance can be enhanced and their muscle growth and strength increased with supplemented protein intake. Nevertheless, additional research revealed that protein doesn't improve muscle development and function in this population on its own or in the absence of exercise [40].
An increasing body of research indicates that l-carnitine can reverse the age-related decline in muscular function and have a favorable impact on muscle hypertrophy. In healthy individuals, there is a documented decrease in muscle l-carnitine content as people age.
Additionally, aging results in decreased transcription of the l-carnitine transporter, OCTN2 mRNA [40], suggesting that aging impairs the distribution and homeostasis of l-carnitine in tissues. As a result, several research looked into the part l-carnitine plays in aging
Malaguarnera et al. conducted a 6-month clinical trial on centenarians who were given a placebo or 2 g of l-- carnitine daily to examine the impact on both physical and mental exhaustion. Supplementation produced better walking ability, decreased total fat mass, and increased muscle mass as compared to the placebo group, indicating a positive impact in this demographic [41]. These results are consistent with other studies conducted by the same group which demonstrated that muscle mass grew while body fat mass decreased in the elderly. Alongside this, there was a noticeable decrease in both physical and mental exhaustion [42]. Supplementing with acetyl-l-carnitine, the acetylated derivative of l- carnitine, also lessened both physical and mental exhaustion in subjects 70 years of age and above. Pre-frail older people with a mean age of 68 years were included in a double-blind, randomized, placebo-controlled clinical trial by Badrasawi et al., which demonstrated a substantial improvement in frailty status after giving 1.5 g l-carnitine daily for 10 weeks [43]. A recent study by Evans et al. shown the beneficial effects of L-carnitine, creatine, and leucine on muscle mass and performance [43].
After eight weeks of supplementation, researchers compared the possible synergistic effect of this unique for mulation to a placebo in this randomized, placebo-controlled, double blind study involving individuals ages 55–70. In comparison to a placebo, it was discovered that patients considerably increased overall lean muscle mass, leg lean muscle mass, and leg strength as well as improved a composite outcome measure of body mass, muscular strength, and a 6-minute walk test. Supplementing with l- carnitine alone did not significantly increase the composite parameter when compared to placebo; however, subjects maintained their leg muscular strength and composite score relative to baseline, while both dropped during the course of the research in the placebo group.
Even though several studies in the younger population were unable to demonstrate weight loss following l-carnitine intake, Pooyandjoo, and colleagues concluded in a recent meta- analysis that subjects receiving l-carnitine experienced a significant reduction in body weight when compared to the control groups [44]. The majority of the research that made up the meta-analysis involved patients who were obese or diabetic [44].
Some of the general mechanisms of action of l-carnitine effects demonstrated in animal studies and younger athletes can apply, even if the processes behind the effects of l-carnitine in boosting muscle development and function in older persons are yet unknown.
Supplemental l-carnitine spared amino acids by turning fat into energy, which resulted in swine muscle protein accumulation [45]. A possible method by which l-carnitine inhibits the breakdown of muscle protein is indicated by Keller and colleagues' demonstration of the role of l-carnitine in the transcriptional control of genes involved in the ubiquitin proteasome system of the piglet's skeletal muscle. Furthermore, it has been documented that l-carnitine raises IGF-1 and Akt, which triggers the mammalian target of rapamycin (mTOR) signaling pathway, a crucial regulator of protein anabolism [46].
Peroxidative damage accelerates the aging process, according to the free radical hypothesis of aging. Reactive oxygen species can be scavenged by antioxidants or their creation can be stopped, reducing oxidative stress. Numerous clinical investigations have demonstrated the antioxidant qualities of l-carnitine, pointing to a possible new mechanism of action by which l-carnitine may prevent the metabolic processes responsible for tissue aging [47,48]. Accelerated neuronal cell damage and death, which results in brain shrinkage and a reduction in brain function, is another feature of aging. It was proposed that the main underlying process might be mitochondrial degradation. Nicassio et al. have proposed that acetyl-l- carnitine affects mitochondrial homeostasis in the brains of aged rats [49].
Conclusion
Scientific research has examined the role of l-carnitine in various indications, as it is an important component in energy production and fatty acid metabolism. Professional athletes have utilized l-carnitine as an ergogenic aid, and physically active people have used it as a nutritional supplement. Many human studies with resistance-trained athletes, untrained men and women, or healthy active people looked at how the dietary supplement affected muscle strength, oxygen capacity, or physical performance. Clinical research has recently focused on testing the theory that l-carnitine supplementation speeds up the healing process following physical activity. According to scientific research, l-carnitine supplementation can help athletes since it lessens the negative effects of high-intensity training by lowering the degree of exercise-induced hypoxia and muscle injury.
Fatty acid β-oxidation is not limited by the supply of l-carnitine when conditions are healthy and stress-free. Urinary excretion, transport, and bioavailability all play a major role in controlling its homeostasis. However, l-carnitine supplementation has been demonstrated to improve endurance and muscle tone and function in circumstances characterized by aberrations, such as hemodialysis, inborn or acquired carnitine deficit, and sarcopenic and frail patients. Both exercise and dietary changes can stop the age-related loss of muscle mass. While moderate exercise combined with dietary supplements may be a potential method to slow down the onset of sarcopenia, a characteristic of frailty in older persons, endurance exercise can be difficult for the elderly. An increasing amount of research conducted on animals has demonstrated the complex processes through which l-carnitine promotes greater protein synthesis and less muscle breakdown. Furthermore, age-related reductions may be influenced by l-carnitine's modulation of mitochondrial homeostasis during aging. Thus, by delaying the rate at which muscle mass and function loss and neurodegeneration occur, dietary supplements containing l-carnitine may benefit during the aging process. In this area, more investigation is necessary. In summary, the structural and symptomatic effects of high- intensity exercise, such as pain and impaired muscle sarcomeres, not only lower quality of life but also limit the ability to train further. For this reason, l-carnitine supplementation that promotes recovery from exercise is especially advantageous for the healthy, young, active population. Furthermore, older adults who are losing lean muscle mass and function, have lower muscle l-carnitine levels, and have mitochondrial dysfunction can also gain from taking a l-carnitine supplement. In instance, the value of l-carnitine in this population will only increase as more older participants engage in moderate activity
- Alesci S, De Martino MU, Mirani M, Benvenga S, Trimarchi F, Kino T, et al. (2003) l‐Carnitine: a nutritional modulator of glucocorticoid receptor functions 17: 1‐20.
- Peluso G, Barbarisi A, Savica V, Reda E, Nicolai R, Benatti P, et al. (2001) Carnitine: an osmolyte that plays a metabolic role 80: 1‐10.
- Rebouche CJ, Chenard CAJTJon (1991) Metabolic fate of dietary carnitine in human adults: identification and quantification of urinary and fecal metabolites 121: 539‐46.
- Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheehy BT, et al. (2013) Intestinal microbiota metabolism of L‐carnitine, a nutrient in red meat, promotes atherosclerosis 19: 576‐85.
- Karlic H, Lohninger AJN (2004) Supplementation of L‐carnitine in athletes: does it make sense? 20: 709‐15.
- Bremer JJPr (1983) Carnitine‐‐metabolism and functions 63: 1420‐80.
- Brass EPJCt (1995) Pharmacokinetic considerations for the therapeutic use of carnitine in hemodialysis patients 17: 176‐85.
- Koepsell HJTips (2004) Polyspecific organic cation transporters: their functions and interactions with drugs 25: 375‐81.
- Bain MA, Faull R, Milne RW, Evans AMJCdm (2006) Oral L‐carnitine: metabolite formation and hemodialysis 7: 811‐6.
- Erich S, Irmgard L (1964) Production of pure d‐and l‐carnitinenitrile‐chloride. Google Patents.
- Yokozeki K, Kubota K (1989) Method for producing L‐carnitine. Google Patents.
- Bernal V, Sevilla Á, Cánovas M, Iborra JLJMCF (2007) Production of L‐carnitine by secondary metabolism of bacteria 6: 1‐17.
- Brass J, Hoeks F, Rohner MJJoB (1997) Application of modelling techniques for the improvement of industrial bioprocesses 59: 63‐72.
- Benvenga S, Amato A, Calvani M, Trimarchi FJAotNYAoS (2004) Effects of carnitine on thyroid hormone action 1033: 158‐67.
- Sheweita SA, Tilmisany AM, Al‐Sawaf HJCdm (2005) Mechanisms of male infertility: role of antioxidants 6: 495‐ 501.
- Cleak M, Eston RJBjosm (1992) Muscle soreness, swelling, stiffness and strength loss after intense eccentric exercise 26: 267‐72.
- Ho J‐Y, Kraemer WJ, Volek JS, Fragala MS, Thomas GA, Dunn‐Lewis C, et al. (2010) l‐Carnitine l‐ tartrate supplementation favorably affects biochemical markers of recovery from physical exertion in middle‐aged men and women 59: 1190‐9.
- Kraemer WJ, Volek JS, French DN, Rubin MR, Sharman MJ, Gómez AL, et al. (2003) The effects of L‐ carnitine L‐tartrate supplementation on hormonal responses to resistance exercise and recovery 17: 455‐62.
- Liu J, Head E, Gharib AM, Yuan W, Ingersoll RT, Hagen TM, et al. (2002) Memory loss in old rats is associated with brain mitochondrial decay and RNA/DNA oxidation: partial reversal by feeding acetyl‐ L‐carnitine and/or R‐α‐ lipoic acid 99: 2356‐61.
- Hooshmand S, Balakrishnan A, Clark RM, Owen KQ, Koo SI, Arjmandi BHJP (2008) Dietary l‐carnitine supplementation improves bone mineral density by suppressing bone turnover in aged ovariectomized rats 15: 595‐601.
- Koverech A, Zallone A (2005) Use of isovaleryl L‐carnitine to increase healing of bone fractures. Google Patents.
- Fagher B, Cederblad G, Monti M, Olsson L, Rasmussen B, Thysell HJSJoC, et al. (1985) Carnitine and left ventricular function in haemodialysis patients 45: 193‐8.
- Spagnoli LG, Corsi M, Villaschi S, Palmieri G, Maccari FJTL (1982) Myocardial carnitine deficiency in acute my ocardial infarction 319: 1419‐20.
- Maggini S, Banziger K, Walter PJAoN, Metabolism (2000) L‐Carnitine supplementation results in improved recovery after strenuous exercise‐A preliminary study 44: 86‐8.
- Stuessi C, Hofer P, Meier C, Boutellier UJEjoap (2005) L‐Carnitine and the recovery from exhaustive endurance exercise: a randomised, double‐blind, placebo‐controlled trial 95: 431‐5.
- Giamberardino MA, Dragani L, Valente R, Di Lisa F, Saggin R, Vecchiet LJIjosm (1996) Effects of prolonged L‐carnitine administration on delayed muscle pain and CK release after eccentric effort 17: 320‐4.
- Volek JS, Kraemer WJ, Rubin MR, Gómez AL, Ratamess NA, Gaynor PJAJoP‐E, et al. (2002) L‐Carnitine L‐tartrate supplementation favorably affects markers of recovery from exercise stress.
- Spiering BA, Kraemer WJ, Hatfield DL, Vingren JL, Fragala MS, Ho J‐Y, et al. (2008) Effects of L‐ carnitine L‐tartrate supplementation on muscle oxygenation responses to resistance exercise 22: 1130‐5.
- Kraemer WJ, Spiering BA, Volek JS, Ratamess NA, Sharman MJ, Rubin MR, et al. (2006) Androgenic responses to resistance exercise: effects of feeding and L‐carnitine 38: 1288‐96.
- Kraemer WJ, Volek JS, Spiering BA, Vingren JLJMfCCM (2005) L‐carnitine supplementation: A new paradigm for its role in exercise 136: 1383‐90.
- Dubelaar M‐L, Lucas CM, Hülsmann WCJJoCS (1991) The Effect of L‐Carnitine on Force Development of the Latissimus Dorsi Muscle in Dogs 6: 270‐5.
- Hülsmann W, Dubelaar MJM (1992) biochemistry c. Carnitine requirement of vascular endothelial and smooth muscle cells in imminent ischemia 116: 125‐9.
- Nüesch R, Rossetto M, Martina BJDue (1999) research c. Plasma and urine carnitine concentrations in well‐ trained athletes at rest and after exercise. Influence of L‐carnitine intake 25: 167‐71.
- Schwane JA, Johnson SR, Vandenakker CB, Armstrong RBJM (1983) sports si, exercise. Delayed‐ onset muscular soreness and plasma CPK and LDH activities after downhill running 15: 51‐6.
- Newham D, McPhail G, Mills K, Edwards RJJotns (1983) Ultrastructural changes after concentric and eccentric contractions of human muscle 61: 109‐22.
- Warren GL, Ingalls CP, Lowe DA, Armstrong RJJoO, Therapy SP (2002) What mechanisms contribute to the strength loss that occurs during and in the recovery from skeletal muscle injury? 32: 58‐64.
- Cruz‐Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. (2010) Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People 39: 412‐ 23.
- McLennan PL, Tapsell LC, Owen A, Gutteridge IJAPJoCN (2003) The influence of red meat intake upon the response to a resistance exercise‐training program in older Australians 12.
- Thomas DK, Quinn MA, Saunders DH, Greig CAJJotAMDA (2016) Protein supplementation does not significantly augment the effects of resistance exercise training in older adults: a systematic review 17: 959. e1‐9.
- Costell M, O'Connor J, Grisolia SJB (1989) communications br. Age‐dependent decrease of carnitine content in muscle of mice and humans 161: 1135‐43
- Malaguarnera M, Cammalleri L, Gargante MP, Vacante M, Colonna V, Motta MJTAjocn (2007) L‐ Carnitine treatment reduces severity of physical and mental fatigue and increases cognitive functions in centenarians: a randomized and controlled clinical trial 86: 1738‐44.
- Pistone G, Marino AD, Leotta C, Dell’Arte S, Finocchiaro G, Malaguarnera MJD, et al. (2003) Levocarnitine administration in elderly subjects with rapid muscle fatigue: effect on body composition, lipid profile and fatigue 20: 761‐7.
- Evans M, Guthrie N, Pezzullo J, Sanli T, Fielding RA, Bellamine AJN, et al. (2017) Efficacy of a novel formulation of L‐Carnitine, creatine, and leucine on lean body mass and functional muscle strength in healthy older adults: a randomized, double‐blind placebo‐controlled study 14: 1‐15.
- Pooyandjoo M, Nouhi M, Shab‐Bidar S, Djafarian K, Olyaeemanesh AJOr (2016) The effect of (L‐) carnitine on weight loss in adults: a systematic review and meta‐analysis of randomized controlled trials 17: 970‐6.
- Owen K, Jit H, Maxwell C, Nelssen J, Goodband R, Tokach M, et al. (2001) Dietary L‐carnitine suppresses mitochondrial branched‐chain keto acid dehydrogenase activity and enhances protein accretion and carcass characteristics of swine 79: 3104‐12.
- Keller J, Ringseis R, Koc A, Lukas I, Kluge H, Eder KJA (2012) Supplementation with l‐carnitine downregulates genes of the ubiquitin proteasome system in the skeletal muscle and liver of piglets 6: 70‐8.
- Parandak K, Arazi H, Khoshkhahesh F, Nakhostin‐ Roohi BJAjosm (2014) The effect of two‐week L‐ carnitine supplementation on exercise‐induced oxidative stress and muscle damage 5: 123.
- Cao Y, Qu H‐j, Li P, Wang C‐b, Wang L‐x, Han Z‐ wJTTjoem (2011) Single dose administration of L‐ carnitine improves antioxidant activities in healthy subjects 224: 209‐ 13.
- Nicassio L, Fracasso F, Sirago G, Musicco C, Picca A, Marzetti E, et al. (2017) Dietary supplementation with acetyl‐ l‐carnitine counteracts age‐related alterations of mitochondrial biogenesis, dynamics and antioxidant defenses in brain of old rats 98: 99‐109.
FIGURE 1
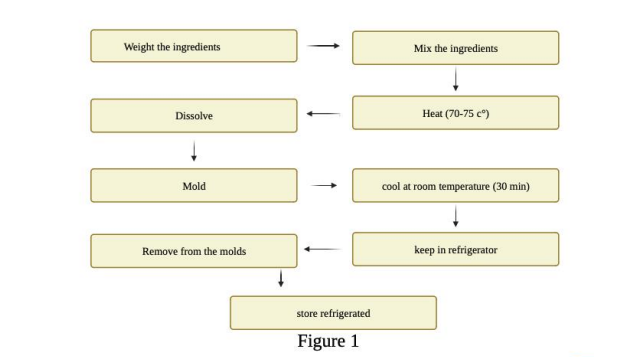
Figure 1: