Lumbago in Adolescents Revealing Type 1 Neurofibromatosis
Received Date: April 27, 2023 Accepted Date: May 27, 2023 Published Date: May 30, 2023
doi: 10.17303/jnnd.2023.11.103
Citation: Anna Modji Basse, Halladain Mpung Mansoj, Adjaratou Dieynabou Sow, Cissé Ousmane, Diagne Ngor Side (2023) Lumbago in Adolescents Revealing Type 1 Neurofibromatosis about A Presentation. J Neurophysiol Neurol Disord 11: 1-6
Abstract
Neurofibromatosis type 1 (NF1) is an inherited disease caused by pathogenic variants of the NF1 gene present on chromosome 17 is an autosomal dominant disease of which occurs de novo. The cardinal signs of NF1 are cafe-au-lait spots and cutaneous neurofibromas.
The ideal imaging is based on the realization of nuclear magnetic resonance imaging. The treatment is based on the surgical removal of the tumor but report recurrence and malignant transformation that requires radiotherapy.
Observation
We present the case of a 14-year-old teenager who came for consultation for a progressive spinal deformity. History of neurofibromatosis in his paternal grandfather.
General Physical Examination
A good general condition and good coloring of the mucous membranes Presents hypochromic spots on the anterior and posterior thoraxes. Neurological examination shows an abolition of the left patellar reflex associated with low back pain without irradiation. The scanner revealed hypertrophy of the left L4 root of 12.8 mm in probable conflict with the disc.
The diagnosis of segmental type 1 neurofibromatosis was made in the face of this strictly unilateral attack, in a familial context and with systemic involvement.
Therapeutically, partial excision of the tumor volume. Histology confirmed the clinical absence of Lisch nodules, but did not show proliferation of neural crest cells in the choroid responsible for hyperplasia. Diagnosis of established neurofibromatosis types1.
Keywords: Neurofibromatosis; lumbago; Chromosome; Mucous Membranes
Introduction
Neurofibromatosis type 1 (NF1) is an inherited disease caused by pathogenic variants of the NF1 gene present on chromosome 17 (1) The approximate diagnostic prevalence is 1 in 3,000 to 4,000 people worldwide [2,3] It is an autosomal dominant disease of which 50% occurs de novo [4].The cardinal signs of NF1 are café-au-lait spots and cutaneous neurofibromas.
Spinal lesions in NF1 are of particular importance because they can lead to distressing neurological deficit, pain, deformity, and functional disability [5]. The lesions most often cited in the literature are dural ectasia, spinal deformities, spinal nerve root tumors and plexiform tumors.
Hypertrophy of the left L4 root of 12.8 mm in probable conflict with the disc which could evoke neurofibromatosis.
Discussion
Among the different variants of neurofibromatosis only for NF1 and NF2 National Institute of Health (NIH) [6] has established diagnostic guidelines as described in the literature.
The NF1 gene corresponds to chromosomal band 17q11.1.
NF2, which is much less common (incidence at birth approximately 1/33,000) and associated with significant morbidity and mortality due to the frequent location of lesions in the brain and spinal cord. The NF2 gene mutation corresponds to chromosomal band 22q12.6 The most important finding for the diagnosis of NF2 is the presence of bilateral schwannomas involving the eighth cranial nerve, with an incidence of approximately 95% of patients. People with NF2 also have an increased risk of developing single or multiple meningiomas and peripheral nerve schwannomas.
Genetic and molecular analysis performed on the tumors of these patients revealed that it is possible to name schwannomatosis as a distinct clinical and genetic syndrome [7].
Schwannomatosis is therefore defined as an extremely rare tumor syndrome characterized by the presence of multiple schwannomas in the absence of typical signs of NF1 and NF2 syndromes. Typically, patients with schwannomatosis develop cranial, spinal, or peripheral nerve schwannomas but do not develop vestibular lesions (VS), typical of NF2. Schwannomas are benign, encapsulated, slowly growing peripheral nerve tumors. They one- third of all primary benign spinal tumors [8].Our patient presented an isolated schwannoma of a lumbar nerve root, this isolated aspect was reported in the literature but also it is possible to find multiple locations involving several nerves
[9] the presence of schwannomas can be responsible for a vertebral deformity such than scoliosis.
Nevertheless, the hypothesis of certain authors on an ectopic origin of CNS neuromas is validated by their encounter with intracerebral neuromas [10]. Since schwanno mas localized in all parts of the CNS have been described, it is also probable that several mechanisms contribute to their development.
In the literature, the authors report erosion of the vertebral somas, mainly in the peduncles and the foramina.As well as surgical damage during tumor removal, can cause instability resulting in deformation of the corresponding spinal tract [11].
The tumor presents a ubiquitous evolution at the level of the spine [12], even if a major incidence at the level of the cervical and lumbar tracts is reported [13]. In 2 cases reports a predilection to the cervical-lower tract and to the lumbosacral tract the passage is reported [14].
In one study, the highest incidence was in the lumbosacral tract (48.60%) with a peak between L1 and L3; the dorsal tract (33.96%) was second with a peak between T7 and T12; and the peak in the cervical tract (18.43%) was between C4 and C8. (15) The lumbar location is linked to the presence of a greater concentration of roots coming from the lumbar plexus) intended for the innervation of the lower limbs at these levels. Imaging itself, especially magnetic resonance imaging (MRI), allows for early diagnosis and more valid prognosis after surgical treatment [16,17].
Our patient did not have the financial means to carry out this imaging from which we contented ourselves with the lumbar scanner and on the basis of the anamnestic elements to establish the diagnosis. Treatment is based on surgical removal of the tumour. Complete removal of the tumor is the ultimate goal; in fact, case reports, which confirmed recurrence after subtotal excision.
In one series, the authors encountered 3 cases of malignant neuroma, 1 of which was in NF2 at the cervical level in C1, and the patient died 20 days after the intervention. In another case, without Recklinghausen at C6, the patient died 2 months later of recurrence [18].
In a third case of neuroma on D12, after excision, the patient underwent radiotherapy and died 2 years after the operation. According to Celli [19], the preoperative symptoms, the preoperative neuro radiological diagnosis and the clinical signs are often not sufficient to suspect a malignant form of neuroma. Unlike cases of more malignant lesions, such as gliomas, complete removal of intramedullary neuromas is feasible and obviously the best clinical outcome and helps prevent possible recurrences.
Conclusion
Neurofibromatosis represents a multi-systemic disease whose clinical manifestation depends on the location. In the face of a clinical suspicion, always carry out a radiological and neurophysiological assessment which can guide the diagnosis. The ideal imaging is based on the realization of nuclear magnetic resonance imaging. The treatment is based on the surgical removal of the tumor but report recurrence and malignant transformation that requires radiotherapy.
- Kallionpää (2022) Prevalence of neurofibromatosis type Google Scholar.
- Evans (2022) Birth incidence and prevalence of tumour prone Google Scholar.
- Gutmann (2022) Neurofibromatosis type 1 - Google Scholar.
- Huson (2022) Von Recklinghausen neurofibromatosis: a clinical Google Scholar.
- Gutmann (2022) Neurofibromatosis type 1 - Google Scholar.
- Baser Increasing the specificity of diagnostic criteria. Google Scholar.
- Seppälä (2022) Multiple schwannomas: schwannomatosis Google Scholar
- Mautner (2022) Spinal tumors in patients with neurofibromatosis Google Scholar.
- Daras (2022) Multiple spinal intradural schwannomas in Google Scholar.
- Bharati (2022) Intramedullary schwannoma-Google Scholar.
- Yasuoka (2022) Incidence of spinal column deformity after Google Scholar
- Seppälä (2022) Long-term outcome after removal of spinal. Google Scholar.
- Miura (2022) Resection of cervical spinal neuroma including. Google Scholar.
- Klekamp (2022) Introduction of a score system for the clinical. Google Scholar.
- Batch (2022) Cervical neuromas with extradural components Google Scholar.
- Klekamp (2022) Introduction of a score system for the clinical Google Scholar.
- Pansini A, Conti P, Conti R (1987) Diagnosis early compressioni _ mielo- radicolari . RX-TCRM Piccin Ed Padova.
- Dini M, Caldarella A, Russo GL, Conti P (1997) Tumore malignant della guaina dei nervi periferici (MPNST)-Post-irradiazione. Pathological 89: 441-5.
- Celli (2022)Primary spinal malignancy schwannomas: clinical Google Scholar.
Figure1

Figure1: Picture types coffee with milk
Figure 2
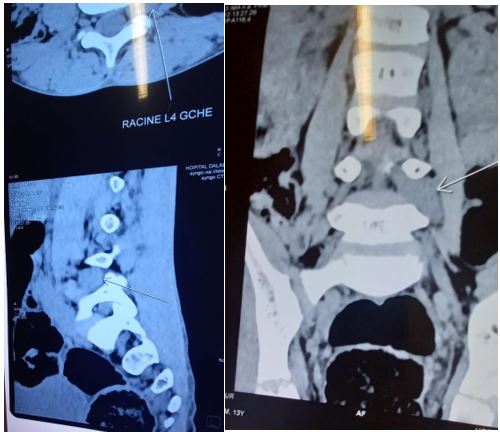
Figure2: CT lumbar spine
Figures at a glance