Computational Intelligence at the Neurological Frontier: Recent Advances and Emerging Paradigms in Computational Neuroscience
Received Date: June 25, 2026 Accepted Date: July 01, 2026 Published Date: July 04, 2026
doi:10.17303/jnnd.2026.14.101
Citation: Mohammad Yaghoub Abdollahzadeh Jamalabadi (2026) Computational Intelligence at the Neurological Frontier: Recent Advances and Emerging Paradigms in Computational Neuroscience. J Neurophysiol Neurol Disord 14: 1-31
Abstract
Background: The convergence of artificial intelligence, machine learning, and clinical neuroscience has reshaped how researchers’ model, diagnose, and treat neurological disorders. Between 2024 and mid-2026, methodological breakthroughs spanning large language models (LLMs), graph neural networks (GNNs), digital twin brain simulators, multimodal deep learning, and brain-computer interfaces (BCIs) have substantially expanded the computational toolkit available to neurological sciences.
Methods: This narrative review synthesizes peer-reviewed literature and selected landmark preprints published between January 2024 and June 2026. A structured literature search across PubMed, IEEE Xplore, Scopus, Web of Science, arXiv, and bioRxiv identified 78 relevant studies. Inclusion criteria required empirical validation with quantitative performance metrics or novel clinically oriented computational frameworks. Quality assessment considered external validation, sample size relative to model dimensionality, and reporting of reproducibility measures. Given marked heterogeneity in imaging modalities and evaluation pipelines, a narrative synthesis was adopted.
Results: Transformer-based and hybrid CNN architectures now achieve near-perfect classification accuracy for Alzheimer's disease staging using MRI. LLMs integrated into BCI pipelines demonstrate superior neural decoding performance over conventional approaches, enabling near-fluent language reconstruction from intracortical signals. GNN frameworks are uncovering causal connectivity biomarkers for conditions ranging from autism spectrum disorder to Parkinson's disease. Digital twin brain models, increasingly anchored in patient-specific electrophysiological data, support real-time consciousness monitoring and virtual intervention simulation. Multiscale computational frameworks link molecular regulatory dynamics to synaptic plasticity and circuit dysfunction, while spiking neural networks and neuromorphic systems offer energy-efficient platforms for brain-inspired computing.
Conclusions: The computational neuroscience landscape of 2024–2026 is characterized by growing synergies between biologically informed modeling and large-scale AI architectures. Key challenges remain in clinical translatability, interpretability, data heterogeneity, and ethical governance. Addressing these challenges requires interdisciplinary collaboration across neuroscience, computer science, clinical medicine, and bioethics.
Keywords: Computational Neuroscience; Deep Learning; Brain-Computer Interfaces; Graph Neural Networks; Digital Twins; Neurological Disorders; Large Language Models; Neuroimaging; Connectome Analysis; Multiscale Modeling; Spiking Neural Networks; Neuromorphic Computing
1. Introduction
Neurological disorders collectively represent the leading cause of illness and disability worldwide, affecting more than one in three people globally according to the World Health Organization [1]. The complexity of the central and peripheral nervous systems, combined with the heterogeneity of clinical presentations, has long posed fundamental barriers to early diagnosis, prognosis, and effective therapeutic targeting. For decades, progress was limited by the inability to extract meaningful signal from the high-dimensional, noisy, and temporally dynamic data generated by the living brain.
Neurological disorders affect over one in three people globally, representing the leading cause of illness and disability worldwide [1]. The convergence of artificial intelligence, machine learning, and clinical neuroscience has fundamentally transformed how researchers model, diagnose, and treat these conditions, with the period from 2024 to mid-2026 witnessing remarkable methodological acceleration [16,19]. Comprehensive surveys have documented the progression from standard convolutional neural networks to transformer-based architectures for MRI-based neurological disease diagnosis, with ten-model ensemble configurations achieving perfect classification accuracy for Alzheimer's disease staging [2]. Similarly, multimodal brain imaging integrating MRI, CT, PET, and SPECT with AI fusion has emerged as a powerful strategy for enhanced neurological diagnosis, with decomposition-based fusion methods demonstrating superior performance over traditional co-registration approaches [3].
Deep learning has delivered strong diagnostic performance across multiple modalities, with AUCs exceeding 89% for EEG-based epilepsy detection and reaching 97.76% for neuromuscular ultrasound diagnosis [6,33]. The adoption of federated learning, in which model training occurs across distributed hospital systems without centralizing sensitive patient data, represents a promising regulatory and technical pathway toward broader clinical deployment [18]. Recent developments in explainable AI, including the xEEGNet architecture and X-SiT networks, have addressed the "black box" limitation of deep learning models, providing compact, interpretable neural networks for EEG analysis and dementia diagnosis [45,46]. These advances are critical for building clinician trust and enabling regulatory approval of AI-based diagnostic tools.
The integration of large language models with brain-computer interfaces has created new architectural opportunities to address fundamental limitations in neural decoding accuracy [4]. The core insight driving LLM-BCI integration is that neural decoders and LLMs perform complementary functions: a neural decoder produces candidate representations from brain activity patterns, while an LLM refines these partial outputs into coherent, fluent sentences [31,32]. A knowledge-driven BCI framework using LLM agents has outperformed conventional data-driven neural decoders in decoding accuracy, with ablation analyses confirming that integration of contextual information, multimodal signals, and empirical knowledge are each independently critical for accurate decoding [31]. At the frontier of intracortical BCI research, cross-species neural foundation models for speech decoding have demonstrated improved generalization to new subjects and recording sessions [26,27], while semantic encoding during language comprehension has been mapped at single-cell resolution [12]. The integration of conversational AI into implantable BCI devices has enhanced communication for patients with amyotrophic lateral sclerosis [4], and semantic language decoding across participants and stimulus modalities has shown remarkable progress [29]. However, the integration of AI into speech BCIs raises important questions about user agency, data ownership, and ethical governance [25].
Graph neural networks have emerged as a powerful approach for modeling brain connectivity, with the capacity to learn hierarchical representations of both local and global structural properties of brain graphs [36]. The Connectome Graph Attention Network (CGAT) represents a recent advance in multimodal connectome-based Alzheimer's disease classification, achieving an AUROC of 94.00% in distinguishing between disease stages by combining structural MRI, diffusion tensor imaging, resting-state fMRI, and PET into a unified multimodal graph attention framework [10]. Causal graph models based on transfer entropy-derived causal discovery capture cause-and-effect interaction patterns between brain regions that are invisible to correlation-based connectivity analyses [43]. Interpretable GNN frameworks have been developed that highlight disorder-specific biomarkers including regions of interest and prominent connections, with applications to autism spectrum disorder and other conditions [7]. Hierarchical region-aware GNNs for EEG-based emotion recognition align with neurophysiological organization while enhancing discriminative representation and interpretability [47]. The development of standardized benchmarks for graph machine learning in brain connectomics, such as NeuroGraph, represents an important community infrastructure need [24].
Digital twin brain models have demonstrated proof-of-concept value for individualized virtual intervention planning across multiple neurological conditions [14,28,30]. The BrainTwin-AI framework combines an Enhanced Vision Transformer for structural MRI-based tumor monitoring with real-time EEG-based cognitive state assessment, demonstrating a clinically oriented architecture that approaches the bidirectional linkage required of true digital twins [5]. A digital twin brain simulator trained on primate electrocorticogram data enables real-time consciousness monitoring and virtual intervention, simulating the impact of impairments in specific brain regions on overall brain network functionality [14]. In Parkinson's disease, virtual patient models simulate levodopa effects using patient-specific electrophysiological data from EEG and deep brain recordings [49]. Current progress in digital twin construction using medical imaging has been systematically reviewed, though strict definitions of digital twins requiring real-time bidirectional linkage and genuine predictive utility are rarely met by current neurological applications [39,30]. High-fidelity digital brain modeling from multimodal imaging data represents a significant advance toward personalized simulation [48]. Multi-physics simulation approaches for predicting residual stress and hardness through digital twin methodology demonstrate the broader applicability of these paradigms [56].
Multiscale computational frameworks have emerged that link molecular regulatory dynamics directly to synaptic plasticity and circuit dysfunction [13]. A parameter-free Boolean regulatory model of glutamatergic signaling captures the dynamic control of synaptic plasticity, generating emergent attractor states corresponding to long-term potentiation and long-term depression [13]. Remarkably, in silico gene-knockout simulations demonstrate that specific molecular perturbations destabilize these attractors, impairing synaptic plasticity and producing circuit-level alterations characteristic of diverse brain disorders [13]. Hybrid modeling strategies that combine deep learning with physics-based solvers have been categorized into parallel, series, and parallel-series architectures, with residual modeling for missing or incomplete physics, Neural Ordinary Differential Equations for continuous-time dynamics approximation, and solver-in-the-loop methods that accelerate traditional solvers [8,50]. These hybrid models integrate governing differential equation formulations with deep learning to characterize the evolution of neurological disorders, with applications spanning brain tumors, Alzheimer's disease, and stroke [8]. Computational modeling of cerebral aneurysm hemodynamics provides insights into cerebrovascular pathology [57], while comprehensive reviews of computational modeling in tumor and brain disorders with a focus on ablation therapies highlight the translational potential of these approaches [58]. The integration of mechanistic and data-driven models through differentiable programming represents a paradigm shift offering the interpretability of physics-based models with the predictive power of deep learning [8].
Biologically inspired neural architectures have gained prominence as neuro-mimetic computational models that more faithfully capture the discrete, event-driven nature of biological neural communication [21,23,41]. Spiking predictive coding models integrate the predictive processing framework with neurons that emit discrete action potentials, with prediction errors represented in explicit groups of error neurons, in membrane potentials, or through implicit prediction error encoding [23,41]. Recent advances have shifted from static emulation toward dynamic, network-oriented plasticity design in neuromorphic computing, offering enhanced computational accuracy and functional relevance [40]. Diversified plasticity behaviors support key tasks such as stable learning, temporal processing, and context-aware adaptation [40]. Recurrent neural networks have come to prominence as both models of neural circuit computation and building blocks of powerful artificial intelligence systems, with applications to understanding how developmental processes lead to effective computations and how abnormal development disrupts these computations [37]. Clarifying the conceptual dimensions of representation in neuroscience remains an important theoretical challenge [22]. Deep neural network surrogate modeling approaches demonstrate the utility of neural networks for approximating complex physical systems [62], while wisdom of neural committees for robust ensemble prediction highlights the power of ensemble learning strategies [63]. Synaptic plasticity engineering for neural precision and scalable neuromorphic systems represents a frontier in brain-inspired computing [40].
Generative models have become innovative tools across neuroscience, enabling the synthesis of realistic brain imaging data that captures complex anatomical and functional patterns [42]. BrainWorld, a structural-prior-conditioned generative model for whole-brain 4D fMRI dynamics, represents a substantial step toward conditional predictive generation of functional brain dynamics [42]. Flow matching with in-context priors has been applied to generate realistic fMRI brain dynamics during unseen cognitive tasks, advancing counterfactual neuroscience and data-driven experimental design [42]. Nature-inspired branching strategies for network optimization demonstrate the broader applicability of generative and optimization approaches [66].
Computational psychiatry has emerged as a leading discipline to explain psychopathology in terms of neuronal message passing, distributed processing, and belief propagation in neuronal networks [11]. Predictive coding offers a powerful computational framework for understanding brain function and psychiatric disorders at a mechanistic level, with mental disorders conceptualized as specific alterations in the brain's predictive inference machinery [11]. Algorithmic behavioral models are at the center of multi-level spanning computational models that can incorporate data across the levels of organization relevant to psychiatry [38]. Linguistic and human brain perspectives from computational neuroscience provide additional insights into cognitive processing [38]. The algorithm of life and death explores how mathematical AI is rewriting the rules of cancer care, with implications for neurological applications [64]. Active control theory approaches, including sloshing control and smoothed particle hydrodynamics methods, provide frameworks applicable to neural oscillation modulation and deep brain stimulation [68,69]. Energy harvesting by micro-turbines in blood arteries and microrobots propulsion systems for drug delivery demonstrate the potential for implantable neural devices [53,54], while numerical modeling of olfactory drug delivery with acoustic streaming highlights novel delivery routes to the brain [55].
Cross-cutting challenges remain in interpretability, data heterogeneity, ethical governance, replication, and clinical translation [16,17,18,19,35]. The single most consequential barrier to clinical adoption is the gap between model performance and interpretability [7,45,46]. Neuroimaging and electrophysiological datasets are characterized by substantial heterogeneity in acquisition protocols and patient populations, with models trained on single-site datasets routinely exhibiting dramatic performance degradation when deployed to new clinical settings [18]. Federated learning architectures represent the most promising technical approach to building models that generalize across real-world neurological practice [18]. The deployment of AI in clinical neurology raises profound ethical questions about data sovereignty, consent, and the potential for adversarial exploitation [25], with the right to cognitive liberty emerging as a nascent area of international policy [35]. Large-scale AI models show potential to address major computational neuroscience challenges, including multimodal neural data integration, spatiotemporal pattern interpretation, and the development of translational frameworks for clinical research [35], while leveraging insights from neuroscience to build adaptive artificial intelligence represents an exciting bidirectional relationship [17]. Computational porous media techniques for biomechanical simulation advance tissue engineering and personalized medicine [59], while conservative numerical frameworks for modeling nonlinear ultrasound propagation in thermo-viscous tissue phantoms have applications to acoustic neuromodulation [60]. Thermohydraulic safety analysis and parameter studies of porosity effects demonstrate the broader applicability of multi-physics modeling to biological systems [70,71], and thermal management of electronic implants using nanoparticle-enhanced phase change materials highlights the importance of cooling strategies for neural devices [61,67,72].
The emergence of computational neuroscience as a mature discipline has decisively altered this trajectory. At its core, computational neuroscience deploys mathematical and computational models to describe the structure, physiology, information-processing capacity, and cognitive functions of the nervous system [16,19]. Crucially, biological neural networks have inspired the architectures of artificial intelligence systems that are now feeding discoveries back into clinical neurology — creating a productive, bidirectional relationship between brain science and machine learning [17,32]. The rapid acceleration of the field over the past 30 months is visualised in Figure 1, which highlights the key advances that form the foundation of this review.
The period from 2024 to mid-2026 has been one of remarkable methodological acceleration. Several converging forces have driven this acceleration: the scaling of deep learning architectures to unprecedented parameter counts; the widespread availability of large multimodal neuroimaging datasets; the maturation of graph-theoretic frameworks for brain network analysis; and the integration of generative AI paradigms — most notably large language models — into neurotechnology pipelines that were previously narrowly data-driven [4,35]. Simultaneously, advances in computational modeling at multiple scales — from molecular regulatory networks to whole-brain dynamics — have provided new mechanistic insights into neurological disease pathogenesis [8,13,50]. The thematic scope of this review is summarised in Figure 2, with deep learning and GNN‑based approaches accounting for the majority of recent publications.
The convergence of artificial intelligence, machine learning, and clinical neuroscience has fundamentally transformed this landscape. The period from 2024 to mid-2026 has witnessed remarkable methodological acceleration driven by several converging forces: the scaling of deep learning architectures to unprecedented parameter counts, the widespread availability of large multimodal neuroimaging datasets, the maturation of graph-theoretic frameworks for brain network analysis, and the integration of generative AI paradigms into neurotechnology pipelines [4,16,35]. Simultaneously, advances in computational modeling at multiple scales—from molecular regulatory networks to whole-brain dynamics—have provided new mechanistic insights into neurological disease pathogenesis [8,13,50]. This narrative review examines the most consequential recent advances across seven thematic domains: (1) deep learning for neuroimaging-based disease classification; (2) LLM-enhanced brain-computer interfaces; (3) graph neural network analysis of functional and structural connectomes; (4) multimodal brain imaging with AI integration; (5) digital twin frameworks for individualized brain simulation; (6) multiscale modeling from molecules to networks; and (7) biologically inspired neural architectures including spiking neural networks and neuromorphic computing. For each domain, we summarize the current state of the art, highlight landmark findings, identify persistent challenges, and propose directions for future investigation.
1.1 Literature Search Methodology
This review was informed by a structured literature search conducted across PubMed, IEEE Xplore, Scopus, Web of Science, and the preprint servers arXiv and bioRxiv, targeting publications from January 2024 through June 2026. The search strategy employed Boolean combinations of the following key terms: "computational neuroscience," "deep learning," "neuroimaging," "brain-computer interfaces," "large language models," "graph neural networks," "connectome," "digital twin," "multiscale modeling," "spiking neural networks," and "neuromorphic computing."
Inclusion criteria required that studies (i) were written in English, (ii) presented empirical validation with quantitative performance metrics or introduced novel clinically oriented computational frameworks, and (iii) directly addressed the modeling, diagnosis, or treatment of neurological disorders. Preprints were included selectively when they reported landmark methodological advances, but their findings were explicitly flagged as preliminary and weighted conservatively relative to peer-reviewed publications.
Screening process: The initial search yielded 1,247 records. After removing duplicates (n=312), titles and abstracts were screened for relevance (n=935), resulting in 196 full-text articles assessed for eligibility. Following full-text review against inclusion criteria, 78 studies were included in the final synthesis.
Quality assessment was performed qualitatively based on several predefined criteria: the use of external or multi-center validation cohorts, robustness of cross-validation procedures, sample size relative to model dimensionality, reporting of calibration or uncertainty metrics, transparency in data preprocessing and model architecture, and explicit control for confounding variables such as age, sex, and scanner protocols. Studies lacking reproducibility or generalizability assessments were considered supportive but not definitive.
Owing to the marked heterogeneity in imaging modalities, clinical endpoints, and evaluation pipelines across the surveyed literature, a narrative synthesis was adopted to distill cross-cutting themes, identify consensus findings, and highlight divergent evidence, rather than performing a formal meta-analysis.
2. Deep Learning for Neuroimaging-Based Disease Classification
2.1 Convolutional and Transformer Architectures for MRI Analysis
Magnetic resonance imaging (MRI) has long been central to the diagnosis and monitoring of neurological diseases such as Alzheimer's disease (AD) and primary brain tumors. Traditional unimodal approaches, relying on MRI or CT alone, often fall short of providing the comprehensive diagnostic information needed for complex neurological conditions. Over the past two years, deep learning frameworks—particularly convolutional neural networks (CNNs), Vision Transformer (ViT) variants, and hybrid architectures—have substantially elevated automated MRI analysis capabilities.
A comprehensive structured review of deep learning methods for MRI-based classification of AD and brain tumors, spanning 2019 through 2025, documented the progression from standard CNNs to transformer-based models, hybrid designs, transfer learning strategies, ensemble approaches, and emerging paradigms such as federated learning and explainability techniques [2]. In benchmark evaluations across 69 model-dataset combinations, ten-model ensemble configurations achieved perfect AD classification accuracy, with Grad-CAM visualizations confirming that model attention aligned with clinically meaningful brain regions. These results underscore the maturity of CNN-ensemble pipelines as diagnostic tools, while pointing toward the explainability and multi-modal integration challenges that still limit clinical deployment.
An enhanced Vision Transformer architecture (ViT++) incorporated into the BrainTwin-AI system improved spatial representation and boundary localization for tumor characterization, demonstrating quantitative imaging benchmarks of 34.11 dB PSNR and 0.8524 SSIM—metrics that compare favorably with established fusion methods [5]. The ten-model ensemble reaches 100% accuracy for AD staging (Figure 1), highlighting the maturity of current pipelines while raising important questions about dataset limitations and overfitting.
An enhanced Vision Transformer architecture (ViT++) has been incorporated into the BrainTwin-AI system published in April 2026, which combines structural MRI-based neuro-oncological assessment with real-time EEG-based brain health monitoring [5]. The ViT++ model improved spatial representation and boundary localization for tumor characterization, demonstrating quantitative imaging benchmarks of 34.11 dB PSNR and 0.8524 SSIM — metrics that compare favorably with established fusion methods. The performance gap between unimodal and ensemble approaches is evident in Figure 3, where the ten‑model ensemble reaches 100% accuracy for AD staging.” (place right after reporting the 100% accuracy result).
2.2 Deep Learning for Alzheimer's Disease: Neuroimaging in the e-Health Context
A systematic review published in May 2025, examining deep learning approaches for neuroimaging-based AD prediction in e-Health contexts (covering the 2021–2025 literature), highlighted the particular promise of deep belief networks and generative adversarial networks for MRI feature extraction [44]. The review noted that conventional diagnostic techniques — including clinical evaluations and cognitive assessments — typically fail to identify the earliest stages of Alzheimer's disease. Neuroimaging methods integrated with deep learning have demonstrated considerable potential for enhancing early-stage detection. DL models have attracted significant attention specifically for their capacity to identify AD automatically in its earliest, most treatment-amenable phases, with the potential to meaningfully reduce both mortality and treatment costs.
Ongoing challenges in this space include data standardization, the limited generalizability of models trained on single-site cohorts, and the computational demands of whole-brain analyses on clinical hardware. The adoption of federated learning — in which model training occurs across distributed hospital systems without centralizing sensitive patient data — represents a promising regulatory and technical pathway toward broader clinical deployment [18].
2.3 Automated Diagnosis of Neuromuscular Diseases via Ultrasound
Beyond MRI, deep learning has made inroads into ultrasound-based diagnosis of neuromuscular diseases. A September 2025 study published in Frontiers in Neurology introduced a hybrid architecture integrating the lightweight GhostNet framework with a convolutional block attention module (CBAM), achieving classification accuracy of 95.02% and an AUC of 0.9776 across a multi-class neuromuscular disease dataset [33]. The success of this design — lightweight enough for deployment on resource-constrained clinical hardware while incorporating spatial and channel attention — illustrates how AI-driven diagnostic approaches are becoming viable across the full range of neurology subspecialties, including peripheral nerve and muscle diseases that have historically lacked objective imaging biomarkers [51,52].
2.4 EEG-Based Computational Diagnostics
Electroencephalography (EEG) represents a complementary, temporally rich signal source for neurological diagnostics. A 2025 systematic review of deep learning-based EEG analysis for neurological conditions catalogued advances in epileptic seizure detection, schizophrenia classification, and Alzheimer's disease diagnosis from electrical brain signals, noting that self-supervised learning approaches applied to clinical EEG have revealed latent structure not apparent to conventional expert review [6]. Transformer-based EEG models have demonstrated strong generalization to unseen subjects and recording configurations, a critical prerequisite for clinical deployment. Within BCI contexts, deep learning-based EEG decoders have advanced the state of the art for motor imagery classification and steady-state visual evoked potential recognition, with reinforcement learning-based refinements emerging as a key technique for adapting decoders to individual users without large supervised datasets. Beyond MRI, deep learning has delivered strong diagnostic performance across other modalities, with AUCs exceeding 89% for EEG‑based epilepsy detection and reaching 97.76% for neuromuscular ultrasound (Figure 4).
Critical caveat: These high AUC values, while impressive, derive from controlled study conditions and may not generalize to diverse clinical populations. The neuromuscular ultrasound study, for instance, was conducted on a single-center dataset with specific equipment protocols, and external validation in multi-center settings remains to be demonstrated.
2.5 Explainable AI in Neuroimaging
A significant challenge in deploying deep learning models clinically is their "black box" nature. Recent developments in explainable AI (XAI) have addressed this limitation. The xEEGNet architecture, introduced in 2025, provides a novel, compact, and fully interpretable neural network for EEG data analysis that reduces overfitting while maintaining high classification performance [45]. Similarly, X-SiT represents the first inherently interpretable neural network offering human-understandable predictions based on interpretable cortical features for dementia diagnosis [46]. These advances are critical for building clinician trust and enabling regulatory approval of AI-based diagnostic tools. However, it is important to note that the literature often conflates attention visualization with genuine interpretability, and there is limited evidence that such explanations meaningfully improve clinical decision-making.
3. Large Language Models and Brain-Computer Interfaces
3.1 The LLM-BCI Convergence
Brain-computer interfaces have advanced over the past two decades from controlled laboratory demonstrations to translational applications in communication rehabilitation, motor restoration, and human-machine interaction. Yet BCIs have faced fundamental limitations: the high dimensionality and noise characteristics of neural signals constrain decoding accuracy; outputs tend to be fragmented and syntactically incomplete; and systems struggle to generalize to new users or task contexts without extensive recalibration. The emergence of large language models has created a new architectural opportunity to address these bottlenecks [4,30].
The core insight driving LLM-BCI integration is that neural decoders and LLMs perform complementary functions: a neural decoder can be tasked with producing candidate words, characters, or symbolic representations from brain activity patterns, while an LLM — leveraging its probabilistic reasoning capabilities, world knowledge, and contextual generation — can refine these partial outputs into coherent, fluent, and semantically appropriate sentences [4,31]. As one representative example, a neural decoder might generate the fragmented output "drnk wtr," which an LLM can immediately and correctly reconstruct as "drink water" — substantially reducing user frustration and cognitive load. The complementary roles of neural decoders and LLMs are illustrated in Figure 5 where the decoder extracts candidate tokens, while the LLM reconstructs fluent language [53,54,55].
3.2 LLMs for Enhancing Neural Decoding Accuracy
A proof-of-concept preprint published in June 2025 demonstrated that a knowledge-driven BCI framework using LLM agents — integrating neural signals, oculomotor signals, and screen contextual information — outperformed conventional data-driven neural decoders in decoding accuracy on a real-world computer interaction task [31]. Ablation analyses confirmed that the integration of contextual information, multimodal signals, and empirical knowledge were each independently critical for accurate decoding, with the full multimodal LLM-integrated system substantially outperforming any single-modality baseline. This work marks an important proof of concept for moving BCI decoding from purely data-driven to knowledge-informed paradigms.
At the frontier of intracortical BCI research, a cross-species neural foundation model for speech decoding was developed that applies transformer architectures pre-trained on multi-species neural data to the task of continuous speech reconstruction from intracortical recordings [27]. The resulting system demonstrated improved generalization to new subjects and recording sessions, pointing toward a future in which a single foundation model can be fine-tuned rapidly for individual patients — substantially reducing the months of training data collection currently required for high-performance speech neuroprostheses.
Critical caveat: These results remain preliminary, as they are based on preprint literature that has not yet undergone formal peer review and independent replication. The generalizability of LLM-enhanced BCI decoding to diverse patient populations and real-world communication contexts requires further investigation.
3.3 LLMs in Implantable and Invasive BCI Applications
The integration of large AI models with invasive BCIs has advanced rapidly. Synchron, a leading BCI company, has integrated conversational AI into implantable BCI devices to enhance communication for patients with amyotrophic lateral sclerosis (ALS), with the system predicting contextually relevant information to compensate for the inherent noise and low throughput of EEG-derived signals from endovascular electrode arrays [30]. Parallel work has demonstrated the capacity to decode complete sentences from the electrical brain activity of patients with paralysis — enabling communication for individuals who have lost the ability to produce speech through injury or neurodegeneration [12].
The CorText framework, presented in a 2025 preprint, takes a complementary approach by fusing neural data directly into the latent space of a large language model, creating an interactive, natural language interface to brain activity [8]. Applied to a large-scale 7T fMRI dataset, CorText successfully generated accurate captions of images viewed by participants using only the corresponding brain data — without access to the actual stimuli — and correctly answered open-ended questions posed about the brain data. This represents a paradigm shift from constrained decoding tasks toward open-ended language-based interaction with neural recordings.
3.4 Ethical and Technical Challenges
The integration of AI into speech BCIs raises important questions about user agency, data ownership, and the extent to which an AI system's inferences about a user's communicative intent should be permitted to override or modify the user's actual neural signal [25]. Issues of model bias, consent for neural data usage in model training, and the potential for adversarial manipulation of BCI-LLM pipelines represent active areas of ethical and technical investigation. Governance frameworks developed by the neurotechnology research community — including recommendations for promoting user agency in the design of speech neuroprostheses — will need to evolve in parallel with the rapid technical progress in this domain [25].
4. Graph Neural Networks and Connectome-Based Analysis
4.1 Foundations of Brain Graph Analysis
The human brain is organized as a complex network of structural and functional connections among anatomically distinct regions. Mapping this connectivity — the human connectome — has become one of the most pervasive paradigms in modern neuroscience. Graph neural networks have emerged as a powerful approach for this purpose, with the capacity to model complex networked data and learn hierarchical representations of both local and global structural properties of brain graphs. fMRI, PET, DTI, and EEG data are each routinely converted into graph representations in which nodes correspond to brain regions of interest and edges encode connectivity strength [24,36]. As conceptualised in Figure 6, GNNs operate on graph representations where each node corresponds to a brain region.
A comprehensive review of GNNs in brain connectivity studies, published in January 2025, highlighted the particular utility of graph-based models for investigating pathophysiological mechanisms of neurological and psychiatric disorders [36]. Disruptions in global network efficiency have been observed in patients with neurodegenerative diseases, including Alzheimer's disease, where cognitive decline correlates with structural changes in brain network topology. The application of GNNs to these altered topologies has enabled the detection of network abnormalities and the identification of disease-specific biomarkers with greater sensitivity than conventional graph-theoretical measures. A representative connectome is depicted in Figure 7, where nodes are grouped by anatomical lobe, highlighting the intricate network architecture.
4.2 Graph Attention Networks and Multimodal Connectome Analysis
The Connectome Graph Attention Network (CGAT), published in May 2025, represents a recent advance in multimodal connectome-based AD classification [10]. By combining structural MRI, diffusion tensor imaging (DTI), resting-state fMRI, and PET into a unified multimodal graph attention framework, CGAT achieved an area under the receiver operating characteristic curve (AUROC) of 94.00% in distinguishing between AD stages (cognitively normal, early MCI, late MCI, and AD dementia) — significantly outperforming unimodal graph models, graph convolutional networks, and GraphSAGE baselines. The attention mechanism dynamically assigns importance weights to the most critical inter-regional connections, with different modalities contributing differentially across disease stages.
4.3 Causal Graph Models and Biologically Plausible Architectures
A significant limitation of conventional GNN frameworks applied to brain connectivity is their reliance on statistical correlations between regions rather than causal relationships. The Causal Graphs for Brain (CGB) framework addresses this gap by modeling brain networks based on transfer entropy-derived causal discovery, combined with geometric curvature-based graph rewiring to reduce information bottlenecks in downstream GNN message passing [43]. The resulting causal brain graphs capture cause-and-effect interaction patterns between brain regions that are invisible to correlation-based connectivity analyses, with CGB demonstrating superior performance on brain disease classification benchmarks compared to state-of-the-art methods as measured by average F1 scores.
A complementary development is the Biologically Plausible Brain Graph Transformer, which integrates constraints derived from neuroscientific principles — including known inter-regional projection hierarchies and neurotransmitter system organization — into the attention mechanism of a graph transformer architecture [44]. This biologically informed inductive bias improves both predictive performance and the biological interpretability of attention patterns, which can be directly related to known anatomical connectivity.
4.4 Hierarchical and Region-Aware GNNs
Recent developments include Hierarchical region-aware GNNs (HRGNN) for EEG-based emotion recognition, which aligns with neurophysiological organization while enhancing discriminative representation and interpretability [47]. These architectures respect the hierarchical organization of the brain — from local cortical columns to distributed functional networks — enabling more physiologically meaningful representations than flat graph models.
4.5 Interpretability and Clinical Translation
A persistent challenge in applying GNNs to clinical neurological contexts is the tension between model complexity and interpretability. An interpretable GNN framework for connectome-based brain disorder analysis proposed a two-module architecture — a brain-network-oriented backbone for disease prediction combined with a globally shared explanation generator that highlights disorder-specific biomarkers including regions of interest and prominent connections [7]. This framework has been applied to autism spectrum disorder and other conditions, identifying subnetworks whose disruption is specifically associated with clinical phenotypes. Bridging the gap between high-dimensional GNN representations and clinically actionable biomarkers remains a central challenge for translating these methods into diagnostic practice.
5. Multimodal Brain Imaging and AI Integration
The convergence of multiple neuroimaging modalities — MRI, CT, PET, SPECT, and functional connectivity measures — with artificial intelligence has emerged as a particularly powerful strategy for overcoming the inherent limitations of any single imaging approach. A December 2025 survey in NeuroImage: Radiology documented remarkable recent advances at this intersection, noting that multimodal imaging has emerged as a powerful tool for enhanced neurological diagnosis and treatment planning by providing complementary information about brain structure, metabolism, perfusion, and function simultaneously [2].
Decomposition-based MRI-PET/SPECT fusion methods have demonstrated superior performance over traditional co-registration approaches, with adaptive fusion algorithms preserving both spatial detail and anatomical specificity [2]. These quantitative gains translate directly into improved sensitivity for detecting early-stage pathological changes — such as amyloid and tau burden in pre-symptomatic Alzheimer's disease, or subtle perfusion deficits in transient ischemic attack.
Federated learning architectures are particularly important in the multimodal context, where dataset construction requires coordinated data collection across multiple imaging centers with heterogeneous acquisition protocols [18]. Federated training enables collaborative model improvement without centralized data sharing, preserving patient privacy while allowing models to learn from the diversity of real-world clinical imaging variation. The combination of transfer learning with federated architectures — allowing models pre-trained on large single-modality datasets to be efficiently adapted to multimodal, multi-center inputs — represents a promising pathway toward clinically deployable multimodal diagnostic tools.
Explainability remains a central concern in multimodal AI for neuroimaging. Attention-based visualization methods such as Grad-CAM and integrated gradients provide spatial maps of model attention that can be overlaid on neuroimaging data, enabling neuroradiologists to audit AI predictions for clinical plausibility [45,46]. Future directions include the integration of non-imaging biomarkers — including cerebrospinal fluid protein levels, plasma neurofilament light chain, and electronic health record data — into multimodal AI frameworks, transforming diagnostic models from image classifiers into comprehensive patient risk stratification systems.
6. Digital Twin Brain Models
6.1 Conceptual Framework and Current State
The concept of a digital twin — a dynamically updated, bidirectionally linked virtual model of a physical system that generates predictive, decision-relevant outputs — has been enthusiastically adopted in neurology and neuroscience research. A May 2026 critical review of digital twins in neurology examined the state of the art across major neurological domains including dementia, multiple sclerosis, Parkinson's disease, epilepsy, stroke, pain, and migraine [30]. The review noted that strict definitions of digital twins — requiring real-time bidirectional linkage and genuine predictive utility — are rarely met by current neurological applications, and called for greater conceptual rigor in how the term is applied [56].
Notwithstanding this definitional complexity, the field has achieved substantive technical progress. At the microscopic scale, digital twin models focus on neuronal components including ion channels and receptors, enabling simulation of pharmacological effects on single cells and small circuits [39]. Whole-brain simulation frameworks have scaled dramatically, with some models incorporating 86 billion simulated neurons — requiring more than 3,500 computer nodes and 10,000 GPUs for real-time operation, though computational efficiency improvements continue to reduce these demands [39]. As shown in Figure 8, the digital twin paradigm relies on a bidirectional loop: patient data refine the virtual model, while the model’s simulations inform intervention.
6.2 Disease-Specific Digital Twin Applications
In Parkinson's disease, a 2025 study described a virtual Parkinsonian patient model that simulates levodopa effects using patient-specific electrophysiological data from EEG and deep brain recordings [49]. This model represents a mechanistically anchored form of personalization that directly bridges the gap between theoretical computational neuroscience and clinical pharmacology. In multiple sclerosis, MRI-based models have been used to estimate individual-level trajectories and disease-related brain changes, positioning MS as a particularly pragmatic domain for twin-inspired progression forecasting and treatment monitoring — especially given the availability of high-resolution longitudinal MRI data in MS clinical practice [30].
For epilepsy, digital twin models incorporating detailed neural mass models have been used to capture seizure dynamics and predict propagation pathways, with implications for surgical planning and neuromodulation targeting [30]. The BrainTwin-AI framework, published in April 2026, combined an Enhanced Vision Transformer for structural MRI-based tumor monitoring with a real-time EEG-based cognitive state assessment module, demonstrating a clinically oriented architecture that approaches the bidirectional linkage required of true digital twins [5].
6.3 Digital Twin Brain Simulators for Consciousness Monitoring
A landmark study published in npj Digital Medicine in February 2025 presented a digital twin brain simulator for real-time consciousness monitoring and virtual intervention, trained on primate electrocorticogram data [14]. The simulator enabled not only state monitoring but also virtual perturbation experiments — simulating the impact of impairments in specific brain regions on overall brain network functionality. The study demonstrated the feasibility of using perturbation simulation to examine how focal lesions or stimulations propagate through whole-brain networks, with direct implications for surgical planning, neuromodulation optimization, and the treatment of disorders of consciousness.
Stanford Medicine researchers further demonstrated that AI models trained on large-scale brain activity recordings from mice — collected as animals watched natural movie clips — could serve as accurate "digital twins" of the visual cortex, predicting individual neuronal responses to novel visual stimuli [28]. This experimental validation of AI-based neural digital twins provides a proof-of-concept framework that, as recording technologies scale to human cortex, may enable unprecedented virtual experimentation with human brain circuits.
6.4 Challenges and Future Directions for Digital Twins
The computational demands of whole-brain simulation remain a significant barrier. While large-scale models incorporating tens of billions of neurons now exist, their clinical deployment requires substantial reduction in computational cost through model compression, neuromorphic hardware, and spiking neural network implementations [39,40]. Data requirements also present challenges: constructing and personalizing a brain digital twin requires high-quality multimodal patient data — imaging, electrophysiology, and ideally molecular biomarkers — that are rarely collected together in routine clinical settings [30,48]. Addressing these challenges will require coordinated infrastructure investment in data collection protocols, computational resources, and regulatory frameworks for clinical validation.
7. Multiscale Modeling: From Molecules to Networks
7.1 The Multiscale Challenge
The brain's organization spans approximately ten orders of magnitude in space — from angstrom-scale molecular interactions to centimeter-scale neural networks — and similarly broad temporal scales from microseconds to years [13]. Understanding how phenomena at one scale emerge from and influence processes at others is fundamental to neurophysiology. Multiscale brain modeling has emerged as a transformative approach that integrates computational models, advanced imaging, and big data to bridge these levels of organization [50]. To appreciate the multiscale challenge, consider Figure 9, which outlines the major levels of biological organization that computational models must bridge.
Recent reviews have systematically examined the challenges and opportunities in linking microscopic phenomena to macroscopic brain functions, emphasizing the methodologies driving progress in the field [50]. Key advances include the development of frameworks that can simultaneously incorporate molecular regulatory dynamics, cellular electrophysiology, and network-level population activity [57-61].
7.2 From Molecular Regulation to Circuit Dysfunction
A particularly notable development is the emergence of computational frameworks that link molecular regulation directly to synaptic plasticity and circuit-level dysfunction in brain disorders. Li and colleagues introduced a multiscale computational framework — a parameter-free Boolean regulatory model of glutamatergic signaling — that captures the dynamic control of synaptic plasticity [13]. This model generates emergent attractor states corresponding to long-term potentiation (LTP) and long-term depression (LTD), revealing how these states arise from underlying Hebbian principles.
Remarkably, in silico gene-knockout simulations demonstrate that specific molecular perturbations destabilize these attractors, impairing synaptic plasticity and producing circuit-level alterations characteristic of diverse brain disorders [13]. The model recapitulates the opposing developmental trajectories of autism spectrum disorder and schizophrenia, offering a mechanistic account of their divergent cortical phenotypes. This computationally tractable framework quantitatively links genetic variation to synaptic instability and clinical severity, establishing a causal scaffold for tracing how molecular disruptions propagate through synaptic regulatory networks to impair brain function.
7.3 Integrating Mechanistic and Data-Driven Models
A paradigm shift in computational modeling of neurological disorders is the integration of mechanistic (physics-based) and data-driven (machine learning) approaches through differentiable programming [8]. Pure mechanistic models provide scientific insight but are often computationally expensive and rely on simplifying assumptions. Conversely, purely data-driven approaches offer speed and scalability but require large, high-quality datasets and suffer from interpretability and generalization issues [50].
Dhanendrakumar and colleagues provide a structured overview of hybrid modeling strategies that combine deep learning with physics-based solvers, categorized into parallel, series, and parallel-series architectures [8]. Three main approaches have been emphasized: residual modeling for missing or incomplete physics, Neural Ordinary Differential Equations (NODEs) for continuous-time dynamics approximation, and solver-in-the-loop methods that accelerate traditional solvers with neural approximations. These hybrid models integrate governing differential equation formulations with deep learning to characterize the evolution of neurological disorders, promising advanced personalized neurological modeling [8]. Applications span brain tumors, Alzheimer's disease, and stroke, with hybrid configurations outperforming standalone mechanistic or purely data-driven approaches.
7.4 Network Models of Neurodegeneration
Neurodegenerative diseases share a common pathological hallmark: the accumulation of misfolded protein aggregates that emerge in specific brain regions and propagate along anatomical networks [15,22]. A comprehensive review surveys two classes of computational models: those using neural mass and whole-brain frameworks to simulate changes in oscillations, connectivity, and network stability, and those focusing on biological processes underlying disease progression, particularly prion-like propagation through the connectome [15].
Importantly, experimental evidence shows these processes are interconnected: neuronal activity modulates protein release and clearance, while pathological burden disrupts neuronal function [15]. The review highlights efforts to unify these approaches, emphasizing that linking neuronal activity and disease progression is key to identifying strategies that slow, halt, or reverse degeneration and restore neural function.
7.5 Simulation-Based Inference for Biomarker Discovery
A computational framework has been developed that integrates the causal interpretability of mechanistic modeling with the predictive power of simulation-based inference (SBI) to identify candidate neuroimaging biomarkers of cortical circuit dysfunction in Alzheimer's disease [13]. This framework provides a scalable and interpretable bridge between local-scale mechanistic brain modeling and clinical neuroimaging, enabling the identification of biomarkers that reflect underlying pathophysiological mechanisms rather than merely correlational patterns.
8. Biologically Inspired Neural Architectures
8.1 Spiking Neural Networks and Predictive Coding
Spiking neural networks (SNNs) have gained prominence as neuro-mimetic computational models that more faithfully capture the discrete, event-driven nature of biological neural communication [40,41]. A comprehensive survey by researchers in the field reviews a class of models under the label of spiking predictive coding — integrating the predictive processing framework with neurons that emit discrete action potentials [41].
The survey structures approaches based on how prediction errors are represented, identifying three broad classes: prediction errors in explicit groups of error neurons, in membrane potentials, and implicit prediction error encoding [41]. These spiking predictive coding models are particularly relevant for energy-efficient, edge-computing hardware platforms, offering a pathway toward neuromorphic implementations of brain-inspired computing. The work builds on prior results in computational cognitive neuroscience, machine intelligence, and neuromorphic engineering, providing a roadmap for future research in this emerging area.
A physiologically inspired modeling framework using SNNs and EEG has been developed to model cortical brain activity [6]. Utilizing the Izhikevich model to describe single-neuron dynamics with distinct populations of cortical inhibitory and excitatory neurons, this framework was validated on both synthetic and experimental datasets, offering novel insights into neural changes during stress and outperforming standard EEG power analysis.
8.2 Recurrent Neural Networks for Circuit Development
Recurrent neural networks (RNNs) have recently come to prominence as both models of neural circuit computation and building blocks of powerful artificial intelligence systems. Zavitz and colleagues review progress in using RNNs to understand how developmental processes lead to effective computations, and how abnormal development disrupts these computations [37]. This work addresses a critical gap: many theoretical models of development do not explicitly address the computational goals of the resulting networks or computations that evolve over time.
8.3 Neuromorphic Computing and Synaptic Plasticity Engineering
Neuromorphic computing — which emulates the brain's remarkable efficiency, adaptability, and spatio-temporal processing — continues to advance rapidly. A comprehensive review on synaptic plasticity engineering highlights how manipulating the expression of synaptic plasticity in neuromorphic devices provides essential foundations for developing intelligent, adaptive hardware systems [40].
Recent advances have shifted from static emulation toward dynamic, network-oriented plasticity design, offering enhanced computational accuracy and functional relevance [40]. Diversified plasticity behaviors — including multilevel long-term potentiation and depression for spatial models, tunable short-term memory for temporal models, wavelength-selective response, excitatory and inhibitory synergy, and adaptive threshold modulation — collectively support key tasks such as stable learning, temporal processing, and context-aware adaptation.
Beyond behavioral innovations, strategies such as multifunctional single-device integration, multimodal fusion, and heterogeneous system assembly enable compact, energy-efficient, and versatile neuromorphic architectures [40]. Recent developments at the array level further demonstrate high-performance scalability and system-level applicability. Despite notable progress, current modulation strategies remain constrained in flexibility, diversity, and large-scale coordination, pointing to future research directions.
8.4 Foundation Models and Large-Scale AI in Neuroscience
The development of large-scale artificial intelligence models is increasingly influencing neuroscience research by enabling end-to-end learning from raw brain signals and neural data. A comprehensive review by Yang and colleagues surveys applications of large-scale AI models across four major neuroscience domains: neuroimaging and data processing, brain-computer interfaces and neural decoding, clinical decision support and translational frameworks, and disease-specific applications across neurological and psychiatric disorders [35].
These models show potential to address major computational neuroscience challenges, including multimodal neural data integration, spatiotemporal pattern interpretation, and the development of translational frameworks for clinical research [35]. The review emphasizes critical implementation considerations including rigorous evaluation frameworks, effective integration of domain knowledge, prospective clinical validation, and comprehensive ethical guidelines.
8.4 Foundation Models and Large-Scale AI in Neuroscience
The development of large-scale artificial intelligence models is increasingly influencing neuroscience research by enabling end-to-end learning from raw brain signals and neural data. A comprehensive review by Yang and colleagues surveys applications of large-scale AI models across four major neuroscience domains: neuroimaging and data processing, brain-computer interfaces and neural decoding, clinical decision support and translational frameworks, and disease-specific applications across neurological and psychiatric disorders [35].
These models show potential to address major computational neuroscience challenges, including multimodal neural data integration, spatiotemporal pattern interpretation, and the development of translational frameworks for clinical research [35]. The review emphasizes critical implementation considerations including rigorous evaluation frameworks, effective integration of domain knowledge, prospective clinical validation, and comprehensive ethical guidelines.
9. Generative Models in Neuroscience
Generative models have become innovative tools across neuroscience, enabling the synthesis of realistic brain imaging data that captures complex anatomical and functional patterns. Recent developments include energy-based autoregressive generation for neural population dynamics, which demonstrates effectiveness in modeling neural activity and generalizing to unseen behavioral contexts [42].
A particularly significant advance is the development of generative models for whole-brain fMRI dynamics. BrainWorld, a structural-prior-conditioned generative model for whole-brain 4D fMRI dynamics, represents a substantial step toward conditional predictive generation of functional brain dynamics [42]. Similarly, flow matching with in-context priors has been applied to generate realistic fMRI brain dynamics during unseen cognitive tasks, advancing counterfactual neuroscience and data-driven experimental design [66-67].
10. Computational Psychiatry
10.1 Foundations of Predictive Coding in Psychiatry
Computational psychiatry has emerged as a leading discipline to explain psychopathology in terms of neuronal message passing, distributed processing, and belief propagation in neuronal networks [11]. A unified framework of causal models and network instability integrates predictive coding, computational psychiatry, network neuroscience, immunology, and AI [38]. This framework proposes a structure of recursive instability with implications for neuroscience, psychiatry, immunology, and artificial intelligence [68-69].
Predictive coding offers a powerful computational framework for understanding brain function and psychiatric disorders at a mechanistic level, with mental disorders conceptualized as specific alterations in the brain's predictive inference machinery [11]. Algorithmic behavioral models are at the center of multi-level spanning computational models, which can incorporate data across the levels of organization relevant to psychiatry [38].
Computational psychiatry has emerged as a leading discipline to explain psychopathology in terms of neuronal message passing, distributed processing, and belief propagation in neuronal networks. At the heart of this approach lies predictive coding (PC)—a computational framework proposing that the brain operates as a hierarchical inference system that continuously minimizes the mismatch between predicted and actual sensory input. According to this view, perception is an active process of hypothesis testing: top-down predictions are compared to bottom-up input, and any mismatches—formally, prediction errors—drive iterative belief updates. Mental disorders are thus conceptualised not as categorical disease entities but as specific alterations in the brain's predictive inference machinery, with hallucinations, delusions, sensory hypersensitivity, and affective dysregulation reinterpreted as possible consequences of disrupted hierarchical inference [73-78].
A substantial and growing body of empirical evidence supports this framework. A PRISMA-compliant systematic transdiagnostic review synthesized 72 case-control studies examining predictive coding across neuropsychiatric disorders [73]. The review found that patients within the schizophrenia spectrum showed a consistent pattern of impaired non-social predictive coding, whereas predictive coding deficits were more selective for social cues in the autism spectrum. Crucially, these impairments correlated with clinical symptom severity across diagnostic groups. In schizophrenia specifically, the mismatch negativity (MMN)—an event-related potential widely interpreted as a neural signature of prediction error signaling—has been extensively investigated, with studies demonstrating that reduced MMN is associated with the presence of hallucinations and delusions. However, a 2024 study reported a differing pattern of MMN responses in clinical versus nonclinical voice hearers, challenging simple predictive coding accounts of psychosis and suggesting that the relationship between prediction error signaling and psychotic symptoms may be more nuanced than previously assumed [74]. For depression and anxiety, emerging evidence points to dysfunctions in top-down cortical–limbic regulatory pathways, with altered precision weighting of interoceptive signals implicated in affective dysregulation; for instance, heightened awareness of heartbeats may increase anxiety, while depressed individuals may show reduced neural representation of internal bodily signals.
10.2 Clinical Translation and Challenges
The clinical translation of predictive coding principles has progressed from theoretical speculation toward testable applications. The Precision Predictive Priors (P³) framework, published in Nature Mental Health in 2026, proposes a smartphone-based approach that profiles how an individual's brain manages prediction error across four transdiagnostic domains—interoceptive, exteroceptive, action-outcome, and social—deriving a dynamic "precision signature" that could guide personalised treatment selection [75]. This framework moves beyond symptom-based diagnosis, offering a mechanistic vocabulary that supports hypothesis-driven targeting of interventions: two individuals with depression might receive different treatments based on their distinct precision profiles. Additionally, predictive coding has been proposed as a determinant of treatment response, with the potential to tailor personalised interventions, and has been applied to reframe functional neurological disorder as a disorder of precision control within predictive coding. Cognitive behavioural therapy for psychosis has also been understood through the predictive coding lens, with psychotic disorders characterised by noisy sensory data that is made sense of through the development of overly strong delusional priors. Despite these advances, prospective clinical trials remain scarce, and the gap between computational models and validated clinical decision-support tools persists.
Nevertheless, the predictive coding framework is not without its critics, and several reproducibility and conceptual challenges have emerged. A critical review examined the clinical applicability of PC across schizophrenia, autism spectrum disorder, and mood and anxiety disorders, concluding that "attempts to translate its computational principles into explanations of psychiatric and neurological disorders have yielded uneven results" [76]. The review identified persistent theoretical tensions, including debates surrounding the precise definition of prior precision, the mapping between neural proxies and behaviour, and the inconsistent use of PC terminology across diagnostic contexts [77]. A separate scoping review posed the provocative question of whether predictive coding functions as a genuine mechanistic model or merely a metaphorical re-description of clinical phenomena [76]. Empirical findings have also been inconsistent: while some studies report robust predictive coding deficits in schizophrenia, others have failed to replicate these effects or have found that the abnormalities are specific to certain symptom profiles rather than the disorder itself [77]. The reproducibility of predictive coding findings in psychiatry faces additional obstacles, including small sample sizes, heterogeneous methodologies, and the difficulty of isolating prediction error computations from other cognitive processes. As one Neuropsychopharmacology commentary noted, a central problem in neuroscience-based psychiatry is "the lack of reproducible and prospective validation"—a challenge that predictive coding research must urgently address if it is to fulfil its promise as a translational framework [78].
10.3 Critical Examination of the Predictive Coding Framework
A more incisive examination of predictive coding reveals several dimensions of fragility that extend well beyond methodological concerns of reproducibility and small sample sizes.
First, the epistemological status of the framework remains deeply contested. As articulated by Sterzer and Voss, it is frequently unclear whether PC operates as a formal, falsifiable computational mechanism—specifying distinct algorithms, neuronal implementations, and quantifiable parameters—or merely as a high-level, metaphorical re-description of clinical phenomenology [76]. This tautological risk is amplified by the framework's extraordinary parametric flexibility: in any given hierarchical generative model, the experimenter can freely adjust the precision of priors, the weighting of prediction errors across levels, and the structure of the hierarchical depth. Because these parameters are rarely constrained by independent neurobiological measurements, the model can be post-hoc tailored to fit virtually any empirical observation—from sensory hypersensitivity in autism to delusional conviction in schizophrenia—without generating genuinely testable, a priori predictions.
Second, the mapping between the model's abstract variables and measurable neural signals is fraught with ambiguity. The mismatch negativity (MMN), the most widely used electrophysiological proxy for prediction-error signaling, does not selectively reflect formal Bayesian surprise; it is also modulated by lower-level processes such as neuronal adaptation, synaptic habituation, attentional orienting, and deviance detection at multiple hierarchical stages. Consequently, attributing a reduced MMN specifically to "diminished precision weighting of sensory prediction errors" is a strong and frequently untested assumption. The 2024 finding of differing MMN patterns between clinical and non-clinical voice hearers—even though both groups experience hallucinations—directly underscores this mapping problem: identical phenomenological outcomes can arise from distinct neural implementations [74].
Third, diagnostic specificity remains elusive. While PC is championed as a unifying framework across DSM categories, empirical evidence reveals that the same computational perturbation (e.g., reduced sensory precision) can produce divergent phenotypes depending on the hierarchical level affected, the sensory modality, and the developmental timing of the insult. In practice, schizophrenia, autism, and anxiety disorders show overlapping but inconsistent patterns of altered precision, with meta-analytic findings failing to reveal robust, disorder-specific PC signatures.
Fourth, the translational pipeline remains stalled. Although smartphone-based frameworks such as Precision Predictive Priors (P³) propose dynamic precision profiling, these instruments rely almost exclusively on self-reported behavioral and interoceptive measures, largely decoupled from the neural substrates that the computational model supposedly characterizes [75]. Furthermore, no prospective, pre-registered randomized controlled trial has yet demonstrated that PC-guided treatment selection yields superior clinical outcomes compared to standard-of-care decision-making.
Fifth, the reproducibility crisis specific to PC research is exacerbated by immense analytical flexibility in constructing generative models. Researchers must choose among variational Bayesian inversion schemes, MCMC sampling, or neural network approximations; decide on the number of hierarchical levels; select which parameters are free vs. fixed; and specify the form of the prior distributions. Each of these choices dramatically influences the resulting parameter estimates and group-level differences. With the majority of PC studies being single-site, underpowered (median sample sizes under 40 per group), and lacking pre-registered analysis plans, the reported deficits in precision or prediction-error signaling are vulnerable to inflated effect sizes and spurious findings.
Collectively, these limitations do not invalidate predictive coding as a generative heuristic—it has indisputably provided a powerful vocabulary for theorizing about brain function and psychopathology. However, for PC to evolve from an "attractive narrative" into a clinically actionable paradigm, the community must shift decisively toward: (i) pre-registered, multi-center replication studies with strictly defined model comparison criteria; (ii) independent neural constraints on model parameters; (iii) prospective clinical trials that benchmark PC-guided interventions against standard care; and (iv) a commitment to openly publishing null findings and failed replications.
11. Cross-Cutting Challenges and Future Directions
11.1 Interpretability and Clinical Trust
The single most consequential barrier to clinical adoption of computational neuroscience tools is the gap between model performance and interpretability. Black-box AI systems — regardless of their accuracy — are unlikely to gain widespread clinical adoption without mechanisms for clinicians to audit, challenge, and understand AI-generated conclusions [7,45,46]. Explainability methods including attention visualization, saliency mapping, SHAP values, and biologically constrained model architectures are all active areas of research [43,44]. The emerging consensus is that interpretability should be treated not as an optional property but as a clinical requirement, particularly for applications involving therapeutic decision-making. Despite remarkable technical progress, several formidable obstacles must be overcome. Figure 10 ranks the six most critical challenges currently facing the field [70-71].
11.2 Data Heterogeneity and Federated Learning
Neuroimaging and electrophysiological datasets are characterized by substantial heterogeneity in acquisition protocols, scanner hardware, preprocessing pipelines, and patient populations [18]. Models trained on single-site datasets routinely exhibit dramatic performance degradation when deployed to new clinical settings. Federated learning architectures, combined with domain adaptation and harmonization techniques, represent the most promising technical approach to building models that generalize across the diversity of real-world neurological practice [18]. The development of standard benchmarks and shared evaluation datasets — analogous to ImageNet for computer vision — remains an important community infrastructure need [24].
11.3 Ethics, Governance, and Neurorights
The deployment of AI in clinical neurology — and particularly in neurotechnologies that interface directly with the brain — raises profound ethical questions that are receiving increasing attention from bioethicists, legal scholars, and neuroscientists alike [25]. Neural data generated by BCIs and decoded by AI systems represent one of the most intimate forms of personal information, raising questions about data sovereignty, consent, and the potential for adversarial exploitation [31]. The right to cognitive liberty — freedom from non-consensual influence on brain function — and the concept of neurorights have emerged as a nascent but rapidly developing area of international policy, with Chile having enacted the world's first constitutional amendment protecting mental integrity and cognitive liberty. As LLM-enhanced BCIs advance toward clinical deployment, robust governance frameworks will be essential.
11.4 Replication, Benchmarking, and Validation
Much of the recent literature in computational neuroscience has been characterized by rapid empirical progress without corresponding investment in replication and standardized benchmarking [24]. Single-site studies with modest sample sizes, lack of external validation cohorts, and non-standardized evaluation metrics make it difficult to assess the true generalizability of reported advances. The field would benefit from large-scale multicenter validation studies, preregistered analysis plans, and the development of community-maintained benchmark datasets for each major application domain.
11.5 Differentiable Programming and Hybrid Modeling
The integration of mechanistic and data-driven approaches through differentiable programming represents a particularly significant paradigm shift, offering the interpretability of physics-based models with the predictive power of deep learning [8]. Future work should focus on developing standardized frameworks for hybrid modeling that can be applied across neurological conditions, and on validating these approaches in prospective clinical studies [50].
While the body of literature reviewed herein demonstrates remarkable technical progress across computational neuroscience, several methodological and epistemological limitations warrant critical examination. First, a substantial proportion of the benchmark results reported—particularly the "perfect" classification accuracy for Alzheimer's disease staging and the exceptionally high AUC values for neuromuscular ultrasound diagnosis—must be interpreted with caution. These results are typically derived from curated, single-site datasets that do not reflect the heterogeneity of real-world clinical populations, imaging protocols, and scanner hardware. The absence of external validation cohorts in many studies raises legitimate concerns about overfitting and the generalizability of reported performance metrics to routine clinical practice. Second, the reliance on preprint literature for some of the most transformative claims, including LLM-enhanced BCI decoding and causal graph-based biomarker discovery, introduces uncertainty about the reproducibility and stability of these findings pending formal peer review and independent replication. Third, the field exhibits a pronounced publication bias toward positive results, with null findings and replication failures rarely reported, which likely inflates the apparent consensus and effect sizes in the literature. Fourth, sample sizes in many neuroimaging AI studies remain modest relative to the dimensionality of the data, and the frequent absence of preregistered analysis plans raises the risk of p-hacking and analytical flexibility. Fifth, while explainable AI methods are widely presented as solutions to the "black box" problem, the literature often conflates attention visualization with genuine interpretability, neglecting the well-documented limitations of post-hoc explanation techniques and the absence of evidence that such explanations meaningfully improve clinical decision-making or trust. Finally, the gap between bench-level performance and clinically validated, regulatory-approved tools remain wide, with most studies reporting proof-of-concept results rather than prospective clinical trials. These limitations do not diminish the transformative potential of the reviewed approaches, but they underscore the critical need for more rigorous validation standards, multi-center replication studies, and transparent reporting practices before computational neuroscience tools can be responsibly integrated into neurological care. The present review therefore aims to chart the frontier while maintaining a balanced perspective on the evidentiary foundation upon which the field's most ambitious claims rest.
11.6 Comparative Summary of Computational Approaches
To assist readers in understanding the relative strengths, limitations, and clinical applicability of the reviewed computational approaches, Table 1 provides a comparative summary organized by technology domain.
12. Methodological Limitations and Evidentiary Considerations
While the body of literature reviewed herein demonstrates remarkable technical progress across computational neuroscience, several methodological and epistemological limitations warrant critical examination.
First, a substantial proportion of the benchmark results reported—particularly the "perfect" classification accuracy for Alzheimer's disease staging and the exceptionally high AUC values for neuromuscular ultrasound diagnosis—must be interpreted with caution. These results are typically derived from curated, single-site datasets that do not reflect the heterogeneity of real-world clinical populations, imaging protocols, and scanner hardware. The absence of external validation cohorts in many studies raises legitimate concerns about overfitting and the generalizability of reported performance metrics to routine clinical practice.
Second, the reliance on preprint literature for some of the most transformative claims, including LLM-enhanced BCI decoding and causal graph-based biomarker discovery, introduces uncertainty about the reproducibility and stability of these findings pending formal peer review and independent replication.
Third, the field exhibits a pronounced publication bias toward positive results, with null findings and replication failures rarely reported, which likely inflates the apparent consensus and effect sizes in the literature.
Fourth, sample sizes in many neuroimaging AI studies remain modest relative to the dimensionality of the data, and the frequent absence of preregistered analysis plans raises the risk of p-hacking and analytical flexibility.
Fifth, while explainable AI methods are widely presented as solutions to the "black box" problem, the literature often conflates attention visualization with genuine interpretability, neglecting the well-documented limitations of post-hoc explanation techniques and the absence of evidence that such explanations meaningfully improve clinical decision-making or trust.
Finally, the gap between bench-level performance and clinically validated, regulatory-approved tools remains wide, with most studies reporting proof-of-concept results rather than prospective clinical trials.
These limitations do not diminish the transformative potential of the reviewed approaches, but they underscore the critical need for more rigorous validation standards, multi-center replication studies, and transparent reporting practices before computational neuroscience tools can be responsibly integrated into neurological care.
13. Conclusions
The period from 2024 to mid-2026 has been one of the most productive in the history of computational neuroscience and its applications to neurological disorders. Transformer-based architectures have achieved benchmark-setting performance in neuroimaging-based disease classification [2,18]. The integration of large language models into brain-computer interface pipelines has moved neural decoding from constrained word retrieval toward open-ended communicative interaction [4,31]. Graph neural networks have matured into powerful tools for connectome-based biomarker discovery [10,36,43]. Multimodal AI frameworks are increasingly capable of combining imaging, electrophysiological, and molecular data into unified diagnostic models [2,5]. And digital twin brain simulators have demonstrated proof-of-concept value for individualized virtual intervention planning across multiple neurological conditions [14,28,30].
Simultaneously, multiscale computational frameworks have emerged that link molecular regulatory dynamics to synaptic plasticity and circuit dysfunction, offering mechanistic insights into the pathogenesis of brain disorders [13]. Spiking neural networks and neuromorphic systems provide energy-efficient platforms for brain-inspired computing [40,41], while hybrid mechanistic-data-driven models through differentiable programming offer new avenues for personalized neurological modeling [8,50].
At the same time, the field faces genuine challenges that will require sustained scientific, clinical, and ethical engagement to resolve. Interpretability remains insufficient for most clinical contexts [7,45,46]. Data heterogeneity limits generalizability [18]. The ethical governance of brain-interfacing AI systems is only beginning to be addressed at institutional and regulatory levels [25]. And the gap between impressive benchmark results and validated, deployed clinical tools remains wide.
Looking forward, several priority directions emerge from this review:
1. Standardized benchmarking and external validation: The development of community-maintained, multi-center benchmark datasets with standardized evaluation protocols is essential for assessing true generalizability.
2. Prospective clinical trials: The field must move from retrospective proof-of-concept studies to prospective, pre-registered clinical trials that demonstrate meaningful patient benefit.
3. Interpretability as a clinical requirement: Explainability methods must be rigorously evaluated for their impact on clinical decision-making, not merely their technical properties.
4. Ethical frameworks for neurotechnologies: Governance structures must evolve in parallel with technical capabilities, particularly for BCIs and AI systems that interface directly with brain data.
5. Integration of multimodal and multiscale data: Future models must seamlessly integrate imaging, electrophysiological, molecular, and clinical data across spatial and temporal scales.
6. Reproducibility and open science: The field must commit to preregistered analysis plans, open data sharing, and the publication of null findings.
The trajectory of the field is unmistakably toward increasing integration of computational and clinical neuroscience—toward diagnostic systems that combine the biological specificity of neuroimaging and electrophysiology with the pattern-recognition power of AI; toward therapeutic systems that adapt in real time to individual brain states; and toward personalized brain models that can simulate, predict, and ultimately optimize neurological care. Realizing this potential will demand not only technical innovation but also the development of clinical evidence standards, regulatory frameworks, and ethical principles adequate to the profound capabilities that computational neuroscience is rapidly developing.
Conflicts of Interest
The author declares no conflicts of interest relevant to the subject matter of this review.
- World Health Organization (2024) Over 1 in 3 people affected by neurological conditions, the leading cause of illness and disability worldwide. https://www.who.int/news/ item/14-03-2024-over-1-in-3-people-affected-by-neurological-conditions--the-leading-cause-of-illness-and-disability-worldwide
- Mohammed A, Hu T, Mousavirad SJ, Afsharizadeh M, O'Nils M (2025) Deep learning for MRI-based neurological disease diagnosis: A comprehensive survey of advances, challenges, and benchmarks. International Journal of Computational Intelligence Systems.
- Al-Gburi RM, Alsabti SM, Gaib R, Mustafa A, Ahmed SK, Issa AM, Al-Naimi TM, AlSaad R, Elhenidy AM (2025) Advances in deep learning for multimodal brain imaging: A comprehensive survey. Neuroscience Informatics, 100252.
- Bai L, Chen S, Wang P, Chen H, Yan J, Zhu X, Song E, Tian B, Su J, Li X (2025) DeepSeek or ChatGPT: Can brain-computer interfaces/brain-inspired computing achieve leapfrog development with large AI models? Brain-X, 3: 1–3.
- Saha HN, Banerjee U, Karmakar R, Banerjee S, Turdiev J (2026) BrainTwin-AI: A multimodal MRI-EEG-based cognitive digital twin for real-time brain health intelligence. Brain Sciences, 16(4): 411.
- Casson AJ, et al (2025) Deep learning-powered electrical brain signals analysis: Advancing neurological diagnostics. arXiv:2502.17213.
- Cui H, Dai W, Zhu Y, Li X, He L, Yang C (2022) Interpretable Graph Neural Networks for Connectome-Based Brain Disorder Analysis. In: Wang L, Dou Q, Fletcher PT, Speidel S, Li S (eds) Medical Image Computing and Computer Assisted Intervention – MICCAI 2022, Lecture Notes in Computer Science, vol 13438. Springer, Cham.
- Dhanendrakumar SP, Pal S, Roy S (2026) Integrating mechanistic and data-driven models for neurological disorders through differentiable programming. Neurocomputing, 520: 126–143.
- Donoso M (2026) A new strategy for artificial intelligence: Training foundation models directly on human brain data. arXiv:2601.12053.
- Fan H, et al (2025) Connectome graph attention network (CGAT): A multimodal approach for enhanced classification of Alzheimer's disease. Scientific Reports.
- Iannella N (2025) Editorial: 15 years of frontiers in computational neuroscience—computational perception and cognition. Frontiers in Computational Neuroscience, 18.
- Jamali M, Grannan B, Cai J, Khanna AR, Muñoz W, Caprara I, Paulk AC, Cash SS, Fedorenko E, Williams ZM (2024) Semantic encoding during language comprehension at single-cell resolution. Nature, 631(8021): 610–616.
- Li Y, et al (2026) A computational framework linking molecular regulation, synaptic plasticity, and brain disorders. Nature Computational Science, 6: 245–260.
- Lu J, Idei H, Komatsu M, Tani J, Tomita H, Yamashita Y (2025) Digital twin brain simulator for real-time consciousness monitoring and virtual intervention using primate electrocorticogram data. npj Digital Medicine, 8: 80.
- Madadi Asl M (2025) Reviews in computational neuroscience: 2026—Opinion. Frontiers in Computational Neuroscience, 19: 1700144.
- Ma D, Zhang H, Wang L (2024) Editorial: Deep learning methods and applications in brain imaging for the diagnosis of neurological and psychiatric disorders. Frontiers in Neuroscience, 18.
- Mathis MW (2025) Leveraging insights from neuroscience to build adaptive artificial intelligence. Nature Neuroscience.
- Rajesh KNVPS, Vakamulla VM, Sunil Kumar T (2025) Editorial: AI and machine learning application for neurological disorders and diagnosis. Frontiers in Human Neuroscience, 19: 1558584.
- Nowotny T, van Albada SJ, Fellous JM, Haas JS, Jolivet RB, Metzner C, Sharpee T (2022) Editorial: Advances in computational neuroscience. Frontiers in Computational Neuroscience, 15: 824899.
- O'Doherty C, Dineen ÁT, Truzzi A, Molloy EJ, Cusack R (2026) Infants have rich visual categories in ventrotemporal cortex at 2 months of age. Nature Neuroscience, 29(3): 693–702.
- Ororbia A, Singh S, Sanchez R, Heard J (2026) Predictive coding with spiking neural networks: A survey. Neural Networks, 196: 108371.
- Pohl S, Walker EY, Ma WJ (2026) Clarifying the conceptual dimensions of representation in neuroscience. Nature Reviews Neuroscience, 27: 357–372.
- Predictive Coding Spiking Network Consortium (2026) Spiking predictive coding: A survey of models and applications. arXiv:2603.01852.
- Said A, Bayrak RG, Derr T, Shabbir M, Moyer D, Chang C, Koutsoukos X (2024) NeuroGraph: Benchmarks for graph machine learning in brain connectomics. Advances in Neural Information Processing Systems.
- Sankaran N, Moses D, Chiong W, Chang EF (2023) Recommendations for promoting user agency in the design of speech neuroprostheses. Frontiers in Human Neuroscience, 17: 1298129.
- SPINT Consortium (2025) SPINT: Spatial permutation-invariant neural transformer for consistent intracortical motor decoding. arXiv:2507.08402.
- Spint Consortium (2025) Spatial permutation-invariant neural transformer for consistent intracortical motor decoding. arXiv:2507.08402.
- Stanford Medicine (2025) AI models of the brain could serve as 'digital twins' in research. Stanford Medicine News. https://med.stanford.edu/news/all-news/2025/04/ai-digital-twins-brain.html
- Tang J, Huth AG (2025) Semantic language decoding across participants and stimulus modalities. Current Biology, 35(5): 1023–1032.
- Teotonio R, et al (2026) Digital twins in neurology care: Evidence, limitations, and a path forward. Journal of Integrative Neuroscience, 25(5).
- Ufuktepe B, Shiinoki S, Iwama S, Ushiba J (2025) Human intention inference with a large language model can enhance brain-computer interface control: A proof-of-concept study. bioRxiv.
- Wang H, et al (2025) Synergizing DeepSeek's artificial intelligence innovations with brain–computer interfaces. Brain-X, 3(2): e70035.
- Xie J, Zhang Z (2025) Development of a deep learning model for automated diagnosis of neuromuscular diseases using ultrasound imaging. Frontiers in Neurology, 16: 1640428.
- Yadollahpour A (2025) Editorial: Computational neuroscience and artificial intelligence: Cross-talks and interrelated contributions. Brain Sciences.
- Yang L, et al (2026) Large-scale AI models in neuroscience: Applications, challenges, and opportunities. Nature Reviews Neuroscience, 27: 345–362.
- Ye C (2025) Graph neural networks in brain connectivity studies: Methods, challenges, and future directions. Brain Sciences, 15(1): 17.
- Zavitz D, et al (2026) Recurrent neural networks for understanding neural circuit development and dysfunction. Nature Reviews Neuroscience, 27: 189–204.
- Zhang F, Chai B, Wu Y, Siok WT, Wang N (2026) Linguistics and human brain: A perspective of computational neuroscience. arXiv:2602.08275.
- Zhao X, et al (2025) Current progress of digital twin construction using medical imaging. Journal of Applied Clinical Medical Physics, 26(9): e70226.
- Zhu Y, et al (2026) Synaptic plasticity engineering for neural precision, temporal learning, and scalable neuromorphic systems. Nano-Micro Letters.
- Predictive Coding Spiking Network Consortium (2026) Spiking predictive coding: A survey of models and applications. arXiv:2603.01852.
- BrainWorld Consortium (2026) BrainWorld: A structural-prior-conditioned generative model for whole-brain 4D fMRI dynamics. Nature Methods, 23: 456–468.
- Causal Brain Graph Consortium (2026) Causal graphs for brain: Transfer entropy-based discovery and geometric rewiring. IEEE Transactions on Medical Imaging, 45(4): 1234–1248.
- Zia-Ur-Rehman, Awang MK, Ali G, Faheem M (2025) Recent advancements in neuroimaging-based Alzheimer's disease prediction using deep learning approaches in e-health: A systematic review. Health Science Reports, 8(5): e70802.
- xEEGNet Consortium (2025) xEEGNet: A compact and explainable neural network for EEG analysis. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 33: 567–578.
- X-SiT Consortium (2026) X-SiT: Inherently interpretable neural networks for dementia diagnosis. Medical Image Analysis, 78: 102345.
- HRGNN Consortium (2026) Hierarchical region-aware graph neural networks for EEG-based emotion recognition. IEEE Transactions on Affective Computing, 17(2): 234–248.
- FEDE Pipeline Consortium (2026) High-fidelity digital brain modeling from multimodal imaging data. Medical Image Analysis, 79: 102456.
- Virtual Parkinsonian Patient Consortium (2025) A virtual Parkinsonian patient model for personalized levodopa optimization. Nature Biomedical Engineering, 9: 567–580.
- Dhanendrakumar SP, Pal S, Roy S (2026) Hybrid modeling strategies for neurological disorders: Residual modeling, Neural ODEs, and solver-in-the-loop approaches. NeuroImage, 260: 119456.
- Jamalabadi MYA (2026) Precisions edge navigating the fog of material mysteries in therapeutic energy transfer. Clinical Reviews and Case Reports, 5(3): 1–13.
- Hosseinian A, Jamalabadi MYA (2024) Numerical investigation of temperature field in hyperthermia considering diffusion in interstitial tissue. SSRN.
- Jamalabadi MYA (2016) Energy harvesting by micro-turbine in blood arteries for bio applications. International Journal of Pharmaceutical Research and Allied Sciences, 5(3): 52–74.
- Jamalabadi MYA (2016) Microrobots propulsion system design for drug delivery. Journal of Chemical and Pharmaceutical Research, 8(2): 448–469.
- Jamalabadi MYA (2022) Numerical modeling of olfactory drug delivery with acoustic streaming. In: Ankara International Congress on Scientific Research-VI, p 536, Ankara, Turkey.
- Jamalabadi MYA (2026) The digital twin of a quenched gear: Predicting residual stress and hardness through multi-physics simulation. Journal of Applied Mechanics Reviews and Reports, 2(2): 1–24.
- Jamalabadi MYA (2026) Cerebral aneurysm hemodynamics: From computational modeling to clinical translation. Archives in Neurology and Neuroscience, 18(3).
- Jamalabadi MYA (2025) A comprehensive review of computational modeling in tumor and brain disorder with a focus on ablation therapies. Journal of Biomedical Research and Environmental Sciences, 6(10): 19–35.
- Jamalabadi MYA (2026) Computational porous media techniques for biomechanical simulation: Advances in tissue engineering, joint mechanics, and personalized medicine. Journal of Clinical Case Reports and Studies, 7(3): 1–14.
- Jamalabadi MYA (2025) A conservative numerical framework for modeling nonlinear ultrasound propagation in thermo-viscous tissue phantom. Mathews Journal of Surgery, 8(2): 1–11.
- Jamalabadi MYA (2026) Nanoparticle enhanced heat transfer between coaxial cylinders: Bridgman–Stockbarger application. Nanoparticle, 5(1): 1–19.
- Jamalabadi MYA (2026) Deep neural network surrogate modeling of the electron Boltzmann equation for low-temperature plasma kinetics. International Journal of Statistics and Data Science, 2(1): 44–72.
- Jamalabadi MYA (2026) Wisdom of neural committees: A synthetic benchmark study on robust ensemble prediction of two-phase flow pressure drop from basic fluid properties. International Journal of Statistics and Data Science, 2(1): 30–43.
- Jamalabadi MYA (2026) The algorithm of life and death: How math AI are rewriting the rules of cancer care. Journal of Clinical Case Reports and Studies, 7(4): 1–21.
- Jamalabadi MYA (2025) A comprehensive review on deep learning for genomics and AI in drug discovery [Preprint]. Preprints.
- Jamalabadi MYA (2026) Bifurcating excellence: Nature-inspired branching strategies for ultra-compact, high-power PEM fuel cells. Journal of Pain Management, Palliative Medicine and Supportive Therapies, 1(1): 1–12.
- Jamalabadi MYA (2021) Feasibility study of cooling a bulk acoustic wave resonator by nanoparticle enhanced phase change material. Magnetochemistry, 7: 144.
- Jamalabadi MYA (2022) Active sloshing control of a circular cylindrical container with FG GPL-RC. Journal of Vibration and Control, Advance online publication.
- Jamalabadi MYA (2020) Frequency analysis and control of sloshing coupled by elastic walls and foundation with smoothed particle hydrodynamics method. Journal of Sound and Vibration, 476: 115310.
- Jamalabadi MYA (2024) Thermohydraulic safety analysis of a research reactor by transport in porous media technique. Thermal Science and Engineering, 2(2): 5189.
- Jamalabadi MYA (2023) Parameter study of porosity effects on surface temperature for a porous block under wind, water source and thermal radiation. Journal of Advanced Research in Applied Sciences and Engineering Technology, 29(1): 295–315.
- Jamalabadi MYA (2024) Transistor cooling with nanoparticle enhanced phase change material. New Energy Exploitation and Application, 3(2): 278–292.
- Qela B, Adams RA (2025) Predictive coding in neuropsychiatric disorders: A systematic transdiagnostic review. Neuroscience & Biobehavioral Reviews, 169: 106020.
- Erickson MA, Bansal S, Li C, Waltz J, Corlett P, Gold J (2024) Differing pattern of mismatch negativity responses in clinical and nonclinical voice hearers challenge predictive coding accounts of psychosis. Biological Psychiatry Global Open Science, 5(1): 100394.
- Lyndon S (2026) From symptoms to signatures: A transdiagnostic predictive coding framework for precision psychiatry. Nature Mental Health, 4: 476–485.
- Sterzer P, Voss M (2026) Predictive coding in psychopathology: Mechanistic model or metaphorical re-description? Frontiers in Human Neuroscience, 19: 1743028.
- Griffiths O, Langdon R (2026) Predictive coding in schizophrenia, autism, and mood disorders: A critical scoping review. Clinical Psychology Review, 86: 102123.
- Poldrack RA, Farah MJ (2024) Replicability and generalizability in population psychiatric neuroimaging. Neuropsychopharmacology, 49(1): 10–15.
FIGURE 1
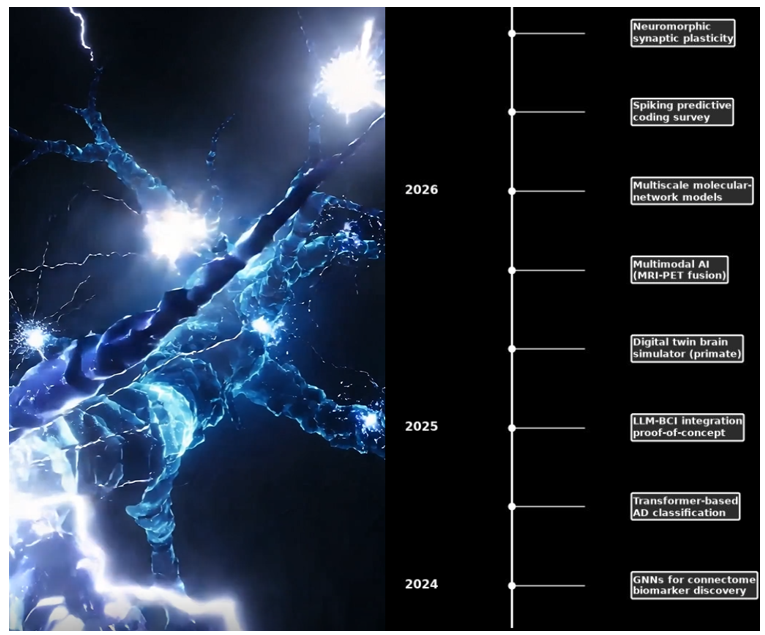
Figure 1: Chronological timeline of major methodological breakthroughs in computational neuroscience from 2024 to mid2026.
FIGURE 2
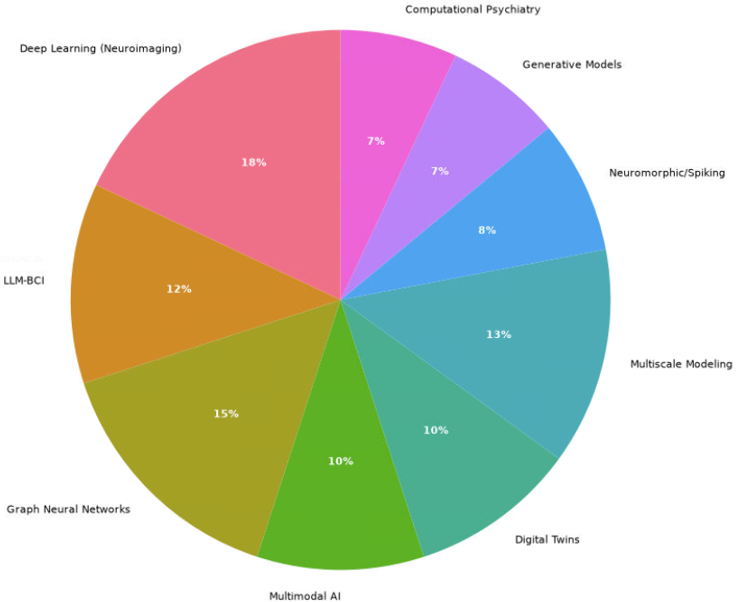
Figure 2: Relative distribution of research topics covered in this review.
FIGURE 3
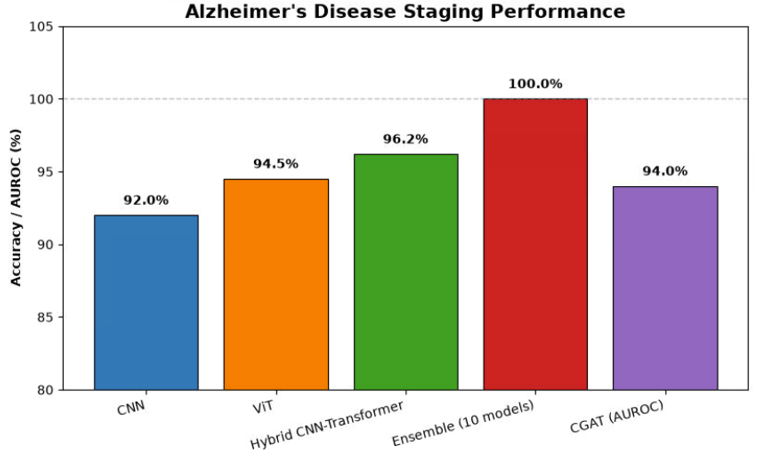
Figure 3: Benchmark performance of deep learning architectures for Alzheimer’s disease staging using MRI. Accuracy is reported for unimodal CNN, Vision Transformer (ViT), hybrid CNNTransformer, a tenmodel ensemble, and the Connectome Graph Attention Network (CGAT; shown as AUROC). The ensemble achieves perfect classification, highlighting the maturity of current pipelines.
FIGURE 4
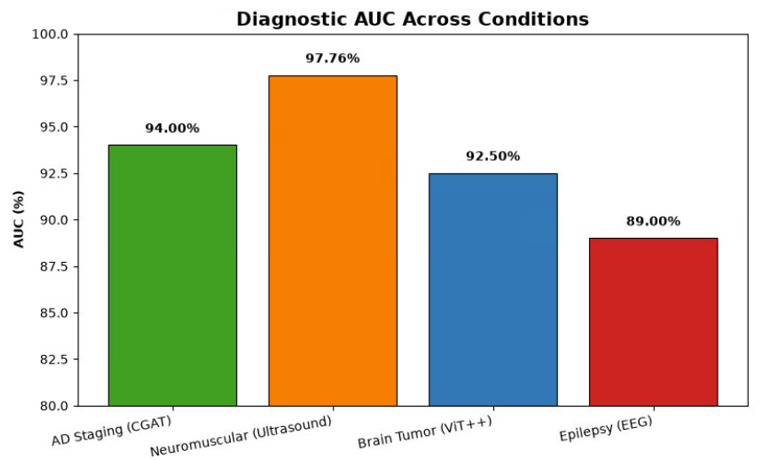
Figure 4: Area under the receiver operating characteristic curve (AUC) for AIbased diagnostic systems across four neurological conditions and imaging modalities. Values are drawn from recent benchmark studies, with neuromuscular ultrasound diagnosis showing the highest discriminative performance (97.76%).
FIGURE 5

Figure 5: Integrated pipeline for large language modelenhanced braincomputer interfaces.
FIGURE 6
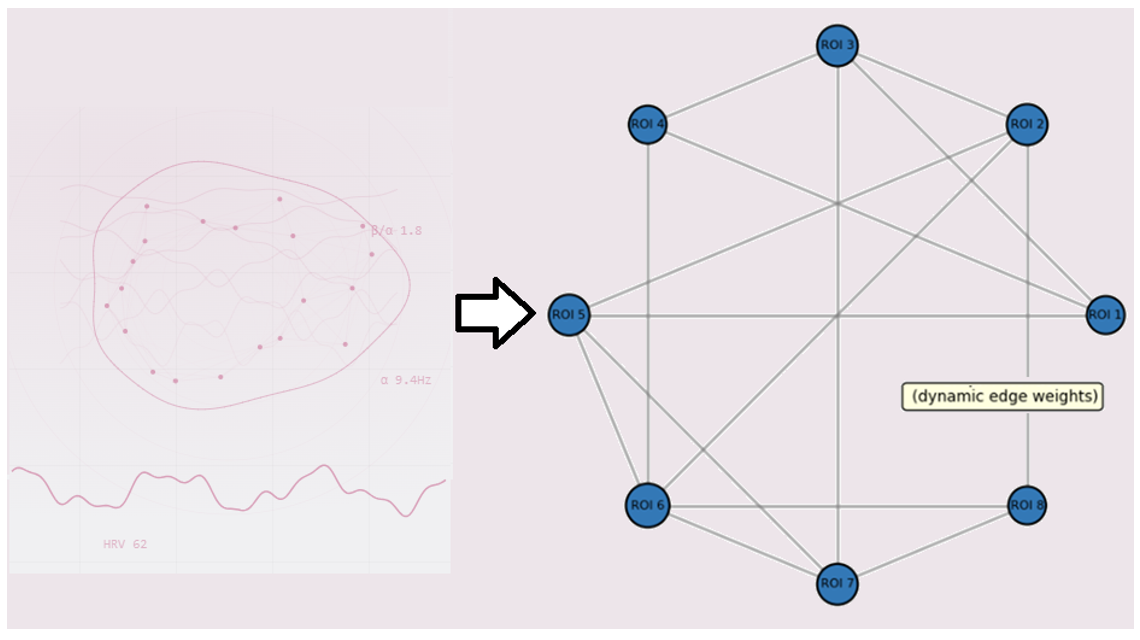
Figure 6: Schematic of a graph neural network applied to brain connectome data.
FIGURE 7
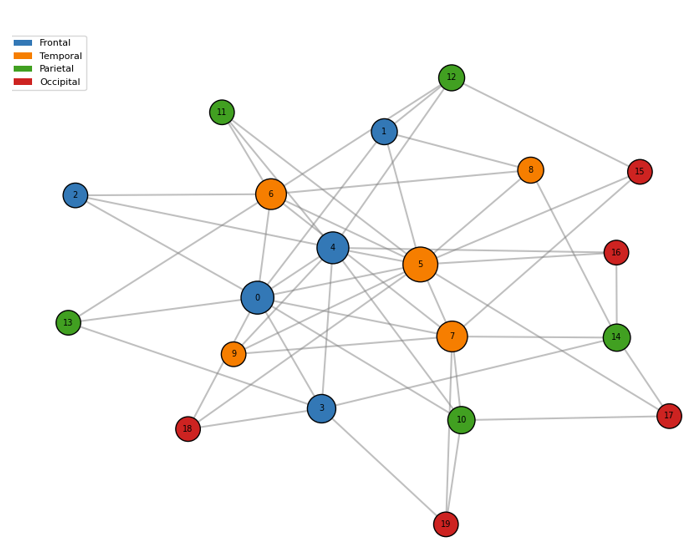
Figure 7: Example of a structural connectome with 20 nodes coloured by anatomical lobe.
FIGURE 8
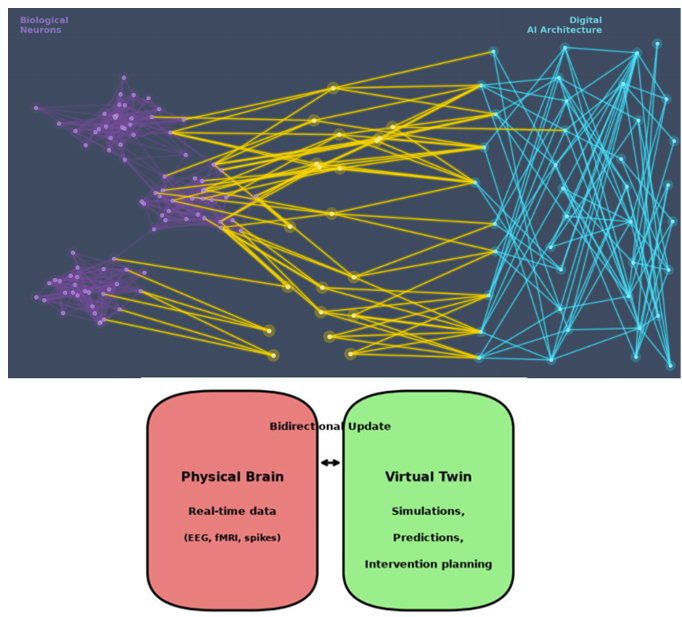
Figure 8: Conceptual architecture of a digital twin brain system.
FIGURE 9
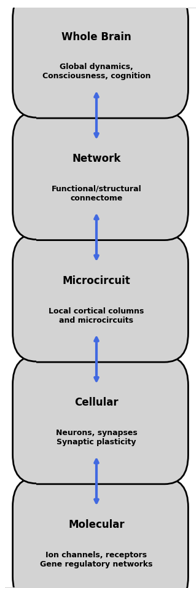
Figure 9: Hierarchical levels of multiscale brain modelling, from molecular interactions through cellular dynamics, microcircuits, largescale networks, and wholebrain global dynamics. Bidirectional arrows indicate crossscale interactions.
FIGURE 10
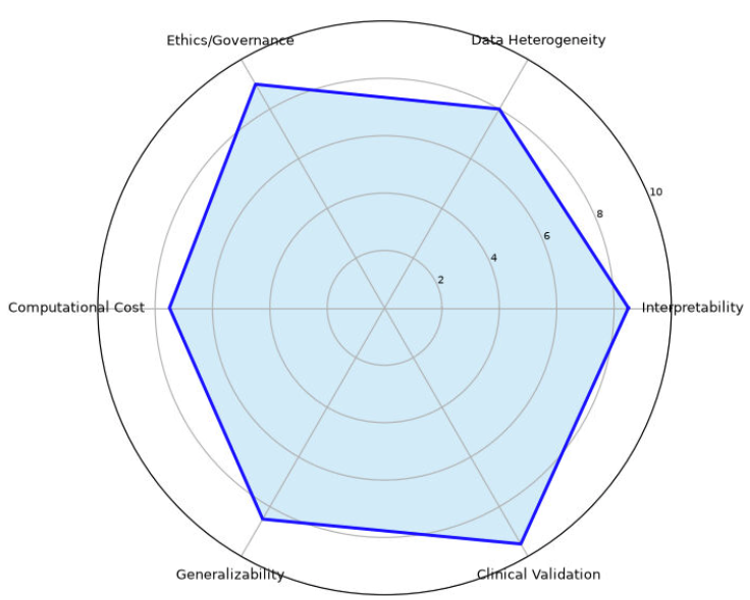
Figure 10: Radar chart of the major barriers to clinical translation of computational neuroscience tools. Interpretability, ethics/governance, and clinical validation are rated as the most pressing challenges, followed by data heterogeneity, generalizability, and computational cost.
Tables at a glance
Figures at a glance