Varicose Veins: Emerging Herbal Drug Treatments
Received Date: December 28, 2023 Accepted Date: January 28, 2024 Published Date: January 31, 2024
doi: 10.17303/jmph.2024.3.104
Citation: Vanshita Hardiya, Dr. Ranajit Shinde, Dr. Shashikant Bagade (2024) Varicose Veins: Emerging Herbal Drug Treatments. J Med Plant Herbs 1: 1-20
Abstract
Varicose veins, a common condition that distresses a substantial portion of the population world widely. They are twisted, enlarged and swollen veins that can cause discomfort and pain mainly in lower extremities. The purpose of this review is to covers risk factors like age and gender as well as the afflicted population with varicose veins. Varicose veins’ signs and symptoms, as well as the diagnostic procedures used to find the condition. Newer techniques are also covered, including radiofrequency ablation and endovenous laser therapy. Finally, the review explores the use of herbal remedies and vitamins for varicose veins including stone root, gotu kola, and butcher’s broom. Overall, this review provides a comprehensive overview of the current understanding of varicose veins and the various treatment options available.
Keywords: Varicose Vein; Stages; Herbal Treatment; Diagnosis; Newer There pie
Introduction
Varicose VeinVaricose veins are thin walled vessels carry deoxygenated blood, they are also known as varicoses or varicosities, trunk varies varicosities in the line of the long or short saphenous vein or their major branches [1]. Varicose veins occur when veins become enlarged, swollen, and twisted that are usually found in the legs and feet (lower extremities). That usually happens when the valves within the veins that help regulate blood flow become weakened or damaged, causing blood to pool and the veins to stretch and bulge. They may also cause skin changes such as itching, dryness, have a bluish-purple or red colour or discoloration in affected area [2]. In some cases, varicose veins can lead to complications such as blood clots or ulcers. Sometimes mild varicose vein can be cosmetic concern but further it may lead to serious problems [3,4].
Affected PopulationVarious peoples worldwide are affected by varicose vein it is reported 30% and around 10%–15% in males and 20%–25% in females, according to survey it is more common in females2 . Currently, it is reported that globally about 2%–7.3% of the population is affected by varicose veins.1 In the United Kingdom, it is assessed that 33% of the population has varicose veins of the lower legs. It is estimated that up to 25% of adults in the United States have varicose veins. In Europe, the prevalence of varicose veins varies by country but is generally estimated to be between 10-30% of the adult population [5].
Stages of Varicose VeinsStage 1: The appearance of small, thin veins on the legs.
Stage 2: The appearance of larger, twisted veins that are more noticeable.
Stage 3: Swelling and discomfort in the lower extremities, as well as skin changes such as itching or discoloration (bluish-purple or red color).
Stage 4: The development of open sores or ulcers on the skin [6].
Causes and Risk FactorWeak or damaged vein valves: Veins have one-way valves that help blood flow back to the heart. When these valves weaken or become damaged, blood can flow backward and pool in the veins, causing them to swell and bulge
Genetics (heredity): A family history of varicose veins increases the likelihood of developing the condition.
Age: As people get older, the veins in their legs can weaken, making them more susceptible to varicose veins.
Hormonal changes (female hormone): Changes in hormone levels, such as during pregnancy, puberty, or menopause, can cause the veins to enlarge.
Pregnancy: During pregnancy, the volume of blood in the body increases, which can put pressure on the veins in the legs and cause them to enlarge.
Obesity: Excess weight puts pressure on the veins in the legs, increasing the risk of developing varicose veins.
Prolonged standing or sitting or occupation and physical activities: Jobs or activities that require long periods of standing or sitting can put pressure on the veins in the legs and increase the risk of varicose veins.
Prior leg injury: A prior injury to the leg may damage the veins and increase the risk of varicose veins.
Gender: Women are more likely to develop varicose veins than men, possibly due to hormonal changes.
Family history: A family history of varicose veins increases the risk of developing the condition
Smoking and alcohol consumption: Smoking can reduce blood flow and increase the risk of varicose veins [7].
Signs and SymptomsVisible, twisted, or bulging veins: The veins in the legs may appear blue, twisted, or bulging, especially after standing for extended periods.
Aching, heavy, or tired legs: The legs may feel achy, heavy, or tired, especially after standing or sitting for extended periods.
Swelling: The legs and ankles may become swollen, especially after standing for extended periods.
Itching or burning: The skin around the varicose veins may feel itchy or burn, especially if the veins are close to the skin's surface.
Skin changes: The skin around the varicose veins may become discolored, dry, or irritated, especially if the condition is severe.
Cramping or throbbing: Some people with varicose veins may experience cramping or throbbing in their legs, especially at night.
Bleeding: In rare cases, varicose veins may burst and cause bleeding [2].
PathophysiologyThe pathophysiology of varicose veins involves the dysfunction of the venous valves and the subsequent impairment of the venous system's ability to return blood to the heart. The venous system consists of veins that transport blood back to the heart, primarily in the lower extremities. Pathophysiology is divided into mainly four categories that may overlap with one another: increased deep venous pressure (distal, proximal), primary valvular incompetence, secondary valvular incompetence, and fascial weakness [8]. Normally, venous valves, which are one-way valves within the veins, prevent blood from backward flow or refluxing. In people with varicose veins, the venous valves in the legs become weak or damaged, leading to venous reflux. When the venous valves are not working correctly, blood can pool in the veins, leading to an increase in venous pressure, which can cause the veins to stretch and enlarge Varicose veins develop as a result of the weakening and loss of flexibility of the vein walls over time. Blood flow through the veins decreases as they get bigger and more convoluted, which causes greater venous reflux and higher venous pressure. The surrounding tissue may become inflamed (burn) and edematous as a result of the increased pressure, producing symptoms including pain, swelling, and discomfort [8].
Diagnosis
Medical History and Physical ExaminationIt is essential to gather an extensive medical history in order to identify risk factors and potential underlying causes of varicose veins. Examinable information includes past pregnancies, prolonged standing or sitting occupations, family history, blood clots, and venous illnesses.
During a physical examination, a doctor pays close attention to the veins' characteristics and appearance. The veins' texture, position, colour, and size are all examined, as well as any accompanying symptoms like discomfort, swelling, or skin changes [9].
Doppler UltrasoundDoppler ultrasound is a type of ultrasound imaging that measures blood flow in veins and arteries using sound waves. A transducer, a portable instrument, is applied to the skin over the area being studied during a Doppler ultrasound. High-frequency sound waves from the transducer cause echoes when they hit the blood cells. The transducer then detects the echoes and transforms them into visible or audible signals that a healthcare professional can understand.
Doppler ultrasound can be used to determine the direction and rate of blood flow in veins, as well as to identify any obstructions or irregularities. Doppler ultrasound can detect venous reflux, or the backward flow of blood in veins caused by faulty valves.
The non-invasive, painless, and safe Doppler ultrasonography procedure requires no downtime or preparation. Duplex ultrasound, on the other hand, combines conventional ultrasound imaging with Doppler ultrasound. It allows medical experts to evaluate the internal structure and blood flow of the veins. Duplex ultrasonography can detect and monitor venous reflux as well as evaluate the internal organisation of veins [9,10].
Venogram:A venogram is a diagnostic imaging procedure used to examine the veins of the body, particularly the deep veins. It is widely used to diagnose conditions such as deep vein thrombosis (DVT) and venous insufficiency, and it provides accurate information on the vein structure and function [9,10].
Treatment of Varicose Veins [9,11]Lifestyle modification or changes: Regular exercise, maintaining a healthy weight, avoiding extended sitting or standing, and wearing compression stockings can help ease symptoms and prevent varicose veins from worsening.
Vein stripping: This is a surgical procedure in which the affected veins are removed through small incisions in the skin.
Sclerotherapy: Sclerotherapy is a minimally invasive procedure that involves injecting a solution directly into the problematic veins, causing them to shrink and seal. After that, blood flow is rerouted to healthier veins.
Ambulatory phlebectomy: This is a minimally invasive surgical procedure in which small incisions are made in the skin to remove the affected veins.
Radiofrequency ablation: A minimally invasive procedure that uses heat to shut the damaged veins. After that, blood flow is rerouted to healthier veins.
EVLT: Endovenous laser therapy is a minimally invasive surgery that uses a laser to heat and seal the afflicted veins. After that, blood flow is rerouted to healthier veins.
Newer Therapies for Treatment of Varicose VeinCyanoacrylate glue ablation: During this minimally invasive procedure, the troublesome veins are injected with a medical adhesive, causing them to close. This procedure is less invasive than traditional vein stripping surgery and can be performed under local anaesthesias [12,13].
Clarivein: A specialised catheter is used in this treatment to deliver a mix of mechanical and chemical therapy to seal the troubled veins [14].
Varithena: this is foam sclerotherapy procedure, the problematic veins are sealed off using a unique foam solution. It is a minimally invasive procedure that can be carried out under local anaesthesia at a doctor's office [15].
Chiva: The term is a French acronym stands for Conservatrice Hémodynamique de l'Insuffisance Veineuse en Ambulatoire (ambulatory conservative hemodynamic treatment venous insufficiency). Doppler ultrasonography is used in Chiva to evaluate the hemodynamics. To be more precise, the ultrasound scan is used to determine where in the venous system the reflux first occurs. The Chiva method, which is based on the hemodynamics of the venous system, strives to maintain the body's venous system while redressing imbalances brought on by shunts between the deep and superficial venous systems. The main characteristics of the procedure are [16]:
Use of local anesthesia
day-clinic surgery (not required hospitalization)
person can immediate return to activities
low pain scores procedure
avoidance of removal of collaterals causing fewer marks on skin [16,17].
he Endovenous ASVAL (Arterialization and Spontaneous Vascular Anastomosis of the Ligation)This procedure is a minimally invasive surgical technique for the treatment of varicose veins. This technique involves inserting a radiofrequency catheter or laser fibre into the afflicted vein using a specialised tool. The vein then collapses and seals shut as a result of the device's heating of the vein interior. After that, blood is redirected to the leg's stronger veins, improving blood flow and reducing pain and swelling. The ASVAL method for treating varicose veins is often done as an outpatient procedure and doesn't require general anaesthesia, making it a rather safe and practical choice. The ASVAL approach does, however, carry certain possible hazards and side effects, such as bleeding, infection, nerve damage, and bruising, as with any medical operation [18].
Vitamins useful in Varicose veinsVitamin E is a powerful antioxidant that can protect the cardiovascular system from the destructive effects of free radicals. Vitamin E also has anti-inflammatory properties that may help prevent and control varicose veins by reducing inflammation in vein linings [19]. Vitamin E also thins the blood by preventing platelets from adhering together. In one clinical study, supplementation of 600 IU of vitamin E per day reduced the occurrence of venous thrombosis, or vein clot formation, in women. Study suggested that vitamin E may help prevent blood clots in the legs by reducing the blood clotting effects of vitamin K while maintaining normal clotting activity. Almonds, sunflower seeds, avocado and fortified cereals are all great sources of vitamin E [20].Vitamin C also works effectively in conjunction with vitamin E to maintain the veins healthy. One study on smokers discovered that 2,000 mg of vitamin C with 400 IU of vitamin E improved endothelial function and decreased levels of clotting factors in the blood [21]. Vitamin C contains antioxidant and anti-inflammatory effects. Ascorbate prevents endothelial dysfunction, boosts type IV collagen formation, and increases cell proliferation in endothelial cells. In sites of vascular injury, ascorbate suppresses dedifferentiation, recruitment, and proliferation of vascular smooth muscle cells [22]. Vitamin B3, also known as niacinamide, prevents and reduces inflammation of endothelial cells, which form the inner linings of veins. It also improves the function of nitric oxide, a compound that relaxes blood vessels and promotes healthy circulation [23]. Homocysteine is linked to blood vessel inflammation, atherosclerosis, and poor platelet function. However, vitamins B6, B12, and vitamin B9 lower homocysteine levels, reducing formation of blood clots in the legs [24].
Vitamin K plays role in the calcification of varicose veins as well as a role in the proliferation of smooth muscle cells in the media layer of the vein wall [25,26]. It has been hypothesized that, formation of varicoceles, leading to varicose veins results in poor prostate health is essentially a vitamin K insufficiency disorder [27]. Increase in intake of vitamin K, both as vitamin K1 (phylloquinone) and vitamin K2 (menaquinone) will lessen arterial calcification and improve prostate function.
Herbs useful in Varicose VeinsMany herbs have specific compositions or ingredients that have ability to reduce inflammation and help to improve blood flow by vasocontraction and vasodilation actions [28]. Some of them are used in external applications such as in poultices, sitz baths, oils, suppositories or fomentation form e.g. Butcher’s broom, Saint John’s wort, Calendula, Ruta, Arnica, Comfrey, Slippery elm, Plantain. Many of them are being used internally e.g. Cinnamon, Gotu kola, Witch hazel, Geranium, Oak bark, Yarrow, Saint John ‘s wort, Calendula, Horse chestnut, Liver herbs, Cayenne, Garlic, Onion, Ginger [28]. These are discussed below [29-31].
STONE ROOT: Stone root -Richweed, (collinsonia canadensis)
Family: Lamiaceae or Mint family
Part used: The root and rhizome (underground stem) are used to make medicine.
Benefits: It used as vaso-contracting agent to the portal system so is indicated for pelvic/rectal congestion secondary to portal back-pressure and venous stasis [28,32].
Stone root (Collinsonia canadensis) has been traditionally used for various medicinal purposes, including the treatment of venous insufficiency and varicose veins. It is believed that the plant's active constituents, including flavonoids, tannins, and resins, help to strengthen and tone the walls of the veins and improve blood circulation. One particular constituent found in stone root that is believed to be responsible for its beneficial effects on varicose veins is a compound called rutin. Rutin is a flavonoid and it have antioxidant and anti-inflammatory properties, and it can reduce inflammation and improve blood circulation in the veins [33,34].
BUTCHER‘S BROOM: Ruscus aculeatus
Family: Liliaceae (Lily family).
Part used: leaves and rhizome of the plant.
Benefits: It has anti-inflammatory, antihemorragic, and vasoconstrictive properties. When applied externally, it causes venous constriction and decreases inflammation [35].
Butcher's broom (Ruscus aculeatus) has been traditionally used for various therapeutic purposes, including the treatment of venous insufficiency and varicose veins. The active components of the plant, such as flavonoids, saponins, and steroidal glycosides, are thought to strengthen and tone vein walls and enhance blood circulation. Butcher's broom contains a specific ingredient known as ruscogenin, which is thought to be responsible for of the herb's therapeutic benefits on varicose veins. Ruscogenin, a steroidal saponin with anti-inflammatory and vasoconstrictive effects, is thought to aid in reducing inflammation and enhancing venous blood flow. Other substances found in butcher's broom, like flavonoids and tannins, may also contribute to the herb's positive benefits on varicose veins. These substances have antioxidant and anti-inflammatory characteristics [35].
CINNAMON: Cinnamomum verum
Family: Lauraceae or laurel family.
Part used: inner bark.
Benefits: Cinnamon has the capacity to improve circulation and raise blood flow. Cinnamon may specifically aid in blood artery dilating and widening, facilitating improved blood flow throughout the body.
Cinnamon (Cinnamomum verum) is a common spice used in cooking and therapeutic purpose. Several bioactive substances found in cinnamon, such as cinnamaldehyde, cinnamic acid, and cinnamate, are thought to have anti-inflammatory, antioxidant, and antiplatelet properties. These substances may aid in enhancing blood flow and reducing inflammation, which may be advantageous for people who suffer from varicose or venous insufficiency. Cinnamon has also been demonstrated to have favourable effects on blood sugar levels, which may be helpful for people with circulation issues.Cinnamon has the ability to improve circulation and raise blood flow. Cinnamon may specifically aid in blood artery dilating and widening, facilitating improved blood flow throughout the body [36].
GOTU KOLA: Centella asiatica
Family: Umbelliferae or apiaceae family.
Part used: whole plant.
Benefits: Gotu kola can be used externally and internally. It accelerates the healing time in wounds and ulcers, and also act as circulatory stimulant.
Gotu kola (Centella asiatica) is a traditional herbal remedy that has been used for various therapeutic purposes, including the treatment of venous insufficiency and varicose veins. Triterpenoids, flavonoids, and asiaticoside are the active ingredients in gotu kola that are thought to be in charge of the herb's therapeutic actions on venous insufficiency. Triterpenoids, such as asiaticoside, are thought to enhance circulation by strengthening vein walls and lowering inflammation. Additionally, they have antioxidant qualities which may shield the veins from oxidative stress brought on by free radicals. In addition to having antioxidant and anti- inflammatory characteristics, gotu kola contains flavonoids including quercetin and kaempferol that may help treat varicose veins and venous insufficiency. Other substances found in gotu kola, including beta-carotene, tocopherol, and zinc, are also thought to assist good circulation and enhance vein health [37].
GARLIC: Allium sativum
Family: Amaryllidaceae or amaryllis family.
Part used: leaves, flower, and cloves.
Benefits: Garlic has fibrinolytic properties that reduce the likelihood of thrombus development in thrombophlebitis and the fat deposition caused by varicose veins that can result in lumpy skin. By effectively breaking down proteins, it improves protein supply by regulating and properly distributing proteins.
Garlic (Allium sativum) is a commonly used culinary ingredient and traditional medicinal herb that is believed to have many benefits. Allicin, one of garlic's active ingredients, is thought to have antioxidant and anti-inflammatory qualities in addition to being the source of the herb's distinctive odour. Individuals with venous insufficiency or varicose veins may benefit from these qualities since they can reduce vein irritation and enhance blood flow.
Other substances found in garlic, including flavonoids and organosulfur compounds, are also thought to have positive benefits on cardiovascular health. While organosulfur compounds are thought to help lower cholesterol levels and enhance blood flow, flavonoids have anti- inflammatory and antioxidant characteristics that may help protect the veins from damage caused by free radicals. Garlic has also been demonstrated to have anticoagulant qualities, which may aid in preventing blood clots and enhancing venous blood flow [38].
CAYENNE PEPPER: Capsicum annuum
Family: Solanaceae or deadly nightshade
Part used: Seeds and fruits of plant is used.
Benefits: Varicose vein cause fat deposition it may result lumpy skin, cayenne act as fibrinolytic agent and decrease the risk of thrombus formation in thrombophlebitis.
Cayenne pepper (Capsicum annuum) is commonly used as a culinary spice and traditional medicinal herb. cayenne is believed to have properties that may be beneficial for blood circulation and vein health. Cayenne pepper's primary ingredient, capsaicin, is thought to have antioxidant and anti-inflammatory qualities in addition to giving the spice its distinctive heat. People who suffer from venous insufficiency or varicose veins may find that capsaicin improves blood flow and reduces vein inflammation.
Capsaicin can be given topically in the form of creams or ointments to assist relieve discomfort brought on by varicose veins. It is also thought to have a pain-relieving effect. Other substances found in cayenne pepper, including flavonoids and carotenoids, are also thought to have advantageous effects on cardiovascular health. Carotenoids are thought to maintain healthy circulation and enhance vein health, while flavonoids are thought to have antioxidant and anti- inflammatory qualities that may help protect the veins from damage caused by free radicals [30,39].
GINGER: Zingiber officinale
Family: Zingiberaceae or ginger family.
Part used: Rhizome, ginger root or whole ginger are used.
Benefits: varicose vein cause fat deposition it may result lumpy skin, ginger act as fibrinolytics and decrease the risk of thrombus formation in thrombophlebitis. ginger also help in regulation and proper distribution of proteins and it enhance protein supply by effective break down of proteins
Ginger (Zingiber officinale) is popular culinary ingredient and herbal remedy that has been used for centuries for therapeutic purposes. Gingerol, which gives ginger its distinctive flavour and is thought to have antioxidant and anti-inflammatory qualities, is one of the active ingredients in ginger. People with venous insufficiency or varicose veins may find these qualities helpful in reducing vein irritation and improving blood flow
Other substances found in ginger, like flavonoids and terpenoids, are also thought to have positive benefits on cardiovascular health. Terpenoids are thought to aid in improving circulation and reducing edoema, while flavonoids contain anti-inflammatory and antioxidant characteristics that may help protect the veins from harm brought on by free radicals. In addition, ginger has been demonstrated to have anticoagulant qualities, which may aid in preventing blood clots and enhancing venous blood flow [40].
WITCH HAZEL: Hamamelis virginiana Family: Hamamelidaceae or witch hazel family. Part used: Bark is used.
Benefits: Used in venous laxity (Ligamentous laxity) and also used as an astringent, styptic, for wounds and local inflammations.
Witch hazel (Hamamelis virginiana) is a traditional herb that isbelieved to have astringent, anti- inflammatory, and antioxidant properties. Witch hazel contains tannins, flavonoids, and other polyphenols, which are thought to be the active ingredients responsible for its therapeutic properties. Tannins contain astringent qualities that aid in vein tightening and toning, lowering edoema, and enhancing blood flow. Flavonoids contain anti-inflammatory and antioxidant property that may help prevent free radicals from harming veins and lessen vein inflammation. Witch hazel is frequently applied topically in the form of lotions, ointments, or astringents to help relieve the swelling, itching, and discomfort associated with varicose veins. Over time, it may also help decrease the visibility of varicose veins [30].
GERANIUM: Pelargonium graveolens Family: Geraniaceae or geranium family. Part used: roots.
Benefits: It used as astringent, (stypic), and act as tonifying for (atomic tissue) venous atony.
Geranium (Pelargonium graveolens) is a plant that is commonly used in traditional medical purpose and aromatherapy. Geraniol, citronellol, and linalool are the major chemical components of geranium oil that are responsible for its distinctive aroma and potential medicinal effects. Antioxidant and anti-inflammatory effects of geraniol have been demonstrated, which could help in reducing vein inflammation and enhancing blood flow. The antispasmodic effects of citronellol are thought to help veins relax and decrease the visibility of varicose veins. Furthermore, it's thought that geranium oil has astringent characteristics that can help to tighten and tone the veins, lowering swelling and enhancing blood flow [41].
OAK BARK (White oak) White oak: Quercus alba
Family: belongs to the Fagaceae or beech family
Part used: bark is used.
Benefits: It has astringent property, and it is useful in treatment of venous laxity and congestion, such as bleeding hemorrhoids and other varicosities. Oak bark has been used for various treatment, including varicose veins. It is thought to have astringent, anti-inflammatory, and antioxidant qualities. The therapeutic properties of oak bark are thought to be a result of its active ingredients, which include tannins, flavonoids, and other polyphenols. Tannins contain astringent properties that relief in vein tightening and toning, lowering edoema, and enhancing blood flow. It is also help in ulcer relief by treating membrane irritation. Flavonoids contain anti-inflammatory and antioxidant qualities that may help prevent free radicals from harming veins and decrease vein inflammation.
Oak bark can apply topically (astringent and styptic) in the form of creams, ointments, or astringents to help relieve the swelling and discomfort associated with varicose veins [30].
YARROW: Achillea millefolium Family: Asteraceae or daisy family. Part used: Flowers and leaves.
Benefits: It is bitter tonic, antiseptic, styptic, anti-inflammatory and anodyne. It is used for atonic and relaxed tissues where there is free discharge or massive bleeding of bright red blood 28occurs.
The medicinal plant yarrow (Achillea millefolium) has been used for millennia to cure a number of illnesses, including varicose veins. It is thought to have astringent, anti-inflammatory, and antioxidant effects that could help reduce the signs and symptoms of varicose veins and improve vein health. Flavonoids, tannins, and volatile oils are some of yarrow's active ingredients, and these are thought to be what gives the herb its therapeutic properties. Flavonoids contain anti- inflammatory and antioxidant properties that may help prevent free radicals from harming veins and reduce vein inflammation. Tannins contain astringent qualities which help in vein tightening and toning, lowering edoema, and enhancing blood flow. Varicose vein pain and discomfort may be lessened by the anti-inflammatory and calming effects of volatile oils, such as chamazulene and bisabolol.
Yarrow is frequently applied topically to treat varicose vein symptoms like pain, edoema, and irritation. It can be found in creams, lotions, and compresses. Additionally, it is said to gradually decrease the visibility of varicose veins [42].
SAINT JOHN‘S WORT: Hypericum perforatum
Family: Guttiferae or clusiaceae family.
Parts used: flowering tops (when they are a mix of buds and open flowers).
Benefits: Saint John's Wort (Hypericum perforatum) is a medicinal herb has historically been used to treat a variety of illnesses, including varicose veins. Saint John's Wort is thought to contain anti-inflammatory and antioxidant characteristics, which may help reduce the symptoms of varicose veins and enhance vein health, while there is little evidence on its efficacy for this particular condition.
Hypericin, hyperforin, and flavonoids are some of Saint John's Wort's active ingredients, and these are thought to be what gives the herb its medicinal properties. The anti-inflammatory and antioxidant characteristics of hypericin and hyperforin are thought to help reduce inflammation in the veins and protect them from damage brought on by free radicals. Due to their antioxidant characteristics, flavonoids may also aid in preventing vein damage and enhancing vein health.
saint John's Wort is used topically to treat varicose vein symptoms like pain, edoema, and discomfort. It comes in cream or oil form. To maintain general vein health, it can also be consumed orally as a supplement [43].
CALENDULA : Calendula officinalis
Family: Asteraceae
Part used: Flowers prior to fully opens is used.
Benefits: Act as antiseptic, anti-inflammatory, it also supports creation of normal connective tissue structure and wound healing44.
The medicinal herb calendula (Calendula officinalis) has been used for centuries to cure a number of illnesses, including varicose veins. It is thought to have astringent, anti-inflammatory, and antioxidant effects that could help reduce the signs and symptoms of varicose veins and improve vein health. Flavonoids, triterpenoids, carotenoids, and volatile oils are some of the calendula's active ingredients and are thought to be the source of its therapeutic properties.
Flavonoids contain anti-inflammatory and antioxidant properties that may help prevent free radicals from harming veins and lessen vein inflammation. Triterpenoids contain astringent qualities which help in vein tightening and toning, lowering edoema, and enhancing blood flow. Carotenoids with antioxidant qualities, such as beta-carotene and lutein, may aid in preventing vein damage and enhancing vein health. Due to their anti-inflammatory and antiseptic qualities, volatile oils like thymol and carvacrol may be able to reduce the pain and discomfort linked to varicose veins as well as prevent infections. Calendula is frequently applied topically to treat varicose vein symptoms like swelling, pain, and discomfort [45,46].
HORSE CHESTNUT: Aesculus hippocastanum
Family: Sapindaceae or soapberry family.
Part used: Ripe chestnut and bark.
Benefits: It act as astringent and improves vascular resistance, reduces pathologically induced capillary wall permeability [28,47].
Horse chestnut (Aesculus hippocastanum) contain active substances known as aescin (also known as escin), flavonoids, and saponins, which are thought to be the cause of its therapeutic properties. Horse chestnut seeds' main active ingredient, aescin, is thought to have venotonic, anti- inflammatory, and antiedematous effects that could help increase blood flow, lessen swelling, and treat the signs and symptoms of varicose veins. Due to their antioxidant qualities, flavonoids like quercetin and kaempferol may be able to protect veins from oxidative damage and enhance vein health. Aescin is one saponin that has astringent qualities that aid to tighten and tone the veins, which decreases edoema and improves blood flow.
Horse chestnut is frequently applied topically in the form of lotions, gels, or ointments to assist relieve the swelling, pain, and discomfort associated with varicose veins. To increase blood flow and lower the risk of developing new varicose veins, it is also taken orally in the form of supplements, capsules, or tablets. Saponins (aescin) have astringent characteristics that help to tighten and tone the veins, reducing edoema and enhancing blood flow48,49
AGRIMONY: Agrimonia eupatoria
Family: Rosaceae or rose family.
Part used: Aerial parts.
Benefits: The medicinal plant agrimony has long been used to cure a variety of illnesses, including varicose veins. The plant's tannins and flavonoids are thought to be the cause of any potential advantages. Many plants, including agrimony, contain tannins, a kind of polyphenol. As a result of their well-known astringent characteristics, they can aid in tightening and toning the vein walls, thereby lowering edoema and inflammation. Flavonoids, which include quercetin and rutin, are antioxidants that can enhance circulation, lower the risk of blood clots, and protect veins from oxidative damage. Varicose vein symptoms like swelling, discomfort, and inflammation are frequently treated topically with agrimony in the form of lotions, ointments, or poultices. To enhance vein health and circulation, it is also taken orally in the form of teas, tinctures, or capsules [30].
SLIPPERY ELM: Ulmus rubra
Family: Ulmaceae or elm family.
Part used: Inner bark.
Benefits: Used internally as anti-inflammatory. And used externally for wounds, burns, ulcers, and all skin disorders with inflammation [28].Slippery elm (Ulmus rubra) is a medicinal plant that has been used to treat a variety of health conditions, including varicose veins. The plant's mucilage content might be the cause of its possible advantages. The soluble fibre known as mucilage is present in a wide variety of plants, including slippery elm. It can help calm and preserve the vein lining by combining with water to create a gel-like material. Inflammation and irritation, two frequent varicose vein symptoms, can be reduced by doing this. The promotion of blood flow through the veins is another way that slippery elm may aid in enhancing circulation. Slippery elm is frequently applied topically in the form of lotions, ointments, or poultices to assist relieve the swelling, pain, and inflammation associated with varicose veins. To enhance vein health and circulation, it is also taken orally in the form of teas, tinctures, or capsules [30,50].
COMFREY : Symphytum officinalis
Family: Boraginaceae
Part used: Root and main rib of leaves.
Benefits: It used externally in form of paste or fomentation for wounds, burns, ulcers and in inflammatory skin disorders and also used in inflammation of thrombophlebitis and phlebitis. It decreases the healing time for skin wounds and irritations.
Since ancient times, the herb comfrey (Symphytum officinale) has been used to treat a number of medical ailments, including varicose veins. Allantoin, rosmarinic acid, and tannins are primarily responsible for its possible medicinal effects. Chemically speaking, allantoin is an anti- inflammatory substance that is also known to accelerate the healing of wounds. It can aid in reducing varicose veins' characteristic symptoms of inflammation and irritation in the veins. The anti-inflammatory properties of rosmarinic acid are another benefit, and it may help shield the veins from oxidative stress. An astringent form of polyphenol known as tannins can aid to lessen edoema and inflammation.
Comfrey is often used externally to reduce swelling, pain, and inflammation caused by varicose veins. It can also be used in lotions, ointments, and poultices. To enhance vein health and circulation, it is also administered orally as teas or capsules [30].
RED ROOT: Ceanothus americanus
Family: Rhamnaceae or buckthorn family. Part used: Root
Benefits: It is beneficial for liver problem. It supports the liver and decrease blockage in the flow of blood from the rectal to the portal veins [28]. It also acts as astringent.
Red root (Ceanothus americanus) is a plant that is commonly used for its therapeutic purpose. Its major component, a flavonoid known as quercetin. Quercetin is antioxidant that has antiinflammatory and antiplatelet properties. It aids in lowering vein swelling and irritation, which are frequent signs and symptoms of varicose veins. It also helps to improve blood circulation by preventing clots from forming in the veins.
Red root is frequently applied topically in the form of creams or ointments to aid with the swelling, discomfort, and inflammation associated with varicose veins. To enhance vein health and circulation, it can also be consumed orally as tea or pills [30].
LICORICE: Glycyrrhiza glabra Family: Fabaceae or Leguminosae family. Part used: Roots.
Benefits: It act as anti-inflammatory agent, licorice decrease inflammation by enhancing movement of leucocytes towards inflamed areas [28].
One of the active chemicals in licorice (Glycyrrhiza glabra) is glycyrrhizin, which has anti- inflammatory and antioxidant properties that may help to increase blood flow and reduce vein swelling. Flavonoids, another substance included in licorice, have been found to have venotonic qualities, which means that they can strengthen and tone the veins, increasing their elasticity and lowering the risk of blood pooling and inflammation.
licorice also includes coumarin, a substance with anticoagulant qualities that can lessen the risk of varicose vein issues by preventing blood clots from developing in the veins [51]
TURMERIC: Curcuma longa Family: Zingiberaceae or ginger family. Part used: Rhizomes.
Benefits: Act as anti-inflammatory, anticoagulant (inhibits platelet aggregation) and increase wound healing.
Turmeric's active component, curcumin, is the component that gives it its possible medical benefits. Anti-inflammatory and antioxidant effects of curcumin have been demonstrated; these features may aid in reducing inflammation and enhancing venous blood flow. Additionally, it can lessen the likelihood of blood clotting by strengthening the walls of the veins [52].Turmeric also includes other substances, such as turmerone, atlantone, and zingiberene, which have been proven to have anti-inflammatory and antioxidant effects and may be useful for treating varicose ve [53].
HAZEL : Hamamelis virginiana Family: Betulaceae or birch family. Parts used: Fruits.
Benefits: It have venotonic action which is used on varicose veins and edema caused by venous insufficiency [28].
Tannins and flavonoids are the active components of hazel that give it its potential therapeutic benefits.
Tannins are a type of polyphenol and has astringent characteristics, which means that it can assist to tighten and constrict the walls of blood vessels, hence reducing vein size and enhancing blood flow. This may help in lowering vein swelling and inflammation, enhancing their appearance, and alleviating pain. Another class of substances that can be found in hazel and have anti-inflammatory and antioxidant activities are flavonoids. They have been demonstrated to decrease the possibility of blood clotting and inflammation by strengthening and protecting the vein walls.
Topical preparations, including lotions or ointments that can be administered directly to the afflicted area. These topical treatments are thought to aid in circulation improvement, edoema and inflammation reduction, and varicose vein improvement [29].
Raw Potatoes Grated(Solanum tuberosum)
Family: Solanaceae or deadly nightshade family.
Parts used: Fruit pulp.
Benefits: Paste is use on varicose veins legs (affected area).
Raw potatoes do contain some nutrients that may be beneficial for overall health, such as vitamin C, potassium, and fiber [30].
Raw Grated Apples (Malus pumila)
Family: Rosaceae or rose family.
Parts used: Fruit pulp.
Benefits: Apple cider vinegar is used in treatment of varicose veins.30
Apples are a nutritious fruit and contain vitamins, minerals, and fiber that are beneficial for overall health
BRAHMI (Bacopa monniera)
Family: Plantaginaceae or plantain family.
Part used: Leaves and stems.
Benefits: Brahmi contain vitamin (beta carotene), and various proteins which help to improve blood circulation by stimulating cell growth and by building collagen.
Ayurvedic practitioners frequently employ the herb brahmi (Bacopa monnieri) for its possible medical benefits, including its capacity to enhance blood flow and fortify blood vessels. Bacosides and saponins are two of Brahmi's active ingredients that may be the cause of its possible effects.
Brahmi contains a class of substances known as bacosides, which have been proven to have neuroprotective and antioxidant properties. Additionally, they might be advantageous for enhancing blood circulation and lowering vein irritation.
Another class of substances in brahmi known to have anti-inflammatory and antioxidant activities are saponins. It improves circulation and reduces the visibility of varicose veins by strengthening the vein walls and lowering the risk of blood pooling [54].
Pine Bark (Pinus)
Family: Pinaceae family.
Part used: bark used.
Benefits: Pine bark extract contains several active ingredients, including procyanidins, flavonoids, and phenolic acids, that are believed to be responsible for its health benefits.Procyanidins and flavonoids, which are thought to be responsible for its health advantages, including the potential treatment of varicose veins, are found in standardised amounts in Pycnogenol,(branded pine bark extract) [54].
Benefits include: Pycnogenol has been demonstrated to increase nitric oxide synthesis, which helps to relax blood vessels and boost circulation, therefore improving blood flow.
Pycnogenol contains potent anti-inflammatory and antioxidant characteristics that may help reduce swelling and inflammation related to varicose veins. This might assist with symptoms like pain, discomfort, and heavy legs. Pycnogenol has been demonstrated to strengthen blood vessel walls, which may help lower the chance of developing varicose veins and enhance the function of already-existing ones.
Pycnogenol is a potent antioxidant that can aid in protecting against oxidative stress, a condition that can harm cells and tissues and lead to the development of varicose veins [55].
Conclusion
In conclusion, varicose veins are a widespread disease that can significantly lower a person's quality of life. In addition to surgical procedures and compression stockings, more recent therapies including radiofrequency ablation and endovenous laser treatment have the potential to improve patient results. Additionally, the use of herbal treatments for varicose veins has become more widespread as a result of studies showing that some herbs may be useful in easing symptoms. In order to enhance patient outcomes and general quality of life, it is crucial to keep looking into novel treatments for this widespread disease as more research is undertaken.
Sources of L-carnitineSkeletal and cardiac muscle contains almost 90% of the entire carnitine pool; the remaining portion is found in the liver, kidneys, and other tissues. L-carnitine concentrations in skeletal muscles, which serve as the primary reservoir, are at least 50–200 times greater than those in the plasma.The typical concentration in blood ranges from around 41 μM/L in females to 50 μM/L in males. The body needs 15 mg of L-carnitine each day, which is obtained from external sources and endogenous production. Therefore, a modest rate of inner carnitine synthesis, food consumption, and effective renal control of carnitine all contribute to the maintenance of carnitine homeostasis. An adult human organism weighing around 70 kg is normally capable of synthesis of 11–34 mg of L-carnitine daily (160–480 g/kg body weight). However, in terms of stress and physical strain, this quantity may not be adequate, particularly for athletes or sportsmen who have undergone advanced training. Since severe vegetarians do not consume any vegetable protein, they are also likely to be low in L- carnitine, which is mostly found in meats and dairy products. Subnormal blood levels of L- carnitine are also linked to other rare situations involving preterm infants, hemodialysis patients, hereditary abnormalities, or certain chronic conditions. Understanding the amounts of L-carnitine found in various biological components is beneficial when people need exogenous supplementation due to carnitine deficiency. The majority of people take more carnitine than is necessary for apparent maintenance. In humans who are omnivores, a well- designed diet meets around 75% of the daily requirement for carnitine, with only 25% coming from endogenous synthesis. Red meat, especially lamb and cattle, is the main source of L-carnitine. Fish, pork, and chicken, as well as dairy products such as whole milk and cottage cheese, have lesser levels of the amino acid. Products made from plants typically do not have enough carnitine [3,4].
Biosynthesis of L-carnitineHumans can produce L-carnitine through a multi- -step process involving multiple cell compartments using the amino acids lysine and methionine. S-adenosyl-methionine, which is produced from methionine, is the methyl donor in a reaction catalyzed by lysine methyltransferases that methylate protein-bound lysine to form ε-N-trimethyl lysine in various organs. Protein hydrolysis releases ε-NTrimethyl lysine to produce carnitine. The manufacture of endogenous L-carnitine involves four enzymes. All of them are common, except for γ-butyrobetaine hydroxylase, which is not present in skeletal or cardiac muscle.
Nonetheless, the human kidney, testes, and liver all have high levels of expression for this enzyme [5,6].
Since cardiac and skeletal muscles cannot produce L-carnitine on their own, they must receive it from the bloodstream. L-carnitine is mostly produced in the liver and is needed for the oxidation of fatty acids in these muscles. The rate of protein turnover and the degree of methylation of peptide-linked lysine determine the rate of L-carnitine production. Although increases in dietary carnitine intake level or renal reabsorption may boost endogenous Lcarnitine production, excess lysine in the diet may not [7].
Therapeutic use of L-carnitineTreatment with carnitine has been recommended for a wide range of hereditary and acquired illnesses. It can be used to remove harmful metabolites even in cases when plasma and tissue carnitine concentrations are normal, as well as to restore low concentrations in situations linked to deficient states. There are formulations for intravenous and oral use. Even so, there have been few controlled studies and mainly anecdotal accounts of L-carnitine's effectiveness due to the rarity of the majority of the specific illnesses for which it is used. Fortunately, side effects from using L-carnitine are rare and usually mild. Large oral doses can sometimes result in unpleasant fishy smells and diarrhea, although these side effects can typically be avoided by reducing the dosage.
Degradation of L-carnitineEnterobacteria are involved in the conversion of L-carnitine in the gastrointestinal tract when it is taken orally. Pharmacological dosages of carnitine were used in animal research to first show how carnitine breaks down. It has also been seen in humans in circumstances where they consume a typical diet. For aerobic development, L-carnitine can be utilized as a source of both carbon and nitrogen, or it can be employed to preferentially exploit the carbon chain after trimethylamine is broken down. Certain bacteria use carnitine as an electron acceptor through crotonobetaine when they are anaerobic and lack preferred substrates. It has been shown in rats and humans that enteric bacteria can formtrimethylamine and butyrobetaine from L-carnitine (by reducing crotonobetaine). Microbial carnitine dissimilation results in the following end products: trimethylamine in Serratia marcescens, Acinetobacter calcoaceticus, and Pseudomonas putida; glycine betaine in Pseudomonas putida; -butyrobetaine in Escherichia coli, Citrobacter freundii, and multiple Salmonella species; and carbon dioxide and water in Acetinobacter calcoaceticus and Pseudomonad putida [8,9].
L-Carnitine DeficiencyTransfer of long chain fatty acids to the mitochondrial matrix for oxidation requires carnitine. Fatty acids become the main substrate for energy production during fasting times, when they are oxidized in the liver, heart muscle, and skeletal muscle. 60% of muscle oxygen use during extended aerobic exercise is accounted for by fatty acid oxidation. Instead of using fatty acids directly for oxidative metabolism, the brain oxidizes ketones made from acetyl CoA and acetoacetyl CoA, which are produced by the liver's fatty acid oxidation. Deficiency is brought on by an inadequate amount of carnitine in the blood, and this can contribute to a variety of hereditary and acquired illnesses.(9) An autosomal recessive fatty acid oxidation condition resulting from impaired carnitine transport is primary carnitine deficiency. This illness manifests itself either early in childhood as hypoketotic hypoglycemia, which is caused by depletion of glucose reserves an alternate substrate to fatty acids or later in life as cardiomyopathy or skeletal myopathy [9].
There are two main forms of carnitine deficiency that have been identified: myopathic (MCD) and systemic (SCD). Low levels of carnitine in plasma and specific tissues, along with lipid deposit deposition and renal carnitine leakage, are the hallmarks of sickle cell disease (SCD). This particular condition is becoming recognized as a potential cause of very low birth weight or even sudden infant death syndrome. It is characterized by progressive cardiomyopathy and skeletal muscle failure, where fatty acids comprise a basic energy source. Particularly preterm babies have little fat reserves and frequently need their parents' prolonged nourishment, which includes emulsified lipids to provide growth-promoting calories and vital fatty acids. Lipid buildup in the muscles and mild to severe muscular weakness are characteristics of MCD. Although the concentration of carnitine in skeletal muscle is low, the levels of carnitine in plasma and liver are normal.
Secondary causes of low levels of L-carnitine in the diet include dialysis therapy, diabetes, mitochondrial myopathy, inborn errors of metabolism, specifically metabolic defects in fatty acid oxidation, and inadequate absorption from the gastrointestinal tract. Vegetarians may experience a carnitine shortage due to an inadequate food intake. Furthermore, despite the presence of substrate amino acids in parenteral nutrition fluids, prior research has demonstrated that newborns receiving carnitine-free parenteral nutrition are unable to synthesize enough carnitine to maintain plasma concentrations equivalent to those found in healthy newborn infants or older children. Low plasma free carnitine levels and high total carnitine levels are also possible in patients with alcoholism and ketosis, primarily as a result of elevated.
Effect of L-Carnitine in Fatty Acid MetabolismIn order for free long-chain fatty acids to be converted to acylcarnitine and then transported into the mitochondrial matrix, l-carnitine is a cofactor of multiple enzymes, including acylcarnitine transferases I and II and carnitine translocase. These molecules undergo fJ- oxidation before entering the Krebs cycle, which is where energy production takes place.
Lack of l-carnitine causes the buildup of free fatty acids in the cytoplasm to be toxic to the cell, and the inability of the mitochondria to generate fatty acids results in an energy shortage.
Synthesis of L-carnitine
The Chemical Optical Resolution MethodChemical optical resolution methods state that diastereomers are produced when an optically pure chiral optical resolution agent reacts with D, L-carnitine, or the racemate of its derivatives. The difference in solubility in a suitable solvent is then used to resolve the target diastereomers. The target L-carnitine is produced by hydrolyzing the aforementioned molecule once more. D-camphoric acid, L-tartaric acid, dibenzoyl-D-tartaric acid, dibenzoyl- L-tartaric acid, D-mandelic acid, and N-acetyl-D-glutamic acid are among the frequently used optical resolution agents [10].
Several chemical processes have been suggested for the large-scale synthesis of carnitine. To create two diastereomers that can be separated from one another, the D, L-racemic mixture is typically treated with an optically active acid, such as D-(-)-tartaric acid, D-(+)-camphor- sulfonic acid, (+)-dibenzoyl-D-(-)-tartaric acid, Nacetyl-L-(+)-glutamic acid, and D-(+)- camphoric acid. D-(+)-camphoric acid is utilized as a resolution agent in a racemic combination of D and L-carnitine in the traditional process outlined in U.S. Patent 4,254,053, producing L-(-)-carnitinamide, which is hydrolyzed to generate L-(-)-carnitine, and D-(+)- carnitinamide as a by-product. Nevertheless, a lot of resolution processes are difficult and
expensive, and they always produce equimolar amounts of D-(+)-carnitine or a precursor as a by-product, which has the opposite configuration of L-(-)-carnitine [11].
The Biological Method
The biological technique of making L-carnitine involves the use of enzymes or microbes. Stereo-selective hydroxylation of butyrobetaine with relevant enzymes or stereo-selective hydration of crotonobetaine with relevant enzymes are the two methods used to manufacture L-carnitine from raw materials [11].
Microorganisms capable of converting crotonobetaine into L-carnitine act in an aqueous media to convert crotonobetaine to L-carnitine. A bacterium that can convert crotonobetaine into L-carnitine is defined as one that, when exposed to crotonobetaine in the following circumstances, generates L-carnitine through the action of the microorganism's enzymes on the substrate crotonobetaine,A strain DSM number 3225 (HK 1331b) microorganism is cultured in a bioreactor with growth substrate in the presence of crotonobetaine and/or γ- butyrobetaine [11,12].
The culture fluid is directed outside the bioreactor in a circulation that performs a cell separation. L-carnitine is separated from the cell-free solution by withdrawing a volume of the solution from the bioreactor that is equal to the amount supplied as a substrate. Utilizing the benefits of the novel operating method, the continuous process's biomass retention, increased productivity, and significantly enhanced long-term stability.
An other biological technique for obtaining L-carnitine involves the interaction between trimethylamine and (R)-3,4-epoxybutyric acid. A racemic 3,4-epoxybutyric acid ester is produced by a chemical reaction starting with (R)-3,4-epoxybutyric acid as the primary raw material [11].
Such an ester, according to the biological process, is optically resolved to selectively yield a (R)-3,4-epoxybutyric acid ester, which is then hydrolyzed once more to yield the desired molecule. Excellent stereo-selectivity has been demonstrated by this approach, even though it necessitates precise reaction modulation and a lengthy reaction period of about 24 hours [12].
Use Chiral Material from the Natural SourceThere is a way to make L-carnitine using chiral material derived from a natural source. D- mannitol is utilized as a raw ingredient in this process.Then, L-carnitine is made by a series of stages. There is now a different way to make L-carnitine from (S)-3-activated hydroxybutyrolactone. This approach involves mixing a 25% trimethylamine solution of 2.0 equivalent with (S)-3-activated hydroxybutyrolactone of 1.0 equivalent. After that, the mixture is mixed for an hour at room temperature in a tight container. Furthermore, the combination is reacted for 16 hours at 100 °C to obtain pure L-carnitine; however, the yield is not stated.
(S)-3-activated hydroxybutyrolactone yields L-carnitine. Using traditional chemistry, (S)-3- hydroxybutyrolactone (S-HGB), often referred to as (S)-3-activated hydroxybutyrolactone (S-HGB), is an essential building block for the production of additional chiral intermediates. Gamma-butyrolactone (S)-3-hydroxyl is a type of crucial intermediate in chemical synthesis. Additionally, it is a crucial chiral source (Chira Pool) [11].
(S)-3-hydroxy-γ butyrolactone (S-HGB) can be used to synthesize ezetimibe and linezolid, and it is a precursor to several enantiopure intermediates for chiral medicines, including cholesterol-lowering medications. In synthetic organic chemistry, enantiopure (S)-3-hydroxy- γbutyrolactone and its structurally related C3-C4 compounds are a key target for chiral building blocks [20]. The alcohols and carboxylic acids in optically pure HGBs can be further derived. Among other things, S-HGB can be transformed into (S)-4-Chloro-3- hydroxybutyrate (S-CHB) and then into hydroxy-nitrile (HN) for the manufacture of Lcarnitine, 4-hydroxy-2-pyrrolidone, oxazolidinones, and intermediates of hydroxy-methyl- glutaryl-CoA (HMG-CoA) reductase inhibitors.
The Process used in the Production PlantEpichlorohydrin and trimethylamine are two inexpensive basic ingredients that are typically used in the chemical production of L-carnitine. After the race mate's separation by processes like fractional crystallization. At this stage, optical resolution is challenging. The biotechnological method of producing L-carnitine is more efficient than the chemical method in terms of procedure. Reports state that compared to chemical operations, biotechnological techniques produce 90% less trash for incineration, 25% less wastewater, and about 50% less total organic waste. Consequently, the manufacture of L-carnitine by microorganisms has become more popular [13].
Researchers decided to use the L-carnitine preparation method of (S)-3-activated hydroxybutyrolactone based on comparisons of the available methods. This is because a very simple and low-cost method of preparing (S)-3-activated hydroxybutyrolactone has been developed, which involves oxidizing and successively cyclizing inexpensive natural D- carbohydrates and hydrogen peroxide [13]. There should be a certain prerequisite for (S)-3- activated hydroxybutyrolactone as a raw material. Using this technique, it will be possible to obtain very pure and high yields of L-carnitine by using inexpensive chemicals in aqueous solutions [13].
(S)-3-activated hydroxybutyrolactone undergoes a ring-opening reaction as the initial reaction step. In the following phase of the reaction, the ring-opened molecule of 4- hydroxy3-activated hydroxybutyric acid experiences an epoxidation reaction wherein the presence of a base causes a stereospecific reversal of the chiral center. From there, a salt of 3,4-epoxybutyric acid that is optically pure is made. The final stage of the reaction process is the reaction of (R)-3,4-epoxybutyric acid with trimethylamine to produce L-carnitine. The procedure above produced sodium 3,4-epoxybutyrate, which was not isolated from an aqueous solution containing 25% trimethylamine equivalent was added right away to the reagent solution, and L-carnitine was produced by stirring it for two hours at 45°C
L-carnitine can be extracted and purified from reagent solution using a well-known technique, ideally one that involves cation exchange resin. The optical purity of L-- carnitine obtained with the cation exchange resin method of separation and purification is more than 95%, with a yield of at least 55%. Moreover, a similar outcome can be achieved by reacting trimethylamine with sodium 3,4-epoxybutyrate, which is created during the reaction of epoxybutyric acid.
Four process units go into the creation of L-carnitine. The following are the process units: sodium (R)-3,4-epoxybutyrate preparation, L-carnitine preparation, (S)-3- methanesulfonyl hydroxybutyrolactone preparation, and (S)-4-hydroxy-3-methanesulfonyl hydroxybutyric acid preparation [13].
Reaction of L-carnitine on Various Diseases Male infertilityNumerous investigations have verified increased reactive oxygen species (ROS) overproduction in prostato-vesiculoepididymitis individuals. Moreover, a lower sperm count is associated with a lower level of L-carnitine. Because of this, the use of L-carnitine is advised in the treatment of male infertility, and since the initial controlled and uncontrolled trials, extremely encouraging outcomes have been obtained. There was a considerable reduction in both baseline and provoked ROS generation with the combined use of carnitines, specifically carnitine and acetyl-carnitine complex. Similar to several antioxidants, carnitine/acetyl-- carnitine combination appears to have a restorative effect by either replacing fatty acids in membrane phospholipids or removing increased intracellular harmful acetyl- coenzyme A (acetyl-CoA) [14,15].
Terminate Renal DiseaseHemodialysis eliminates L-carnitine and shortand medium-chain acylcarnitine molecules from the bloodstream. Patients with end-stage renal disease (ESRD) receiving hemodialysis are at risk for developing a progressive carnitine shortage due to a combination of factors, including L-carnitine loss into the dialysate and reduced kidney production. A increased risk of cardiovascular mortality has been linked to a high acylcarnitine-to-L-carnitine ratio, which is caused by inadequate clearance of long-chain acylcarnitine molecules [16,17]. Patients receiving hemodialysis may experience a number of disorders as a result of carnitine depletion, including refractory anemia, anomalies in plasma lipid levels, and weakness and exhaustion of the muscles. Serum C-reactive protein, a marker of inflammation and a predictor of death in patients receiving hemodialysis, and LDL cholesterol decreased when L- carnitine treatment was given orally or intravenously, according to a 2014 systematic review and meta-analysis of 31 randomized controlled trials involving 1,734 patients with ESRD, though the latter was not considered to be significant to be clinically relevant. Other serum lipids (such as total and HDL cholesterol, triglycerides) and anemia-related markers (such as hemoglobin concentration, hemoglobin-related erythropoietin-requiring dose, albumin, and hemoglobin-to-crit ratio) were not affected by L-carnitine [16].
Effect on Heart FailureThe incapacity of the heart to pump enough blood to meet all of the body's requirements is known as heart failure. The buildup of atherosclerotic plaque in the coronary arteries may cause coronary heart disease by preventing the heart's inner regions from receiving enough blood flow, which can lead to cardiac injury and reduced pumping capacity.Heart failure may result from myocardial infarction-related damage to the heart muscle. Furthermore, heart failure may result from the heart's reduced ability to pump blood in dilated cardiomyopathy situations [18]. Measures of exercise tolerance are widely used to track the severity of heart failure since exercise puts more strain on the already compromised heart.The left ventricular ejection fraction (LVEF), an objective indicator of the heart's pumping capacity, is also calculated via echocardiography. Systolic heart failure is indicated by an LVEF of less than 40%. Patients with heart failure who have aberrant acylcarnitine profiles and high acylcarnitine to free carnitine ratios in their blood have been associated with severe illness and a bad prognosis [18].
Effect on Bone MassAs people age, their cells' concentration of carnitine decreases, which has an impact on different tissues' fatty acid metabolism. Bones that depend on osteoblasts for ongoing metabolic and reconstructive processes to maintain bone mass are particularly badly impacted [19]. Osteoporosis is a common condition in the elderly, although it primarily affects women who have gone through menopause. Patients with osteoporosis are more likely to fracture because their bone is more brittle as a result of disturbed bone microarchitecture. It was discovered that giving animals a carnitine mixture—which contains propionyl L- carnitine or one of its pharmacologically acceptable salts—could raise the concentrations of osteocalcin in their serum. In contrast, serum osteocalcin levels in control animals tended to decline with age [20].
Our carnitine levels decrease with aging. Patano and colleagues suggest that this age-related decrease in energy availability may have deleterious effects on osteoblast activity and bone remodeling. Research has shown that fatty acid oxidation produces 40–80% of the energy needed for osteoblastic lineage cells. This implies that regulating the oxidation of fatty acids could regulate the amount of energy accessible to osteoblasts for the creation of proteins [20]. Researchers found that L-carnitine supplementation can affect bone density and minimize bone turnover by decreasing bone loss and boosting bone microstructural characteristics through the use of an aged ovariectomized rat model [21].
Cardiovascular Disease
Patients with severe cardiovascular conditions, such as coronary heart disease, chronic heart failure, and peripheral vascular disease, have been demonstrated to benefit from L-carnitine. Giving L-carnitine to individuals with chronic heart disease during a 12-month period avoided ventricular remodeling and attenuated left ventricular dilatation, which in turn decreased the risk of chronic heart failure and mortality. L-carnitine improves glucose metabolism and lessens the toxicity of elevated free fatty acid levels to lessen cardiac damage during ischemia.(22) It has been established that L-carnitine protects against ST-elevation myocardial infarction. Prompt L-carnitine delivery after an acute myocardial infarction and ongoing maintenance therapy attenuate. gradual dilatation of the left ventricle. At six months, L-carnitine lowers early mortality but not the total risk of death or heart failure. In addition, supplementing with L-carnitine decreases the size of infarcts and cardiac biomarkers, prevents ventricular hypertrophy and dysfunction, and lowers the overall frequency of cardiac events, which includes nonfatal infarction and cardiac fatalities. According to Xue and colleagues, the restoration of myocardial energy stores and the start of normal oxidative metabolism are the reasons behind L-carnitine's positive benefits in cardiovascular disease [23].
It is commonly advised to take supplements containing carnitine if you have cardiovascular disease. But as previously noted, carnitine supplementation exacerbates both injury and recovery of contractile function following brief ischemia in the perfused rat heart when it does not enhance glucose oxidation [23].
Drug InteractionsL-carnitine losses are increased when pivalic acid combines with L-carnitine and is eliminated in the urine as pivaloylcarnitine (see also Secondary carnitine deficit). As a result, extended usage of antibiotics containing pivalic acid, such as cefditoren pivoxil pivampicillin, pivmecillinam, and pivcephalexin, might result in secondary L-carnitine insufficiency. When combined with L-carnitine, the anticonvulsant valproic acid (Depakene) creates a valproylcarnitine ester, which is eliminated in the urine. This disruption of Lcarnitine production occurs in the liver. However, only a small percentage of valproic acid users require L-carnitine supplementation. Young age (less than 2 years), significant neurological issues, usage of many antiepileptic medications, poor nutrition, and ketogenic diet intake are risk factors for L-carnitine shortage with valproic acid.
Reaction to Muscle injury of L-CarnitineMuscle soreness and injury brought on by exercise can both lower quality of life and restrict training. L-carnitine has been shown to improve exercise performance in addition to aiding in post-exercise recovery through a variety of methods. On the other hand, performance during a second round of intense cycling exercise after three hours was not enhanced by a single administration of l-carnitine [24,25].
L-carnitine supplementation was found to reducediscomfort, soreness, and the release of creatine kinase, a muscle marker, in a cross-over trial. This suggests that the vitamin is beneficial in preventing tissue rupture and the resultant leaking of cytosolic proteins [26]. The beneficial effects of l-carnitine on lowering exercise-induced hypoxia, ensuing muscle damage, and delayed onset muscle soreness (DOMS) were further supported in a series of studies conducted by Kraemer and colleagues [27]. It was possible to show that daily use of 2 g l-carnitine, as opposed to a placebo, decreased muscle disruption during intense exercise using the magnetic resonance imaging (MRI) technique [18]. Along with this, there was a notable drop in purine metabolism indicators including hypoxanthine and xanthine oxidase, as well as released cytosolic proteins such myoglobin, creatine kinase, and malondialdehyde (MDA) [28]. In one investigation, the effects of two distinct l-carnitine dosages on these metabolic indicators and the subjective perception of muscle soreness were compared [29]. The researchers found that supplementing with 1 g and 2 g of l- carnitine daily produced similar advantages, adding to the body of evidence supporting the supplement's potential.The researchers also found that over three weeks, supplementing with l-carnitine l-tartrate, or 2 g of l-carnitine daily, increases the amount of androgen receptors on muscle cells, which enhances protein signaling, which is necessary for muscle cell repair and post-exercise recovery [30].
Reaction on Blood Flow and Endothelial FunctionBy guarding against carnitine deficit in endothelial cells, l-carnitine supplementation decreased structural and biochemical muscle damage and facilitated tissue repair, improving blood flow and oxygen supply.(30) Dubelaar and Hülsmann's early research served as the foundation for the new paradigm [31,32]. Here, it was shown that, both in the absence of enhanced muscle l-carnitine level and upon l-carnitine infusion, dogs' muscle contractile force was markedly boosted and accompanied by an elevated blood flow [32]. Furthermore, during ischemia, l-carnitine extends endothelial cells' capacity to control blood flow. This suggested a process separate from the accumulation of muscle l-carnitine and energy generation. The authors postulated that enhanced force resulted from a change in the capillaries encircling the muscle [32].
Nuesch et al.'s findings confirmed this vascular effect. It was demonstrated that following maximal exercise, plasma carnitine levels in athletes taking 1 g of l-carnitine remained elevated as opposed to significantly declining in athletes not taking supplements [33]. In a cross-over study, Volek et al. looked into the flow-mediated dilation (FMD) following a high-fat meal to learn more about the impact of l-carnitine on endothelial cell function.
Following three weeks of l-carnitine supplementation, peak FMD reduced in the placebo arm but post-prandial brachial artery FMD rose in response to a five-minute upper arm occlusion [33]. These findings provide credence to the theory that l-carnitine improves vascular function by modulating endothelial function [33].
L-Carnitine as an Anti-OxidantThe function of l-carnitine supplementation in reducing oxidative stress during exercise is one of the possible processes underlying this effect. Muscle damage is mostly brought on by acute cellular and structural injury as well as following biochemical reactions during tissue regeneration, particularly during eccentric exercise (active force producing lengthening contractions) [34,35]. Long-term dysfunction can result from modifications to the surrounding tissue and sarcomeres of muscle fibers, allowing the healing process to last up to ten days. By distancing ATP synthesis from the Krebs cycle from cell energy use, local hypoxia brought on by exercise may potentially exacerbate inflammation and muscle damage [36].
Reactive oxygen species may occur as a result of this (ROS). In the end, the release of intracellular components into the interstitium and the ensuing inflammation cause DOMS, which is characterized by discomfort, edema, and rigidity of the muscles in addition to pain when moving [16]. These events are caused by molecules like MDA, hypoxanthine, or creatine kinase that are produced when sarcolemma rupture occurs. Parandak et al. also reported on the antioxidant benefits of l-carnitine on exercise-induced oxidative stress. When compared to a placebo before and 24 hours after exercise, daily administration with 2 g l- carnitine over 14 days significantly enhanced total antioxidant capacity. However, indices of muscle injury and lipid peroxidation remained significantly lower [16]. Additionally, Parthimos et al. discovered that l-carnitine administration after training enhanced the overall antioxidant status that basketball players otherwise showed in the absence of supplementation [16].
Ho and colleagues initially presented experimental evidence indicating a positive impact on recovery after exercise in middle-aged healthy men and women, with an average age of 45 and 52, respectively [17]. However, the majority of these investigations were conducted in young, healthy volunteers. L-carnitine supplementation, once again, attenuated a rise in stress markers during and after exercise, such as muscle pain as reported by the individuals [17].
Reaction of L-Carnitine on AgingAging might offer insights into the future course of l-carnitine research and application. Although studies on the benefits of l-carnitine ingestion in physically demanding conditions have shown that the healthy young to middle-aged population can benefit from it, the effects of l-carnitine intake in physically exhausted senior individuals are still unknown. Sarcopenia is the name for the age-related decrease in skeletal muscle mass, strength, and general activity. It is a complex age-related disorder. Sarcopenia is caused by various factors, including reduced mobility, poor nutritional health, and a deterioration in mitochondrial activity [37].
As sarcopenic subjects age, changes in protein metabolism and a decrease in protein synthesis have been documented [38]. While the balance of proteolytic and anabolic processes controls protein metabolism in young, healthy persons, sarcopenia results in a lack of sufficient protein synthesis and increasing breakdown, which in turn causes physical weakness in elderly individuals [37]. According to a recent study using the nematode Caenorhabditis elegans, some aggregation proteins may be involved in the age-related decrease of muscular mass. A further process contributing to the age-related decrease of muscle mass is the progressive reduction in anabolic stimulus sensitivity. Furthermore, the loss of type II fibers was linked to this deterioration in the elderly [39].
Diet and physical activity are two factors that can affect sarcopenia. It has been demonstrated that eating meat and resistance training work in concert to improve older people's muscle endurance and strength as well as their ability to synthesize muscle proteins [40]. Furthermore, senior citizens' physical performance can be enhanced and their muscle growth and strength increased with supplemented protein intake. Nevertheless, additional research revealed that protein doesn't improve muscle development and function in this population on its own or in the absence of exercise [40].
An increasing body of research indicates that l-carnitine can reverse the age-related decline in muscular function and have a favorable impact on muscle hypertrophy. In healthy individuals, there is a documented decrease in muscle l-carnitine content as people age.
Additionally, aging results in decreased transcription of the l-carnitine transporter, OCTN2 mRNA [40], suggesting that aging impairs the distribution and homeostasis of l-carnitine in tissues. As a result, several research looked into the part l-carnitine plays in aging
Malaguarnera et al. conducted a 6-month clinical trial on centenarians who were given a placebo or 2 g of l-- carnitine daily to examine the impact on both physical and mental exhaustion. Supplementation produced better walking ability, decreased total fat mass, and increased muscle mass as compared to the placebo group, indicating a positive impact in this demographic [41]. These results are consistent with other studies conducted by the same group which demonstrated that muscle mass grew while body fat mass decreased in the elderly. Alongside this, there was a noticeable decrease in both physical and mental exhaustion [42]. Supplementing with acetyl-l-carnitine, the acetylated derivative of l- carnitine, also lessened both physical and mental exhaustion in subjects 70 years of age and above. Pre-frail older people with a mean age of 68 years were included in a double-blind, randomized, placebo-controlled clinical trial by Badrasawi et al., which demonstrated a substantial improvement in frailty status after giving 1.5 g l-carnitine daily for 10 weeks [43]. A recent study by Evans et al. shown the beneficial effects of L-carnitine, creatine, and leucine on muscle mass and performance [43].
After eight weeks of supplementation, researchers compared the possible synergistic effect of this unique for mulation to a placebo in this randomized, placebo-controlled, double blind study involving individuals ages 55–70. In comparison to a placebo, it was discovered that patients considerably increased overall lean muscle mass, leg lean muscle mass, and leg strength as well as improved a composite outcome measure of body mass, muscular strength, and a 6-minute walk test. Supplementing with l- carnitine alone did not significantly increase the composite parameter when compared to placebo; however, subjects maintained their leg muscular strength and composite score relative to baseline, while both dropped during the course of the research in the placebo group.
Even though several studies in the younger population were unable to demonstrate weight loss following l-carnitine intake, Pooyandjoo, and colleagues concluded in a recent meta- analysis that subjects receiving l-carnitine experienced a significant reduction in body weight when compared to the control groups [44]. The majority of the research that made up the meta-analysis involved patients who were obese or diabetic [44].
Some of the general mechanisms of action of l-carnitine effects demonstrated in animal studies and younger athletes can apply, even if the processes behind the effects of l-carnitine in boosting muscle development and function in older persons are yet unknown.
Supplemental l-carnitine spared amino acids by turning fat into energy, which resulted in swine muscle protein accumulation [45]. A possible method by which l-carnitine inhibits the breakdown of muscle protein is indicated by Keller and colleagues' demonstration of the role of l-carnitine in the transcriptional control of genes involved in the ubiquitin proteasome system of the piglet's skeletal muscle. Furthermore, it has been documented that l-carnitine raises IGF-1 and Akt, which triggers the mammalian target of rapamycin (mTOR) signaling pathway, a crucial regulator of protein anabolism [46].
Peroxidative damage accelerates the aging process, according to the free radical hypothesis of aging. Reactive oxygen species can be scavenged by antioxidants or their creation can be stopped, reducing oxidative stress. Numerous clinical investigations have demonstrated the antioxidant qualities of l-carnitine, pointing to a possible new mechanism of action by which l-carnitine may prevent the metabolic processes responsible for tissue aging [47,48]. Accelerated neuronal cell damage and death, which results in brain shrinkage and a reduction in brain function, is another feature of aging. It was proposed that the main underlying process might be mitochondrial degradation. Nicassio et al. have proposed that acetyl-l- carnitine affects mitochondrial homeostasis in the brains of aged rats [49].
Conclusion
Scientific research has examined the role of l-carnitine in various indications, as it is an important component in energy production and fatty acid metabolism. Professional athletes have utilized l-carnitine as an ergogenic aid, and physically active people have used it as a nutritional supplement. Many human studies with resistance-trained athletes, untrained men and women, or healthy active people looked at how the dietary supplement affected muscle strength, oxygen capacity, or physical performance. Clinical research has recently focused on testing the theory that l-carnitine supplementation speeds up the healing process following physical activity. According to scientific research, l-carnitine supplementation can help athletes since it lessens the negative effects of high-intensity training by lowering the degree of exercise-induced hypoxia and muscle injury.
Fatty acid β-oxidation is not limited by the supply of l-carnitine when conditions are healthy and stress-free. Urinary excretion, transport, and bioavailability all play a major role in controlling its homeostasis. However, l-carnitine supplementation has been demonstrated to improve endurance and muscle tone and function in circumstances characterized by aberrations, such as hemodialysis, inborn or acquired carnitine deficit, and sarcopenic and frail patients. Both exercise and dietary changes can stop the age-related loss of muscle mass. While moderate exercise combined with dietary supplements may be a potential method to slow down the onset of sarcopenia, a characteristic of frailty in older persons, endurance exercise can be difficult for the elderly. An increasing amount of research conducted on animals has demonstrated the complex processes through which l-carnitine promotes greater protein synthesis and less muscle breakdown. Furthermore, age-related reductions may be influenced by l-carnitine's modulation of mitochondrial homeostasis during aging. Thus, by delaying the rate at which muscle mass and function loss and neurodegeneration occur, dietary supplements containing l-carnitine may benefit during the aging process. In this area, more investigation is necessary. In summary, the structural and symptomatic effects of high- intensity exercise, such as pain and impaired muscle sarcomeres, not only lower quality of life but also limit the ability to train further. For this reason, l-carnitine supplementation that promotes recovery from exercise is especially advantageous for the healthy, young, active population. Furthermore, older adults who are losing lean muscle mass and function, have lower muscle l-carnitine levels, and have mitochondrial dysfunction can also gain from taking a l-carnitine supplement. In instance, the value of l-carnitine in this population will only increase as more older participants engage in moderate activity
- Golledge J, Quigley FG (2003) Pathogenesis of varicose veins. European Journal of Vascular and Endovascular Surgery. 25.
- Hulekar S, Chandarlal Poolya M (2022) Varicose Veins and Homoeopathy. © Journal of Medical and Pharmaceutical Innovation 9.
- Raetz J, Wilson M, Collins K (2019) Varicose veins: Diagnosis and treatment. Am Fam Physician. 99.
- PiazzaG (2014) Varicose veins Circulation. 130: 582-7
- Aslam MR, Muhammad Asif H, Ahmad K, et al. (2022) Global impact and contributing factors in varicose vein disease development. SAGE Open Med 10.
- Mansilha A. Early Stages of Chronic Venous Disease: Medical Treatment Alone or in Addition to Endovenous Treatments.
- Ahti Tiina (2010) Risk Factors of Varicose Veins. Tampere Univ Pr.
- GOLDMAN MP, FRONEK A (1989) Anatomy and Pathophysiology of Varicose Veins. J Dermatol Surg Oncol 15.
- Bergan JJ (1994) Diagnosis and treatment of varicose veins: A review. J Am Acad Dermatol 31.
- Youn YJ, Lee J (2019) Chronic venous insufficiency and varicose veins of the lower extremities. Korean Journal of Internal Medicine 34.
- Millan SB, Gan R, Townsend PE (2019) Venous ulcers: Diagnosis and treatment. Am Fam Physician 100.
- Langridge BJ, Onida S, Weir J, Moore H, Lane TRA, Davies AH (2020) Cyanoacrylate glue embolisation for varicose veins – A novel complication. Phlebology 35.
- Dimech AP, Cassar K (2020) Efficacy of Cyanoacrylate Glue Ablation of Primary Truncal Varicose Veins Compared to Existing Endovenous Techniques: A Systematic Review of the Literature. The Surgery Journal 06.
- Tang TY, Kam JW, Gaunt ME (2017) ClariVein® – Early results from a large single-centre series of mechanochemical endovenous ablation for varicose veins. Phlebology 32.
- Li N, Li J, Huang M, Zhang X (2021) Efficacy and safety of polidocanol in the treatment of varicose veins of lower extremities: A protocol for systematic review and meta-analysis. Medicine (United States) 100.
- Faccini FP, Ermini S, Franceschi C (2020) CHIVA to Treat Saphenous Vein Insufficiency in Chronic Venous Disease: Characteristics and Results. J Vasc Surg Venous Lymphat Disord 8.
- Faccini FP, Ermini S, Franceschi C (2023) CHIVA to treat saphenous vein insufficiency in chronic venous disease: Characteristics and results. J Vasc Surg Venous Lymphat Disord 11.
- Atasoy MM, Oğuzkurt L (2016) The endovenous ASVAL method: Principles and preliminary results. Diagnostic and Interventional Radiology 22.
- Jiang Q (2014) Natural forms of vitamin E: metabolism, antioxidant, and anti-inflammatory activities and their role in disease prevention and therapy. Free Radic Biol Med 72: 76-90.
- Glynn RJ, Ridker PM, Goldhaber SZ, Zee RYL, Buring JE (2007) Effects of random allocation to vitamin E supplementation on the occurrence of venous thromboembolism: report from the Women’s Health Study. Circulation. 116: 1497-503.
- Antoniades C, Tousoulis D, Tentolouris C, et al. (2003) Effects of antioxidant vitamins C and E on endothelial function and thrombosis/fibrinolysis system in smokers. Thromb Haemost 89: 990-5.
- Aguirre R, May JM (2008) Inflammation in the vascular bed: importance of vitamin C. Pharmacol Ther 119: 96-103.
- Mateuszuk Ł, Campagna R, Kutryb-Zając B, et al. (2020) Reversal of endothelial dysfunction by nicotinamide mononucleotide via extracellular conversion to nicotinamide riboside. Biochem Pharmacol 178: 114019.
- Dionisio N, Jardín I, Salido GM, Rosado JA (2010) Homocysteine, intracellular signaling and thrombotic disorders. Curr Med Chem 17: 3109-19.
- Geleijnse JM, Vermeer C, Grobbee DE, et al. (2004) Dietary Intake of Menaquinone Is Associated with a Reduced Risk of Coronary Heart Disease: The Rotterdam Study. J Nutr 134: 3100- 5.
- Beulens JWJ, Bots ML, Atsma F, et al. (2009) High dietary menaquinone intake is associated with reduced coronary calcification. Atherosclerosis 203: 489-93.
- Donaldson MS (2015) Vitamin K: the missing link to prostate health. Med Hypotheses 84: 219-22.
- Kandasamy Palanisamy J, Ponnu S, Mani S, Balakrishnan S (2018) A CRITICAL REVIEW ON TRADITIONAL HERBAL DRUGS: AN EMERGING ALTERNATIVE DRUG FOR VARICOSE VEINS. Palanisamy et al World Journal of Pharmaceutical Research. 7: 316.
- Dwyer HC, Baranowski DC, Mayer PV, Gabriele S (2018) LivRelief varicose veins cream in the treatment of chronic venous insufficiency of the lower limbs: A 6-week single arm pilot study. PLoS One 13.
- Parihar S, Sarswati, Chattarpal, Sharma D (2022) A Brief Review on Herbs Used in the Treatment of Varicose Veins. Journal of Drug Delivery and Therapeutics 12.
- Garg N, Jain A. AYURVEDIC PERSPECTIVE OF VARICOSE VEINS. Nidhi et al World Journal of Pharmaceutical Research. 6: 296.
- Ernst E (1999) Herbal medications for common ailments in the elderly. Drugs Aging 15.
- AG, AKS (2017) The Pharmacological Potential of Rutin. Saudi Pharmaceutical Journal 25.
- Patel K, Patel DK (2019) The Beneficial Role of Rutin, A Naturally Occurring Flavonoid in Health Promotion and Disease Prevention: A Systematic Review and Update. In: Bioactive Food as Dietary Interventions for Arthritis and Related Inflammatory Diseases.
- Review AM, Reserved AR, Reprint N, Written W (2001) Monograph Ruscus aculeatus (Butcher ’ s Broom). Alternative Medicine Review 6.
- Lichota A, Gwozdzinski L, Gwozdzinski K (2019) Therapeutic potential of natural compounds in inflammation and chronic venous insufficiency. Eur J Med Chem 176.
- Chong NJ, Aziz Z (2013) A systematic review of the efficacy of centella asiatica for improvement of the signs and symptoms of chronic venous insufficiency. Evidence-based Complementary and Alternative Medicine.
- Chan JYY, Yuen ACY, Chan RYK, Chan SW (2013) A review of the cardiovascular benefits and antioxidant properties of allicin. Phytotherapy Research 27.
- Bal S, Sharangi AB, Upadhyay TK, et al. (2022) Biomedical and Antioxidant Potentialities in Chilli: Perspectives and Way Forward. Molecules 27.
- Bischoff-Kont I, Fürst R (2021) Benefits of ginger and its constituent 6-shogaol in inhibiting inflammatory processes. Pharmaceuticals 14.
- Narnoliya LK, Jadaun JS, Singh SP (2019) The Phytochemical Composition, Biological Effects and Biotechnological Approaches to the Production of High-Value Essential Oil from Geranium. In: Essential Oil Research.
- Matić M, Đuran V, Jovanović M, et al. (2013) Treatment of venous leg ulcers with an ointment containing yarrow (Achillea millefolium) extract / Primena preparata sa ekstraktom hajdučke trave (Achillea millefolium) u lečenju venskih ulkusa potkolenice. Serbian Journal of Dermatology and Venerology 1.
- Kühnl J, Tao TP, Brandmair K, et al. (2021) Characterization of application scenario-dependent pharmacokinetics and pharmacodynamic properties of permethrin and hyperforin in a dynamic skin and liver multi-organ-chip model. Toxicology 448.
- Patil K, Sanjay C, Doggalli N, Devi KR, Harshitha N (2022) A Review of Calendula OfficinalisMagic in Science. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH. Published online.
- Arora D, Rani A, Sharma A (2013) A review on phytochemistry and ethnopharmacological aspects of genus Calendula. Pharmacogn Rev 7: 179-87.
- Givol O, Kornhaber R, Visentin D, Cleary M, Haik J, Harats M (2019) A systematic review of Calendula officinalis extract for wound healing. Wound Repair and Regeneration 27: 548-61.
- Suter A, Bommer S, Rechner J (2006) Treatment of patients with venous insufficiency with fresh plant horse chestnut seed extract: A review of 5 clinical studies. Adv Ther 23.
- Bielanski TE, Piotrowski ZH (1999) Horse-chestnut seed extract for chronic venous insufficiency. J Fam Pract. 48.
- Horse-chestnut seed extract for chronic venous insufficiency: a systematic review. Focus on Alternative and Complementary Therapies 4.
- Tilgner S. A Herbal Newsletter From Wise Acres Farm Herbal Transitions E-Zine: Reprint for Www.Herbaltransitions. Com Email List Varicose Veins & Hemorrhoids. www. herbaltransitions.com
- Yang R, Yuan BC, Ma YS, Zhou S, Liu Y (2017) The antiinflammatory activity of licorice, a widely used chinese herb. Pharm Biol 55.
- Dida Bulbula D (2021) Cancer Ther Oncol Int J Comprehensive Review on Turmeric (Curcuma Longa l.) as Medicinal Plant and its Nutraceutical Quality to Human Cancer Therapy & Oncology International Journal. Cancer Ther Oncol Int J. 18.
- Onkaramurthy M, Vishwakarma KK, Singh P, et al. (2022) Herbal Formulations Ameliorates Chronic Venous Insufficiency, Venotonicity and Elastase Inhibition in the Management of Varicose Veins: A Preclinical Study. Indian J Pharm Sci 84.
- G.K. S, Muralidhara, M.S. Bharath M (2011) Exploring the Role of “Brahmi” (Bacopa monnieri and Centella asiatica) in Brain Function and Therapy. Recent Pat Endocr Metab Immune Drug Discov 5
- Gulati OP (2014) Pycnogenol® in chronic venous insufficiecy and related venous disorders. Phytotherapy Research 28.
Table 1
S.N. |
Plant Name |
Family |
Ingeredient Responsible For Activity |
Structure |
Plant Part Use |
Benefits |
1. |
Stone root |
Lamiaceae |
Rutin |
|
Root and rhizome |
Antioxidant and anti- inflammatory |
2. |
Butcher's broom |
L i li ace ae (Ruscus aculeatus) |
Ruscogenin |
|
leaves and rhizome |
Anti- inflammatory, vasoconstrictor, antihemorrhagi c |
3. |
Cinnamon |
L a urace ae (Cinnamomu m verum) |
Cinnamaldehyde, cinnamic acid and cinnamate |
|
Inner bark |
Anti-inflammatory, antioxidant, |
4. |
Gotu kola |
Umbelliferae (Centella asiatica) |
|
Antioxidant and anti- inflammatory |
||
5. |
Garlic |
Amaryllidacae (Alliums tivum) |
Allicin |
|
Leaves, flower, and cloves |
Antioxidant and |
6. |
Cayenne pepper |
Solanaceae (Capsicu annum) |
Capsaicin |
|
Seedand fruits |
Antioxidant and |
7. |
Ginger |
Z in g i b erace ae (Zingiber officinale) |
Gingerol |
|
Rhizome, ginger root |
Antioxidant and |
8. |
Witch hazel |
Hamamelidaceae (Hamamelis virginiana) |
Tannins, flavonoids, and other polyphenols |
|
Bark |
Astringent, antioxidant and anti- inflammatory |
9. |
Geraniu m |
Geraniaceae (Pelargonium gra- veolens) |
Geraniol, citronellol, and linalool |
|
Roots |
Antispasmodic, anti- oxidant and anti- inflammatory |
10. |
Oak bark |
Fagaceae (Quercus spp.) |
Tannins, flavonoids, a n d other polyphenols |
|
Bark |
Astringent, anti inflammatory, and antioxidant |
11. |
Yarrow |
Asteraceae (Ach- illea millefolium) |
Chamazulene and bisabolol |
|
Flowers and leaves |
Anti-inflam- matory, |
12. |
Saint John's Wort |
Guttiferae (Hypericum perforatum) |
Hypericin, hyperforin, |
|
Flowering tops |
Anti-inflam- matory |
13. |
C a len - dula |
Asteraceae (Calendula officinalis) |
Flavonoids, triterpenoids, carotenoids, |
|
F l o w e r s priorto ful- ly opens |
antisepti- canti-in- flammato- ry,antiox- idant, and astringent |
14. |
Horse ches nut |
Sapindaceae (Aesculus hippocastanum) |
Aescin |
|
Ripe ches nut and bark |
Anti-inflammatory, anti-edematous,and venotonic properties |
15. |
Agrimoy |
Rosaceae (Agrimonia eupatoria) |
Quercetin and rutin |
|
Aerial parts |
anti-inflammatory, antioxidant, and astringent |
16. |
Slippery elm |
Ulmaceae (Ulmus rubra) |
Plant's mucilage |
|
Inner bark |
Anti-inflammatry |
17. |
Comfrey |
Boraginaceae (Sym- phytum officinale) |
Allantoin, rosmarinic |
|
Root and main rib of leaves |
Anti- inflammatory, astringent |
18. |
Red root |
Rhamnaceae (Ceanothus americanus) |
Quercetin |
|
Root |
Antioxidant that has anti-inflammatory and antiplatelet |
19. |
Licorice |
Fabaceae (Glycyrrhi- za glabra) |
Glycyrrhizin |
|
Roots |
Anticoagulant, anti- inflammatory |
20. |
Turmeric |
Zingiberaceae (Curcuma longa) |
Curcumin, turmerone, atlantone, |
|
Rhizome s |
Anti- inflammatory, anticoagulant and antioxidant |
|
|
|
|
|
|
|
21. |
Hazel |
Betulaceae (Ham melis virginiana) |
Tannins |
|
Fruits |
Anti-inflammatry, antioxidant, astrigent and venoton action |
22. |
Raw potatoes |
Solanaceae (Solanum tuberosum) |
Vitamin, potassium, and fiber |
|
Fruit pulp |
Paste is used on varicose veins legs |
23. |
Raw Grated Apples |
Rosaceae (Malus pumila) |
Vitamins, minerals, |
|
Fruit pulp |
Apple cider vinegar used |
24. |
Brahmi |
Plantaginaceae (Bacopa monnieri) |
Bacosides and sapnins |
|
Leaves and stems |
Neuroprotectiv e andantioxidant, anti- inflammato- ry |
25. |
Pine |
Pinaceae (Pinus) |
Procyanidins and flavonoids, phenolic acids |
|
Bark |
Anti- inflammato- ry, antioxidant |
 Quercetin Whole plant
Quercetin Whole plant 
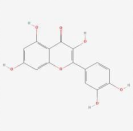
Table 1: Details of herbs that can be used in the treatment of varicose veins
FIGURE 1
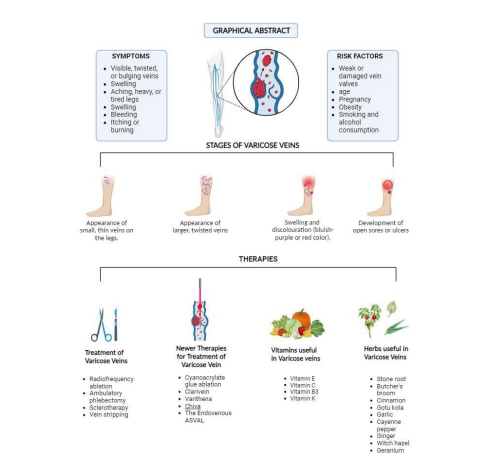
Figure 1:
Tables at a glance
Figures at a glance